|
Algorithm for Management of Radiation-Induced Cutaneous Damage (Acute and Late Effects)
|
TREATMENT
Overview
This topic covers management of radiation-induced cutaneous damage, including treatment, prevention and a section for clinicians on patient education. For an introduction and assessment of this condition including epidemiology, risk factors, etiology, pathophysiology, history, physical examination, diagnosis, differential diagnoses, documentation and ICD-10 coding, see "Radiation-induced cutaneous damage - Introduction and Assessment". For hyperbaric oxygen treatment indications and protocol related to radiation-induced cutaneous ulcer see "Soft Tissue Radionecrosis".
Classification
Radiation-induced cutaneous damage can be classified as acute, consequential-late, chronic (also known as late), or other less common forms of radiation damage.[3]
-
Acute effects: present within 90 days of exposure and range from mild erythema and hyperpigmentation to severe desquamation and ulceration. Acute damage can also be caused by radiation burns and fluoroscopy.[19][20]
-
Late effects (i.e. chronic reactions): present after more than 90 days after exposure. It is both progressive and irreversible - unlike acute damage, which typically peaks and then resolves unless severe.[1][3][21] Ulceration is a common finding in chronic damage, in addition to fibrosis, telangiectasia, lymphedema, and necrosis.[13]
-
“Consequential-late”: If severe acute toxicity does not heal, it can result in clinical manifestations similar to those of chronic reactions such as fibrosis and ulceration, but are mechanistically similar to the acute process. This “consequential-late” damage is most common in the gastrointestinal and bladder mucosa, as well as the epidermis, which are particularly sensitive to disruption of the epithelium.[22] Consequential-late cutaneous non-healing ulcers may undergo malignant transformation.[1]
-
Less common forms of radiation damage include: eosinophilic, polymorphic, and pruritic eruption (EPPER), as well as radiation recall reaction.[23][24]
Treatment for each of the specific conditions above is detailed in this topic and summarized in the algorithm below (Algorithm 1)
Algorithm 1. Algorithm for Management of Radiation-Induced Cutaneous Damage - Acute and Late Effects
Acute effects
There is a paucity of consensus in management of acute radiation-induced cutaneous damage.[2][25] Lucey et al. conducted a survey of 709 members of the American Society for Radiation Oncology and found that 89 percent of physician respondents employed anecdotal evidence or observational findings to determine treatment strategies, and 51.4 percent used evidence-based therapies.[26]The few modalities that have repeatedly demonstrated effectiveness are presented here.
Management may be guided by staging either with the CTCAE 4.03 or RTOG/EORTC scales. Conservative measures with general skin care practices and washing are the first line, with increasing interventions for more advanced stages. The presence of advanced symptoms, moist desquamation, ulceration, necrosis, may necessitate cessation of radiotherapy until the wound has been stabilized. Most of these patients will require pain control, which should follow the WHO analgesic ladder.[27]
Treatment goals
The primary objective in treatment of acute radiation-induced cutaneous damage is to limit and/or repair current injury and to prevent further damage.
General skin care for all patients undergoing radiotherapy
After treatment, care should be taken to prevent further damage to the skin. See details in ‘Prevention’ below. Briefly:
- Patients should be advised to avoid irritants such as excessive friction by wearing loose-fitting, cotton clothing.[28]
- Sun exposure can also compound the damage and should be avoided for the duration of treatment. Sunscreen with UVA and UVB protection should always be worn.[1][7][28]
- Moisturizers should be avoided at least one hour before treatment as they can cause a bolus effect that enhances cutaneous radiation damage.[4] [7][29][8][30]
Management of acute radiation injuries by CTCAE 4.03 severity grading
Grade 1 injuries: mild to moderate erythema with dry desquamation.
- These patients often require no specific treatment other than routine skin care as outlined above. For patients with symptomatic desquamation, a hydrophilic, unscented, topical emollient can provide relief. Pruritus and irritation can be treated with a mild corticosteroid.[1][2][4][5]
Grade 2-3 injuries: tender erythema, moist desquamation that extends beyond intertriginous areas (grade 3), edema, and bleeding
- These symptoms may require cessation of radiotherapy. Moist desquamation increases susceptibility to infection and causes frequent drainage, which necessitate wound coverage with dressings.
-
Local care of moist desquamation: systematic reviews and guidelines recommend the use dressings that promote a moist wound environment to facilitate healing.[6][7][8][31] For customized, wound-specific recommendations, use the "Wound Prep and Dress Tool". For practical information on dressing indications, contraindications, application, Medicare coverage and brands see tool "Dressing Essentials". General recommendations regarding dressings for radiation-induced acute damage are listed below:
-
- As for choice of dressings, there is insufficient evidence to recommend one type over another.[9] Hydrogels, hydrocolloid, semipermeable transparent films, and non-adherent foams are frequently used in practice.[2][4][7][8][30] A randomized controlled trial [32] found an increased time to heal when using hydrogel compared to dry dressings. However, a systematic review [33] found mixed evidence in healing time when comparing hydrogel, hydrocolloid to other alternatives. Nevertheless, the review and other authors mentioned that hydrogel and hydrocolloid may improve patient comfort compared to other alternatives.[7][33]
- Infection: If the affected skin becomes infected, it should be treated with either topical with or without systemic antibiotic therapy, depending on severity of infection.
-
2BFor patients undergoing radiotherapy and at high-risk of acute radiation injuries, clinicians might opt to have patients apply silver sulfadiazine cream 1% (SSD 1%) to prevent radiation-induced skin injury compared with general skin care alone (Grade 2B). Expert panel suggests routine use of SSD 1% to treat already established acute radiation injuries grades 2 or 3.[8]
-
- Clinical guideline [9] suggests use of silver sulfadiazine cream 1% compared with skin care alone to prevent or decrease severity of acute radiation injuries. This suggestion is based on a single randomized controlled trial (RCT) [34] of moderate level of certainty (evidence level B) that concluded that silver sulfadiazine cream 1% three times a day, 3 days a week, for 5 weeks during radiotherapy and one week thereafter reduced the severity of radiation-induced skin injury compared with general skin care alone.
- An expert consensus [8] suggested use of silver sulfadiazine after radiotherapy for injuries grades 2 and 3, possibly in the evening, after cleaning the irradiated area, to promote healing. However no RCTs were cited to support recommendation. A small, underpowered RCT [35] concluded that silver-leaf nylon dressings were more effective than silver sulfadiazine cream at reducing the severity of reaction within the same acute injury grade.
- Silver sulfadiazine has potential side effects that include rash, skin discoloration, photosensitivity, hypersensitivity reactions, and treatment protocol may disrupt patients’ routine due to the need to apply treatment 3 times a day. This medication is not routinely covered by Medicare for this purpose and may need to be purchased by patient at list price. For these reasons, we suggest that this protocol be reserved as an option for patients at high-risk for acute radiation injuries.
Grade 4 injuries: ulceration, full thickness necrosis, invasion of subcutaneous tissue and underlying bone.
- These wounds require cessation of radiotherapy and a multidisciplinary team comprising of oncology, dermatology, nursing, and wound care.
