ABSTRACT
This topic covers management of acute burns. For a review and framework for assessment of acute burns including first aid and initial care (primary assessment, assessment of inhalation injury, secondary assessment), classification of acute burn injuries, burn center referral criteria, documentation and ICD-10 coding, see topic "Acute Burns - Introduction and Assessment". For clinical guidelines and quality measures, see "Acute Burns - Overview".
Treatment summary
Patients should be assessed, triaged and referred to a burn center as per criteria outlined in sections ‘Classification of Burn Injuries’ and ‘Burn center referral criteria’ in topic "Acute Burns - Introduction and Assessment". Management of minor, moderate and severe burn injuries require pain control, tetanus immunization and local wound care. Patients with moderate or severe burn injuries generally meet at least one burn center referral criterion. Nutrition should be optimized and antibiotics administered, if indicated. In addition, patients with severe burn injuries often require initial stabilization, coagulopathy management, thromboprophylaxis and surgical management. Table 1 provides details on management of burn injuries by severity.
Hospital admission: Patients with inhalation injury, hemodynamic instability requiring monitoring, or any other risk factors that are potentially life threatening must be admitted to an intensive care unit. Other burn patients may be treated as outpatients or inpatients depending on specific conditions and criteria. See ‘Burn center referral criteria’ in topic "Acute Burns - Introduction and Assessment", and 'Disposition' in Table 1 in this topic.
Whether the patient is treated in the outpatient or inpatient setting, an adequate treatment plan for acute burns should aim to:
Treat the cause/ provide systemic treatment. See details related to:
- Initial stabilization with fluid resuscitation, inhalation injury management
- Infection management
- Tetanus immunization
- Nutritional optimization
Address patient's concerns
- Pain control is critical to ensure comfort and help promote healing
Provide effective wound care
- Local interventions: the primary goals of local wound management are the prevention of desiccation of viable tissue and the control of bacteria. Topical management will follow the same basic principles of wound management, including cleansing, debridement of nonviable tissue, infection control, and moisture management. See local wound care for superficial, superficial partial-thickness, deep partial-thickness and full-thickness burns in 'Local Interventions' in this topic. Table 2 shows local wound care interventions for burn injuries by burn depth, Table 3 shows dressings and topical products commonly utilized in burn injuries.
- Surgical management: escharotomy is indicated for circumferential burns of the limbs and/or thorax that compromise blood circulation or oxygenation. Surgical excision of burns with or without definitive wound coverage with skin grafting is employed in the treatment of most full thickness burns, and often in patients with burn TBSA greater than 10%. See indications, techniques, and types of wound coverage.
Plan Reassessment: patient follow up intervals vary according to burn severity.
Adjunctive Therapy: see details on biophysical interventions (e.g., negative pressure wound therapy, hyperbaric oxygen therapy), wound coverage with cellular and/or tissue products and biologics (e.g. mesenchymal stem cells)
ICD-10 coding: See section on 'Coding' in "Acute Burns - Introduction and Assessment"
Clinical guidelines and quality measures: See "Acute Burns - Overview".
This topic covers management of acute burns. For a review and framework for assessment of acute burns including first aid and initial care (primary assessment, assessment of inhalation injury, secondary assessment), classification of acute burn injuries, burn center referral criteria, documentation and ICD-10 coding, see topic "Acute Burns - Introduction and Assessment". For clinical guidelines and quality measures, see "Acute Burns - Overview".
Background
Patients should be assessed, triaged and referred to a burn center as per criteria outlined in sections ‘Classification of Burn Injuries’ and ‘Burn center referral criteria’ in topic "Acute Burns - Introduction and Assessment".
In all practice settings, it is essential to ensure that the treatment plan and care provided adheres to the specific facility's policies, procedures, protocols, and formulary.
Treatment goals
Treatment goals and plan are determined by the extent, depth of burns and overall patient status.