- Local wound care as described above for grade 2-3 injuries may be followed.
- Radiation-induced cutaneous damage manifested as ulcers or necrosis that occasionally do not heal are called consequential late changes of acute dermatitis, and have potential for malignant transformation.[1]
- Advanced injuries may require surgical debridement, reconstruction with skin grafting and myocutaneous flaps, or amputation.[1][8]
Follow-up and prognosis
- Most acute radiation-induced cutaneous damage persist during radiotherapy but are expected to heal, with mild cutaneous changes.[1]
- Closer follow-up and monitoring is recommended for more severe acute effects (CTCAE 4.03 Grade 2 or greater)
- Prompt investigation and intervention is required if signs of infection arise (e.g, inflammation, swelling or tenderness beyond radiated field, purulent discharge or malodorousness).[30]
Other interventions
While there are myriad other therapies currently in use for symptom reduction, there is a dearth of high-powered, randomized control studies that would allow for a conclusive answer as to their use.
- Chan et al.[28] performed a systematic review and meta analysis of therapies used to treat acute radiation injuries and found insufficient evidence to recommend treatment with the following agents:
-
- Oral systemic pentoxifylline, sucralfate, or antioxidant;
- Nonsteroidal therapies including: qingdiyou medication, wheatgrass extract cream, and sucralfate;
- LED treatment;
- Specialized dressings.
- Wong et al.[9] conducted a systematic review with the same aim, and only found sufficient evidence to strongly recommend topical steroids, gentle washing with soap, and antiperspirant use. A strong recommendation was made against use of aloe vera and a weak recommendation was made for use of silver sulfadiazine to reduce breast dermatitis. However, insufficient evidence was found for all of the following:
-
- Topical sulcrate and its derivatives;
- Hyaluronic acid;
- Ascorbic acid;
- Silver leaf dressing;
- LED therapy;
- Theta-Cream;
- Dexpanthenol and calendula;
- Oral proteolytic enzymes; sucralfate; zinc; and pentoxifylline.
- Salvo et al. and Bolderston et al. found similar results in their respective reviews, underscoring the need for continued research so as to determine the definitive therapy for these damages.[2][6]
- Novel investigational interventions to treat acute radiation cutaneous damage include stem cells, growth factors, deferoxamine and low level light therapy. See section on 'Experimental Therapy' below
Uncommon presentations
Radiation recall injury (RRI):
- Cessation of the chemotherapeutic agent usually causes resolution.[24][36]
- Strouthos et al. described a case of docetaxel-induced radiation recall, which responded to topical steroids and systemic antihistamines. Subsequent challenges with docetaxel resulted in very mild reappearance of rash.[37]
- Bourgeois et al. described a case of tamoxifen-induced radiation recall that occurred over four years after cessation of chemotherapy. Treatment with topical 0.1 percent triamcinolone cream twice daily resulted in resolution of symptoms without recurrence. [38]
Eosinophilic, polymorphic, and pruritic eruption (EPPER):
- Antihistamines, topical and systemic corticosteroids, and ultraviolet B radiation have all been successfully used as treatment. Spontaneous resolution has also been described. [23][39]
Chronic effects
As with acute cutaneous toxicity, the treatment of chronic radiation-induced cutaneous damage is lacking in experimentally validated and reproducible data. The majority of current treatment regimens are based on experience and extrapolation from existing general wound care guidelines.[1][13] Unlike acute injuries, the staging of chronic wounds is not emphasized in published clinical guidelines. This may be due to the fact that the manifestations of chronic radiation damage are more disparate than the acute variety, which follows a continuum. Instead, treatment is split up into presentations with their respective recommendations and regimens.
Treatment Goals
The objective in treatment of chronic radiation-induced cutaneous damage is to limit and repair cutaneous damage to achieve the best possible functional and cosmetic outcome, and improve quality of life.
Ulcers and necrosis
The incidence of ulceration and necrosis have decreased due to improvements in radiotherapy dosage and delivery. However, these complications are not uncommon at specialized centers. As with most radiation injuries, treatment guidelines are lacking and most recommendations lack rigorous validation. In general, experts suggest that simple ulcers be initially treated with active wound care approach, followed by definite wound coverage or adjunctive therapy if the ulcer fails to respond.[12][6][7][8][9][12] Ulcers with exposure of critical underlying structures (e.g., vessels, nerves, etc.), larger ulcers (e.g. greater than 2 cm in diameter), and ulcers with poor blood supply may require implementation of a surgical approach from the start. [16]
Ulcerations in radiation-damaged tissue can be managed with a systematic approach such as the one described below and illustrated in Algorithm 1 above.
-
Rule out malignancy: when treating a non-healing wound due in an irradiated area, recurrence or secondary malignancy must always be considered and a low index of suspicion is required.[1][7][40]
-
Determine wound prognosis: determine if wound is healable or non-healable with conservative treatment, or if co-existing medical conditions/drugs significantly or circumstances hamper wound healing (“maintenance”). See Table 1 below. [10][11]
Table 1. Wound healability and prognosis. (* ) As determined by comprehensive patient assessment. Maintenance wounds have potential to heal, but patient or health system barriers compromise healing (**) For persons without diabetes, inadequate blood supply is objectively confirmed by ankle-brachial index (ABI) < 0.5, monophasic doppler waveform, skin perfusion pressure < 30mmHg, transcutaneous oxygen < 30mmHg, absolute systolic ankle pressure < 50 mmHg OR toe pressure < 30mmHg. For persons with diabetes, perform any other testing listed above besides ABI as ABI can be falsely elevated
| Can underlying cause be treated? |
How is blood supply to the wound? |
Co-existing medical conditions/drugs... |
Then wound prognosis is...
|
| Yes |
Adequate |
Are not an obstacle for healing |
Healable
|
| No (*) |
Adequate |
May or may not prevent healing |
Maintenance
|
| No |
Usually inadequate (**) |
May inhibit healing |
Non-healable |
Modified from Sibbald RG et al. 2011[41]
-
- Healable wounds: may be initially managed with an active wound care approach. Adjunctive therapy is considered if this approach fails.
- Non-healable wounds: wounds are considered non-healable when active wound care approach is likely to fail without correction of underlying cause, optimization of blood supply and adequate bioburden control (e.g., wounds with frequent, recurrent infections that may need oral antibiotics in addition to topical antimicrobials).
-
- Radiation can frequently compromise tissue vasculature and hamper delivery of blood and nutrients needed for wound healing. In these cases, clinicians might opt for referral to plastic surgeon for evaluation of surgical wound coverage. Free flaps or flaps with pedicles originating in non-irradiated areas may represent the best treatment option.
-
- Maintenance wounds: managed with a “non-healable” wound care protocol until co-existing medical conditions/drugs or circumstances that inhibit healing are mitigated. Goal of wound care in the interim is to prevent further deterioration of wound, control bioburden, manage moisture and provide patient comfort.
Treat the cause and factors impeding healing
For all patients (healable, non-healable and maintenance ulcers), cause and factors impeding healing should be addressed. For ulcers caused by late effects of radiation, the main cause has likely been removed, as by definition, late-effect radiation-induced cutaneous damage appears 90 days after radiation exposure. Measures below can also be taken:
- Avoid trauma to the previously irradiated skin, including mechanical trauma such as friction, irritants, extreme heat or cold.
- Address any identified factors that can adversely affect wound healing, such as:
-
- Co-morbidities: uncontrolled diabetes mellitus, skin disorders (such as acne, psoriasis, or atopic eczema) in the irradiated area, obesity
- Medications: immunosuppressants, corticosteroids
- Lifestyle: smoking, impaired mobility, financial constraints
- If new radiotherapy is needed, advanced modalities in radiation delivery are recommended to prevent further radiation damage
Address patient's concerns
For all patients (healable, non-healable and maintenance ulcers), patient's and caregiver's concerns and psychosocial aspects should be assessed and taken in consideration when creating a treatment plan.
- Evaluate psychosocial aspects of the patient, caregiver and family: cognitive, functional, emotional status, understanding of the condition and risk factors, preference for treatment method, motivation for adherence to the care plan, financial concerns
- As with acute radiation cutaneous damage, pain control should follow the WHO analgesic ladder.[27]
Local wound care - Conservative management
For healable wounds, clinicians can implement the interventions below, according to general wound bed preparation principles.[10][11] For customized, wound-specific recommendations, use the "Wound Prep and Dress Tool". For practical information on dressing indications, contraindications, application, Medicare coverage and brands see tool "Dressing Essentials". General recommendations regarding dressings for ulcers caused by late effects of radiation are listed below:
-
Debridement of necrotic tissue:
-
- Non-healing ulcers after radiation exposure are poorly vascularized, thus debridement may need to be done carefully and selectively [1]
- Necrotic tissue can be debrided with conservative sharp debridement, enzymatic or autolytic methods.[1][3] Maggot debridement therapy has also been posited as an alternative technique, but has not been extensively studied in this context.[42]
- For patients who cannot receive conservative sharp debridement (due to logistics or contraindications), clinicians might opt for enzymatic debridement with collagenase (e.g., Santyl).
-
Infection management: Infected wounds, those at high risk of infection or with refractory ulcers can be treated with silver-based dressings or other topical antimicrobials.[1][7] Advanced cases may require surgical debridement.
-
- If concomitant debridement is needed and patient cannot receive conservative sharp debridement, clinicians might opt to alternate a silver topical antimicrobial (e.g., Silvadene) with collagenase (e.g, Santyl).
-
Promotion of moist environment [1]:
-
- Lipophilic and hydrophilic creams can be added to the dressing for comfort.
-
Hydrogel or hydrocolloid dressings may be utilized for ulcers with none to moderate exudate, similar to management of moist desquamation
-
-
Reassessment in 2 to 4 weeks: ulcers that do not show improvement with conservative measures require adjunctive treatments including hyperbaric oxygen therapy, negative pressure wound therapy (if excessive exudate), application of cellular and/or tissue products, or surgical intervention such as surgical debridement and reconstruction with flaps (pedicled/free, cutaneous/myocutaneous).[1][13][43] See sections on 'Plan Reassessment','Surgical Wound Coverage' and 'Adjunctive Therapy'.
For non-healable or maintenance wounds, priority should be given to addressing patient's concerns and providing comfort. For maintenance wounds, ulcers may be debrided conservatively (no bleeding), topical antiseptics (e.g. povidone-iodine) may be used to reduce bioburden, and moisture reduction with non-adherent or more absorptive dressings may be more appropriate. For non-healable wounds, same suggestions are valid, however debridement should be limited to removal of slough only.[11]
Fibrosis
Management of fibrosis is very challenging and requires a multidisciplinary team to achieve the best outcomes.[1] The current mainstays of treatment are: rehabilitation, pharmacotherapy, laser therapy, and surgery:
-
Rehabilitative care consists of tissue mobilization and manipulation, which are both preventative and therapeutic for early stages.[1][13] Bourgeois et al. found a modified massage and skin mobilization technique to decrease pain, erythema, and subjective induration when compared to the control group.[44]
- Pharmacotherapy regimens are frequently used to treat fibrosis despite the lack of definitive evidence for their efficacy:
-
2CClinicians might opt to use pentoxifylline and vitamin E to treat chronic radiation-induced cutaneous damage manifested as cutaneous fibrosis (Grade 2C)
-
- Pentoxifylline (PTX), a methylated derivative of xanthine, is commonly used along with and without the antioxidant tocopherol (vitamin E). PTX is commonly used for its antiplatelet effects, but is also believed to modulate immune response via upregulation of neutrophils, antagonization of tumor necrosis factors -alpha and -ß, and suppression of GM-CSF and IFN-gamma. Additional experiments found that tocopherol may compound these effects by downregulating TGF-ß1 and reversing radiation induced damage to fibroblasts.[1][3] In their clinical guidelines published in 2013, Wong et al. recommended the use of PTX for patients with established cutaneous fibrosis.[9] The question of PTX use remains unsettled as multiple studies have come to conflicting conclusions regarding the efficacy of PTX with or without tocopherol use. [45][46][47] Delanian et al. showed that patients required two years of therapy to achieve the maximal response rate, and those who aborted treatment within a year of initiation actually had an increased risk of fibrosis, indicating that the regimen may require a set period of time to become efficacious.[48] A study that found combined therapy to be successful in reducing fibrosis have employed 400 mg bid up to 1200 mg qd of pentoxifylline and 1000 units of vitamin E qd. [49] PTX side effects include dizziness, gastrointestinal dysfunction [50] and contraindications include intolerance to xanthines (e.g. caffeine, theophylline). PTX should be used with caution in patients taking other antiplatelet regimens.
- Other therapies have shown promising results including liposomal superoxide dismutase [51] and IFN-gamma [52], however larger studies are required to demonstrate their efficacy.
-
Laser therapy in conjunction with skin grafting has been shown to be effective at reversing cutaneous fibrotic changes, but requires more investigation to definitively prove its efficacy.[14]
- Lipotransfer a retrospective analysis with 38 patients concluded that lipotransfer was effective for volume restoration and treatment of scar and radiation-induced fibrosis in irradiated head and neck defects.[15] However stronger evidence in the form of a prospective randomized controlled trial is needed.
-
Surgical intervention can be necessary in cases of advanced, refractory fibrosis or in patients where the damage threatens vital structures. Care must be taken when making the decision whether or not to intervene as further disruption of the tissue can worsen the existing fibrosis.[13] However, in instances such as head and neck cancers, where the involvement of the oropharynx compromises the airway or alimentary tract, reconstruction with free flaps may be necessary.[43]
Telangiectasia
The presence of telangiectasia can be disfiguring and psychologically distressing for the patient. The only modality that has been shown to have some effect is pulse laser dye therapy.[4][13][9] In a comparison between long pulsed dye laser (LPDL) and intermittent pulsed light (IPL), Nymann et al. found that LPDL had increased efficacy and patient satisfaction.[53]
Lymphedema
Typically lymphedema is a sequelae of breast cancer treatment due to lymph node dissection, but it can also be the result of radiotherapy-induced lymphatic disruption, which can occur anywhere in the body.[43][54][55] For earlier stages, conservative measures such as compression garments and weight loss are first line. More advanced stages require surgical interventions such as lymphatic venous anastomosis or vascularized lymph node transfer.[43][54][55]
Postirradiation morphea
Treatment of postirradiation morphea is similar to that of localized scleroderma and consists of phototherapy, intralesional and topical corticosteroids, and immunosuppressive therapy.[56]
Plan Reassessment
Reassessment can be guided by the staging of the radiation-induced cutaneous damage. See topic "Radiation-induced cutaneous damage - Introduction and Assessment"
Acute effects
- More severe acute effects (CTCAE 4.03 Grade 2 or greater) require closer follow-up and monitoring.
- At any time, signs of infection such as fever, inflammation, swelling or tenderness beyond radiated field, purulent discharge or malodorousness of the wound require prompt investigation and intervention.[30]
Late effects (ulcers)
- If radiation-induced ulcers do not show signs of improvement in 4 weeks, the patient/ulcer and treatment plan should be reassessed.
- Evidence of improvement includes measurable changes (decreases) of some of the following:
-
- Drainage
- Inflammation
- Swelling
- Pain
- Wound dimensions (diameter, depth)
- Necrotic tissue/slough
- Medicare and many insurers in the U.S. require a change to the plan of care of ulcers with no signs of improvement in 30 days, which may include physician reassessment of underlying infection, metabolic, nutritional, or vascular problems inhibiting wound healing, or a new treatment modality.
- Chronic, non-healing ulcers that do not respond to conservative therapy should be biopsied to evaluate for secondary malignancy if they have not been already.[1][3][7] If other differential diagnoses have been ruled out and factors impeding healing have been addressed, surgical wound coverage and/or adjunctive therapies may be incorporated into the treatment plan. See sections 'Surgical Wound Coverage' and 'Adjunctive Therapy'.
Surgical Wound Coverage
Indicated for ulcers caused by late effects of radiation with exposure of critical underlying structures (e.g., vessels, nerves, bone), larger size (e.g., >4cm2), with poor blood supply (unlikely to heal with conservative management only), or radiation ulcers (acute or late effects) that failed to show signs of improvement despite adequate wound care for at least 4 weeks.
Skin grafts
- Not recommended for late radiation cutaneous damage due to the microvascular dysfunction and local tissue changes of the recipient area, which result in high failure rates.[57]
Flaps
- Flaps are the preferred method for surgical coverage of radiation wounds. Surgical repair of radiated tissue requires resection of damaged/necrotic tissue followed by coverage with well-vascularized flaps.
- Vascularized free flaps from beyond the radiation bed are often utilized to ensure adequate coverage and healing.[58] The recipient vessel might be difficult to localize in the fibrotic wound bed, in which case long pedicled flaps with vessels outside the zone of radiation will be required.[43]
- Axial musculocutaneous flaps are usually first choice because of intact blood supply versus local random flaps, which may fail for the same reasons that skin grafts do - disrupted microvasculature [16]
- Revascularized free flaps are also good candidates, especially for large wounds that require extensive debridement that compromises axial flaps [16]
-
- Damage to recipient vessels can cause flap necrosis and may require long vessel grafts to achieve successful anastomoses
- Perforator flaps are an alternative to free flap that does not require disruption of large vessels that supply other structures such as muscles and bones [16]
-
- Used for small ulcers where perforator and flap are outside radiation zone
Below are commonly used flaps and their suggested indications. These solutions may not be suitable for all patients and surgeons should always assess the wound independently before proceeding (Figure 1).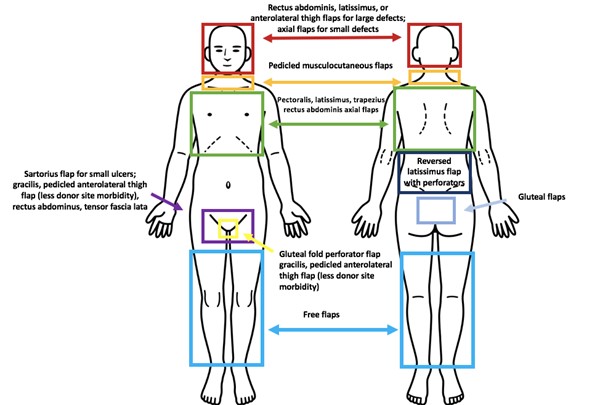
Figure 1. Common indications and suggested flaps for definite coverage of ulcers in irradiated skin and subcutaneous tissue
| Indications |
Flap |
Head and midfacial ulcers
|
Free flap transfer is used because axial flaps cannot provide adequate coverage
- Rectus abdominis or latissimus dorsi flap for large coverage or infected wound
- Anterolateral thigh flap for skull reconstruction for aesthetic concerns and fascia provides watertight closure needed by dura
|
Very small head/ midfacial defects
|
Axial flaps may be superior to free flap because the flap can be smaller and less disruptive
|
Neck radiation ulcers
|
Musculocutaneous flaps such as pectoralis or latissimus musculocutaneous pedicled flaps provide adequate coverage and acceptable donor morbidity
|
Extra articular ankylosis secondary to fibrosis
|
Free flap release
|
Chest wall ulcers (Figure 2)
|
Musculocutaneous axial flaps such as pectoralis (upper chest), latissimus, trapezius, and rectus abdominis for all areas are employed to repair defects and maintain pleural space.
Latissimus flaps are preferred for their versatility and low donor site morbidity
|
Lower and mid-back wall ulcers
|
The current recommendation is for reversed latissimus flap with perforators as it provides prerequisite coverage, is adjacent to the ulcer site, and has low morbidity.
Large defects may require free flap
|
Groin ulcers
|
Multiple flap options:
- sartorius flap: for small ulcers that do not require division of more than three proximal vascular pedicles, which causes muscle necrosis
- rectus femoris flap: limited by ulcer size and morbidity of decreased knee ROM
- tensor fascia lata flap: fasciocutaneous flap is recommended as it allows for stable blood supply and has low morbidity
- omental transposition: when femoral artery branches have been compromised. Not desirable as it requires laparotomy
|
Sacral ulcers
|
Gluteal musculocutaneous and fasciocutaneous flaps provide coverage and have low morbidity.
- Reverse latissimus pedicled flap can also be used, but usually is limited by size of coverage
- Musculocutaneous free flap can be used, but recipient vessels are often inadequate
- Gluteal perforator flaps are also useful
- Spinal cord involvement requires bone debridement and dural patching
|
Vulvar ulcers
|
If cutaneous perforators off internal pudendal artery are identified, a gluteal fold perforator flap should be used as it is similar to vulvar skin in thickness and width, and offers good aesthetic outcomes with low donor morbidity
|
Leg defects (Figure 3)
|
Free flaps |

Figure 2: 2A) Chronic radiation-induced ulceration of the upper back in a 54 year old woman. The ulcer appeared after a cervical spine surgical procedure (see posterior surgical scar). It was treated for several weeks with standard wound care (topical antimicrobial ointment and dressings) but with no signs of improvement. The patient had a past history of radiotherapy for dorsal sarcoma 9 years prior. 2B) Ultimately the patient received a trapezius rotation flap that provided definitive wound coverage.
Figures 3: 3A) Chronic radiation-induced ulceration of the leg in a 65 year old woman, who received radiotherapy for sarcoma. This image was taken several years after completion of radiotherapy. The wound had been treated with over 100 hyperbaric oxygen therapy sessions, and with silver-impregnated foam dressings. 3B) Ultimately, the ulcer required surgical debridement and reconstruction with free muscle flap
Adjunctive Therapy
The adjunctive therapies below are indicated for chronic radiation-induced ulcers (i.e., late effect) if there are no signs of improvement of the ulcer after four weeks of conservative therapy.
Negative pressure wound therapy (NPWT)
- May be appropriate as adjunctive treatment of chronic radiation-induced ulcers that are deep and do not have tendon, bone, nerve or vessels exposed, and/or if the patient is not a surgical candidate for surgical wound closure.
- NPWT is extensively used to treat acute and chronic wounds of different etiologies.[59] Many studies have also been published detailing use of NPTW for treatment of chronic radiation-induced cutaneous damage.[60][61][62] However, use of NPWT for skin breakdown due to acute reactions has not been well-documented. Rudert et al. found that NPWT used in conjunction with brachytherapy for treatment of soft tissue sarcomas resulted in decreased acute and chronic damage. The patients experienced no greater than grade 2 toxicity on the LENT-SOMA scale.[63]
Skin substitutes (i.e., cellular and/or tissue products or CTP)
-
2CClinicians may consider utilization of cellular and/or tissue products (CTPs) as an adjunctive therapy to promote healing of refractory chronic radiation-induced wounds (Grade 2C)
-
Rationale: Low certainty evidence (evidence level C) support use of CTPs to promote healing of radiation-induced cutaneous damage. Current evidence is mainly derived from encouraging results described by case reports and experimental studies utilizing different types of CTPs.[64][65] [66][67][68][69][70][71] Most CTPs utilize a scaffold that are designed to easily integrate with host tissue and provide an optimal environment for cell growth and differentiation. Some deliver growth factors that important for wound healing.[72] Despite the different types of CTPs available in the market (e.g, amniotic and placental-based, skin allografts and bioengineered skin substitutes), more randomized clinical trials and cost-effectiveness analyses are needed to strengthen evidence to support routine use as adjunctive interventions to promote healing of radiation-induced chronic ulcers.
Hyperbaric oxygen therapy (HBOT)
-
HBOT is indicated as an adjunct intervention to promote healing of refractory wounds on irradiated areas with onset at least 6 months since last radiation exposure, in patients with history of radiation in excess of 40 Gray.[17][18] For HBOT protocol and criteria see "Soft Tissue Radionecrosis".
- 1BFor patients with non-healing ulcers who need reconstructive soft tissue surgery or flaps into a previously irradiated area in the head or neck, we recommend HBOT to prevent postoperative wound dehiscence (Grade 1B)
-
Rationale: Therapeutic delivery of oxygen at higher than atmospheric tension has been demonstrated to increase wound healing through stimulation of angiogenesis in hypoxic tissues.[57]. A Cochrane review investigated the use of therapeutic oxygen delivery in late radiation injuries and found there is moderate quality evidence to support use of HBOT in head, neck, and rectal wounds. [73] Tahir et al. performed a review with similar findings. [74] In their 2017 systematic review, Borab et al. found promising associations between HBOT and healing of skin necrosis. Further, high-powered studies are required to definitively demonstrate the benefits of HBOT in irradiated tissues.[75] Radiation injury is one of the indications “approved” by the Undersea and Hyperbaric Medicine Society (UHMS), and insurers in the U.S. will usually cover HBOT for this indication.[17]
Experimental therapy
For acute effects:
-
Stem cell: radiation damage to cutaneous stem cells has been demonstrated to be a key factor in impaired wound healing. There exists a rich body of literature regarding the use of dermal fibroblasts, adipocyte, and mesenchymal stem cells for treatment of irradiated wounds. The proposed mechanisms include terminal differentiation of stem cells, immunomodulation, and paracrine effects.[57] Human studies are rarer, however, limited to case reports. Bey et al. described the use of autologous bone marrow stem cells for treatment of a radiation burn that failed conservative and surgical management.[76]
-
Growth factors: administration of growth factors such as platelet derived growth factor (PDGF) has been shown to improve wound healing. Iervolino et al. prepared autologous platelet gel rich in PDGF and administered it to ten patients with acute radiation-induced cutaneous damage and found complete resolution in all patients who were treated. [77]
-
Deferoxamine: in addition to acting as an iron chelator, deferoxamine has been shown to increase angiogenesis. Farberg et al. [78] investigated deferoxamine use in rats that had undergone mandible distraction and subsequent radiation. They found the experimental group had increased bone regeneration and angiogenesis, which indicates a potential therapeutic use for deferoxamine.
-
Low level light therapy (LLLT): the use of LLLT is currently under investigation for treatment of acute radiodermatitis.[4] Censabella et al. found that use of LLLT in acute radiation dermatitis led to a decrease in skin toxicity compared to the control group, indicating a potential new use for this technique.
For late effects:
-
Fat grafting: autologous fat grafts are used frequently in plastic surgery for reconstruction and can be delivered alone, as composite grafts, or with vascularized tissue flaps. Fat grafting has been shown to improve healing of chronic radiation-induced cutaneous damage with no subsequent recurrence or ulcer.[79][80] Adipocyte stem cells have also been shown to improve fibrosis and wound contracture in chronic breast cancer radiation injuries. [79] Both Sultan et al. and Garza et al. demonstrated that fat grafting under irradiated skin decreased dermal collagen deposition, while the latter group also found decreased vessel attenuation.[81][82] The proposed mechanisms for improved wound healing include immunomodulation, mediation of fibrosis, while enhancing angiogenesis and adipogenesis.[83] Fat grafting is an attractive option that holds promise in healing of these wounds.
-
Antiapoptotic and antioxidant therapy: radiation induced apoptosis and free radical liberation from DNA damage are key mediators of impaired wound healing and have been investigated as potential therapeutic avenues. Doctrow et al. found that systemic synthetic superoxide dismutase/catalase analogs improved wound healing and downregulated genes associated with oxidative stress in irradiated rat skin. [84] Delanian et al. reported that treatment with the antioxidant liposomal copper/zinc superoxide dismutase led to reduction in radiation-induced fibrosis and a decrease in TGF-ß1 mRNA [51], a pathway that is related to decreased inflammation and scarring. [85]
-
Pro- and anti-TGF-ß1 therapy: TGF-ß1 has a controversial therapeutic role. When combined with basic fibroblast growth factor, TGF-ß1 was shown to improve wound healing in irradiated tissue by enhancing cellularity and tensile strength in a rat model. [86] In contrast, Flanders et al. demonstrated that suppression of TGF-ß1 via knockout of signalling mediator Smad3 in a mouse model led to a decrease of inflammation and scarring while maintaining wound strength.[85]
PREVENTION
As the prevalence and incidence of radiation-induced cutaneous damage have increased, so too has the emphasis on prevention. Reduction of exposure via adequate shielding and targeting of radiotherapy is the standard of care and should always be practiced.[1]
Prevention of acute radiation-induced cutaneous damage:
Skin care and preparation before and after radiotherapy
The interventions below are intended to prevent acute radiation-induced cutaneous damage in persons undergoing radiotherapy.
Washing practices
-
1BFor patients undergoing radiotherapy, we recommend gently washing the area to be irradiated with water and soap before radiotherapy, to reduce severity of acute reactions (i.e, reduce incidence of CTCAE 4.03 Grade =2).(Grade 1B)
-
-
Rationale: Systematic reviews [28] [9] provide moderate certainty evidence (evidence level B) that support this intervention to reduce severity of acute reactions, but not to completely prevent them. Washing with water and soap will likely reduce bacterial load and allow patients to maintain their normal hygienic routine and psychosocial well-being.[9] Areas should be meticulously dried after cleaning.
Skin care
- Avoid alcohol containing products because they dry skin, which can worsen radiodermatitis [29] [8]
- Clinical guidelines strongly recommend normal antiperspirant use during the course of breast radiotherapy because no adverse effects have been documented and to maintain a sense of routine [87]
Topical steroids
-
2BClinicians might opt to have patients apply topical corticosteroids on the areas to be irradiated prior to radiotherapy, to mitigate inflammatory symptoms (Grade 2B). Caution should be exercised to avoid adverse effects related to prolonged use of corticosteroids.
-
-
Rationale: Recent systematic reviews highlight moderate certainty evidence that support use of topical steroids to reduce the pruritus, incidence of moist desquamation as well as the mean toxicity grade.[9] [25] However, it is important to avoid long term steroid use as it can lead to dermal atrophy, acne, telangiectasia, rosacea, dermatitis, delayed wound healing, and skin discolorations.
Skin hydration
- Unscented, lanolin-free, emollient cream daily, after radiotherapy [4][30]
- Do not apply lotion to radiation zone an hour before treatment as it can cause a bolus effect and increase the incidence of radiation injury [4][7][29][8][30]
Sun exposure
- Minimize or limit sun exposure to irradiated skin to prevent further injury [1][7][28]
- Use sunscreen with UVA/UVB coverage
Clothing
- Loose-fitting, cotton clothes that will minimize contact with irradiated skin [7][28]
Hair care
- Clip, do not shave hair to prevent irritation [7]
Temperature
- Avoid extremes of temperature [3]
Prevention of acute and late radiation-induced cutaneous damage:
Use of advanced modalities in radiation delivery
The delivery of radiotherapy has advanced to improve its therapeutic effect as well as decrease its associated adverse effects. Techniques such as the ones described below tailor the radiation delivery to maximize anti-oncological effect, while minimizing damage to healthy tissue.[1][88][13][89]
-
Fractionation: Fractionation has been shown to decrease the incidence of damage to healthy tissue, even if the total dosage is greater than a single treatment. Non-malignant cells with intact cellular repair mechanisms are able to overcome “sublethal” doses of <2 Gy. In contrast, cancerous cells, which have impaired DNA repair mechanisms and disrupted cell cycle checkpoints are much more susceptible to the damage. [89][90][91] However, there is new evidence to suggest that hypofractionation — giving larger doses over fewer days — may be as effective or superior to conventional fractionation as it preserves anti-cancer immune function. [92]
-
Radiation therapy techniques: Tailored delivery of radiation has been shown to decrease toxicity while preserving anti-oncologic effect. [93] Intensity-modulated radiotherapy was found to decrease the incidence of moist desquamation to 31.2 percent compared to 47.8 percent with the standard technique.[93]
PATIENT EDUCATION - FOR CLINICIANS
Radiation-induced cutaneous damage is an almost ubiquitous sequela of radiotherapy. Every patient undergoing cancer treatment should be prepared to experience some manifestation of skin toxicity during their course.[1][2] We recommend sharing our patient education materials with patients receiving radiotherapy, with acute or late radiation-induced cutaneous damage:
-
"Patient Education - Radiation-Induced Cutaneous Damage - Acute Effects"
-
"Patient Education - Radiation-Induced Cutaneous Damage - Late Effects"
For all patients (i.e, receiving radiotherapy, with acute or late radiation-induced cutaneous damage):
- Patients should be counseled on the different presentations of acute and chronic injuries, and cautioned that the latter can appear years after treatment.[94][13][57]
- Regarding risk factors:
- It is important to discuss risk factors for developing radiodermatitis, especially those that can be modified, such as smoking and obesity, to decrease the incidence and severity of acute effects. [1][7][95]
- Extrinsic risk factors (e.g., radiation methods and dose) impact on the incidence of both acute and late effects. Patient understanding of which methods and how much radiation they have/will receive helps raise awareness of symptoms of acute and late effects so that patients can seek timely medical attention
- See "Radiation-induced cutaneous damage-Introduction and Assessment".
For patients receiving radiotherapy:
What to expect during radiotherapy
- Since acute toxicity follows a stepwise progression, the different stages can be clearly demonstrated with images.[9][96][97] A visual depiction can help patients better understand the process and progress of their illness, so as to better prepare.
- Chronic toxicity is more variable, so it is more difficult to illustrate than acute. Patients should be counseled on the importance of following up even after the completion of radiotherapy to ensure chronic radiation-induced cutaneous damage are not missed.
- Finally, patients should be counseled on the risks of delaying or refusing treatment of radiation-induced cutaneous damage, should these lesions develop. If treatment of the radiation-induced cutaneous damage is delayed, infection, evolution of the wound to compromise underlying structures may occur.[1][7][9][98]
Prevention of acute radiation-induced cutaneous damage
- Measures such as prophylactic topical steroids [9][25][5], cleaning with soap and water [28][9][99], avoidance of emollients before treatment [4] [7][29][8][30], avoidance of sun exposure [1][7][28], and minimizing friction and irritation of irradiated skin [7][28] all decrease the incidence and severity of radiodermatitis. See ‘Prevention’ above.
For patients with acute radiation-induced cutaneous damage:
Treatment
Acute toxicity usually resolves with conservative wound care to keep the wounds clean and moist, periodic debridement, and topical steroid therapies.[7][8][9][12]) Moist desquamation can be treated with moist dressings.[6][7][8][9] Infections should also be treated with appropriate antibiotics.
Follow-up
- Patients should be encouraged to follow up with their physicians even after resolution of initial symptoms as chronic injury may recur months or years after radiotherapy.[94][13][57]
For patients with late radiation-induced cutaneous damage:
Treatment
Chronic damage takes time to present, and patients should be cautioned that even they may suffer from this condition even after the acute phase has resolved.
- Telangiectasias can be treated effectively with laser therapy.[4][13][9]
- Fibrosis is more difficult to treat, but may respond to tissue manipulation and massage. [1][13] Pharmacotherapy including pentoxifylline has also been shown to be beneficial in reversing the fibrotic deposition. [1][9]
- Chronic ulcers should be treated according to the ulceration and necrosis algorithm outlined above. See section 'Ulcers'. Conservative wound care is first line. [12][6][7][8][9] If that fails or if the ulcer threatens critical structures, surgical intervention to achieve definitive coverage is required. [57][16][43] Patients should be counseled on the possibility of secondary malignancy and clinicians should always consider this when evaluating an ulcer in previously irradiated territory.[1][7][23]
- Some patients may benefit from adjunctive therapy including negative pressure wound therapy [60][61][62], hyperbaric oxygen therapy [73][74] or cellular tissue products. [64][65][66][67][68][69][70][71] These options should be discussed with patients who meet the criteria.
Follow-up
- Patients should be encouraged to follow up with their physicians even after resolution of initial symptoms as chronic injury may recur months or years after radiotherapy.[94][13][57]
-
Telehealth Conferencing Tool can be used in between scheduled appointments to determine need for an additional in-person visit.
APPENDIX
Summary of the evidence: use of silver sulfadiazine for acute radiation-induced cutaneous damage
Systematic Reviews, meta analyses, clinical guidelines
- A 2013 systematic review made a weak recommendation supporting the use of for silver sulfadiazine cream in breast cancer (Level II evidence, Grade of Recommendation B). Use of silver sulfadiazine was found to decrease the incidence of radiation induced skin injury in breast cancer. This was based on a single RCT [34] that found silver sulfadiazine to both prevent and treat radiation-induced cutaneous damage.[9]
- A 2008 consensus guideline suggested use of silver sulfadiazine or beta glucan cream after radiotherapy for injuries grades 2 and 3 on the CTCAE 4.03 scale, possibly in the evening, after cleaning the irradiated area, to promote healing. However no RCT was cited to support recommendation.[8]
- A 2015 systematic review included 12 RCTs that evaluated the effectiveness of topical therapies including sulfadiazine in patients with breast cancer to treat or prevent acute radiation injuries. The authors found that among the interventions evaluated, only polyurethane dressings appear to be effective in management and prevention of all stages of skin toxicity, as well as improvement of well-being. [100]
Randomized Controlled Trials
- A 2012 RCT (n=42) compared silver nylon dressing to the standardized care, silver sulfadiazine, in treating radiodermatitis of anal/rectal cancer patients undergoing chemo and radiotherapy. Treatment started day one of radiation and continued until two weeks after completion. Silver nylon dressing was found to be superior in reducing symptoms as determined by blinded scorers using standardized dermatitis scoring scales. [101]
- A 2012 RCT (n=102) concluded that silver sulfadiazine cream 1%, three times a day, three days a week, for five weeks during radiotherapy and one week after completion reduced the severity of radiation-induced skin injury compared with general skin care alone. The RCT can be classified as moderate certainty (evidence level B) due to the fact that patients were not blinded and the lack of follow-up through 90 days, the period during which acute injuries may arise.[34]
- A 2008 RCT (n=12) compared silver-leaf nylon dressings with silver sulfadiazine cream applied on each side of the body, in patients receiving radiation for head-and-neck cancer. The authors concluded that silver leaf dressing does not appear to be superior to standard treatment for radiation-induced dermatitis when the RTOG grading system is used. It does, however, seem to reduce the severity of reaction within the same grade, and provide improved pain control over treatment with silver sulfadiazine. Evidence level C (low certainty due to small sample size, assessor and patient not blinded) [99]
Summary of the evidence: pentoxifylline with vitamin E for treatment of fibrosis back to text)
Systematic reviews, meta analyses, and clinical guidelines
- A 2016 review included 5 RCTs that evaluated pentoxifylline ± tocopherol in treating radiation induced fibrosis and found mixed results. One cited study [46] found that it took 2 years of treatment to reach maximum efficacy and that stopping treatment within a year of initiation led to increased risk of fibrosis. In light of the conflicting data, the authors called for more data to ascertain the effects of the drug therapy[13]
- A 2013 set of clinical guidelines included two prospective single arm studies evaluating the use of pentoxifylline and vitamin E in treatment of cutaneous fibrosis. The panel concluded there was insufficient evidence to support a recommendation for or against pentoxifylline and vitamin E. (Level of evidence II, Recommendation Grade B) [9]
- A 2016 review included 5 RCTs that evaluated pentoxifylline ± tocopherol in treating fibrosis. The authors concluded that PTX+vitamin E can reverse radiation-induced fibrosis, but the optimal dosage and timing are currently unknown.[1]
- A 2013 review included one retrospective analysis [49] that compared pentoxifylline and vitamin E as both combined and monotherapy to placebo in treating fibrosis. Combined therapy was found to be the most efficacious and superior to monotherapy. The authors concluded that 400 mg twice a day up to 1200 mg daily of pentoxifylline and 1000 units of vitamin E daily were effective in reducing fibrosis and radionecrosis.[29]
Randomized Controlled Trials
- A 2004 RCT (n=78) compared the prophylactic effect of PTX on complications of radiotherapy in patients with squamous cell carcinoma of head and neck. Patients received 400 mg three times a day. Four patients were removed from the study due to gastrointestinal upset and dizziness. The experimental group was found to have superior rates of skin changes, fibrosis, and soft tissue necrosis compared to the placebo group. No effects were found on pain scales. [50]
- A 2004 double blind placebo controlled RCT (n=68) compared vitamin E and PTX treatment of patients with arm lymphedema and fibrosis after surgery and radiotherapy for breast cancer. The experimental group was treated with dl-alpha tocopheryl acetate 500 mg twice daily and 400 mg PTX twice daily or placebos for 6 months. The groups were evaluated using ipsilateral limb measurement. At twelve months after initiation of treatment, no significant difference was found in arm measurement, nor were differences found in fibrosis, chest wall appearance, or quality of life. The authors concluded that the regimen does not have an effect in arm lymphedema following axillary surgery and radiotherapy, nor does it benefit fibrosis of the chest.[58]
- A 2009 double blind, placebo controlled RCT (n=83) compared PTX and vitamin E to placebo in reversing radiation-induced fibrosis of patients with breast cancer. Patients received 400 mg PTX three times daily or placebo in combination with 100 mg vitamin E three times daily starting one to three months post completion of radiotherapy. The end point was abduction of shoulder, improving from inability to do so at the beginning of the trial. Seven patients withdrew for progression of disease. The experimental group improved over the placebo in arm volume and shoulder abduction, leading the authors to conclude the combination therapy is safe and effective at reducing radiation side effects.[44]
- A 2013 RCT (n=53) investigated the efficacy of PTX and vitamin E at preventing radiation induced fibrosis of breast. Experimental patients received 400 mg PTX three times daily and vitamin E 400 units daily for six months after radiotherapy. Tissue compliance was the primary outcome and measured by a compliance meter at eightteen months. Subjects were followed for two years. Experimental group was found to have significant difference in fibrosis and treatment was found to be safe means of preventing fibrosis.[45]
- A 2005 study (n=44) investigated treatment of fibrosis with PTX and vitamin E from six to 48 months finding 68% regression required two years of treatment. Those who stopped treatment before twelve months had rebound of fibrosis. The authors recommended a long course of treatment (greater than three years) for fibrosis. [48]
Summary of the evidence: should CTP be used to treat late radiation-induced radiation damage? (Back to text)
Systematic reviews, meta analyses, clinical guidelines
- A 2016 systematic review investigating the use of Integra for scalp wounds reviewed 34 articles and recommended against Integra use for previously irradiated scalp wounds due to the low take (50-100%) and complication rates. [102]
Experimental studies
- A 2013 experimental study investigated the use of chitosan-based skin substitutes in irradiated, full-thickness wounds in a rat model. Wounds were created in the dorsum two months after irradiation with ten Gy. The wounds were treated with either a chitosan dermal substitute, chitosan skin substitute, or Duoderm CGF dressings. Wounds treated with skin substitute showed the greatest reepithelialization. Scar size was found to be smallest in the skin and dermal substitute groups. [103]
- A 2016 experimental study compared use of bilayer and monolayer autologous skin substitutes in murine irradiated wounds. Monolayers contained keratinocytes and bilayers contained keratinocytes and fibroblasts. Healing efficiency was found to be improved in bilayer treated mice compared to monolayer and controlled as measured by wound closure rates, histological sectioning, and protein expression of TGF-B, PDGF, VEGF. The authors concluded that bilayer autologous skin substitutes are superior to monolayer.[64]
- A 2015 experimental study compared wound healing in irradiated rat wounds between bilayer engineered skin substitutes, chitosan skin templates, or duoderm, (a hydrocolloid dressing). They found improved healing in bilayer and chitosan templates as evidenced by H&E staining. [65]
- A 2004 experimental study investigated the use of human amniotic membrane loaded with marrow mesenchymal stem cells to treat full thickness, irradiated wounds in a minipig model. Healing time was found to be significantly faster in the experimentally treated wounds compared to the control. Experimentally treated wounds had increased rates of granulation, reepithelialization, increased angiogenesis, and decreased inflammatory infiltrate to the control group. [66]
Case reports
- A 2016 case report (n=1) detailed use of acellular dermal matrix to treat a chronic radiation ulcer of the breast. Excision of the irradiated tissue with tissue expander and application of ADM led to resolution of the ulcer and improved cosmesis. [67]
- A 2013 case series (n=3) reported three recalcitrant chronic irradiated wounds (abdomen, thigh and sacrum) that failed traditional therapies, which were treated with porcine bladder matrix. Wound closure was achieved within three weeks of application and remained closed for nine months of follow up. [68]
- A 2016 case report (n=3) investigated the use of cryopreserved amniotic suspension allograft (CASA) topically and subcutaneously in the treatment of chronic, non-healing wounds. Three irradiated wounds were included in the study. One patient with post-mastectomy tissue necrosis required surgical closure in addition to CASA application. All wounds closed within 5-22 weeks of application. [69]
- A 2016 case report (n=1) detailed the use of polylactide-based skin substitute to treat acute moist desquamation of plantar foot melanoma. After application the patient received the remainder of the radiotherapy regimen. The skin substitute remained in place for ten days, after which it was removed to reveal successful reepithelialization. The remaining course was uncomplicated. [70]
- A 2003 case report (n=14) detailed the use of irradiated amnion as a biological dressing to treat moist desquamation of the pelvis secondary to radiotherapy for carcinoma of the cervix or rectum. All treated wounds healed within 4-16 days (median of 7) and a median of four dressing changes. No complications were reported. [71]
Summary of evidence: Should washing with soap and water be encouraged to prevent radiation-induced cutaneous damage? (back to text)
Systematic reviews, meta analyses, and clinical guidelines
- A 2013 systematic review included three relevant studies and made a strong (level II evidence, Grade B) recommendation for use of gentle soap and washing to prevent moderate/severe acute radiodermatitis. Cohorts who were permitted to wash had decreased incidences of CTCAE 4.03 Grade =2.[9]
- A 2014 systematic review included three relevant studies. Washing with soap was not found to affect the incidence of radiation-induced cutaneous damage. However, washing with soap was found to be superior to no washing for decreasing the incidence of moist desquamation at the end of treatment with two weeks of follow up, and decreased incidence of itch and erythema. The only difference between washing with and without soap was incidence of itch at week eight of treatment. The authors stated that patients may be advised to gently wash with soap, but did not give a grade or evidence.[28]
- A 2006 systematic review and guideline included 3 relevant studies and made a recommendation that skin washing should not be restricted and can be performed with or without soap. No grade or evidence was given. [6]
Randomized Control Trials
- A 2001 RCT (n=99) compared washing with soap and water to no washing in preventing the incidence of acute radiodermatitis in breast cancer. Moist desquamation was found to be higher in the non-washing group (33 vs 14 percent) and scores of pain, itch, and burning were higher in the non-washing group, but not significant. The authors concluded that washing with soap should not be avoided as it does not increase toxicity.[99]
Summary of the evidence: Should topical steroids be used to prevent acute radiation-induced cutaneous damage? (Back to text)
Systematic reviews, meta analyses, guidelines
- A 2013 review included five relevant studies that compare the use of topical corticosteroids to no treatment, an emollient, a placebo, or dexpanthenol in prevention of radiodermatitis in breast cancer. Treated groups had reduced maximum toxicity (11 percent of treated suffering CTCAE Grade 2 or higher versus 37 percent of control) and moist desquamation (17 percent in treated versus 40 percent untreated). One study compared 0.1% mometasone furoate to placebo and found significantly decreased discomfort, burning, and itching, but no difference in maximum toxicity grade endpoints. The authors make a strong (level II evidence, Grade B) recommendation for use of prophylactic topical corticosteroids (mometasone - potent) to reduce discomfort and burning.[9]
- A 2017 review included nine relevant studies that detailed topical prevention of acute radiodermatitis of the breast. The authors concluded that topical corticosteroid treatment significantly reduces the incidence of moist desquamation as well as the mean toxicity grade. Use of topical corticosteroids can also reduce the incidence of pruritus and increase quality of life. [25]
- A 2006 review included five relevant studies that investigated the use of topical corticosteroid use to prevent acute radiodermatitis. The authors found insufficient evidence to recommend the use of topical corticosteroids. However, they did state in the group opinion that there can be a use for low potency steroids with the caveat of potential adverse reaction due to long use.[6]
- A 2014 review included four relevant studies that assessed using topical corticosteroids to prevent acute radiodermatitis. The authors found insufficient evidence to make a recommendation and called for more, rigorous studies.[28]
Randomized control trials
- A 2011 double blind RCT (n=176) compared the use of daily mometasone furoate to placebo in the prevention of acute radiodermatitis of the breast or chest wall. They found no significant difference in the mean maximum grade of radiodermatitis. The steroid treated group had significantly lower pruritus, irritation, persistence of symptoms, and burning sensation compared to the control group. The authors concluded that use of mometasone may reduce skin toxicity compared to placebo.[87]