Management by Burns Severity
Table 1 below provides an overview on management of burn injuries by severity, based on clinical guidelines by the International Society for Burns Injuries (ISBI), American Burn Association (ABA), systematic reviews, and expert opinion.[1][2][3]
Table 1. Overview on management of burn injuries by severity
| Minor burn | Moderate burn | Major/severe burn |
| Definition | - Partial-thickness burns <10% TBSA in patients 10 to 50 years old
- Partial-thickness burns <5% TBSA in patients under 10 or over 50 years old
- Full-thickness burns <2 % TBSA in any patient without other injury
Also: - Does not meet any of the burn center referral criteria as defined by the American Burn Association
- Isolated injury
- Does not affect feet, face, hands, perineum or major joints
- Is not circumferential
| - Partial thickness burns 10-20% TBSA in adults
- Partial thickness burns 5-10% TBSA in children or those over age 50
- 2-5% full thickness burn
- Low voltage burn, suspected inhalation injury, circumferential burn
- Comorbid conditions predisposing to infection (e.g., diabetes mellitus, sickle cell anemia)
| - Partial thickness burns >20% TBSA in adults
- Partial thickness burns >10% TBSA in children or those over age 50
- >5% full thickness burn
- High voltage burn
- Chemical burn
- Any clinically significant burn to the eyes, ears, genitalia, or major joints
- Clinically significant concomitant (e.g., fracture, other major trauma)
|
|
Disposition
|
- Typically treated in the outpatient setting, provided none of the criteria for burn center referral is met. Intangible factors such as availability of resources, and patient’s self care ability should be taken into consideration during disposition planning
- Most patients benefit from a consult/referral to a burn center to ensure proper management in the outpatient setting
- Patients with full thickness burns should be evaluated by a burn center for the need for skin grafting
|
- Generally meet one of the burn center referral criteria. After evaluation by burn center, patient may be treated as inpatient at a hospital with experience in burn management
|
- Should be referred to or treated at a designated burn center
- Patients with inhalation injury, hemodynamic instability requiring monitoring, or any other risk factors that are potentially life threatening must be admitted to an intensive care unit
|
|
Systemic treatment and patient's concerns
|
- Pain control
- Tetanus immunization
|
- Pain control
- Antibiotics if indicated
- Tetanus immunization
- Nutritional optimization
|
- Initial stabilization
- Pain control
- Coagulopathy management
- Thromboprophylaxis
- Antibiotics if indicated
- Nutritional optimization
|
|
Local and/or surgical interventions
|
- Local interventions (See Table 2)
|
- Local interventions (See Table 2)
|
- Local interventions, including potential escharotomy (See Table 2)
- Surgical management (e.g. burn excision, autologous and other grafts, advanced wound management)
|
Treat the cause/ provide systemic treatment
Initial stabilization
Indicated for all major/severe burns and some moderate burns, before referral and after referral to a burn center.
Fluid resuscitation
-
Indications: fluid resuscitation is indicated for patients with more than 20% TBSA, older adults or children. Adequate hydration should be initiated as soon as the patient is assessed. Patients with less than 20% TBSA may achieve adequate hydration with oral fluids [4], which may be complemented with intravenous maintenance hydration.
-
Formulas: various formulas are used to guide volume resuscitation, such as the Parkland or Modified Brooke Formula. Common to both formulas, the recommended fluid is Ringer’s lactate solution (RL), administered from 2 to 4 ml/kg/% of burns over a period of 24 hours.[1] As an example of typical regimen, in the first 24 hours patients receive 2ml/kg/% of RL plus maintenance fluid calculated at 50ml/kg body weight. In the next 48h fluid is given at the rate of 1ml/kg/% of RL plus maintenance fluid at 50ml/kg body weight. [5]
-
Assessment: resuscitation formulas only serve as a guideline; the patient's physiologic response must be the true marker for assessment of adequate volume replacement.. All the formulas guide resuscitation with the aim of achieving a diuresis between 0.3-0.5 ml/kg/h in adults and 1.0 ml/kg/h in children.[1]
- In children, maintenance intravenous fluid administered after the first 24 hours must include glucose due to the risk of depleted hepatic glucose stores after 12 to 14 hours of fasting.[1]
- In adults, a recent randomized controlled trial with 200 patients concluded that dextrose normal saline (DNS) should be used as daily maintenance fluid with RL, as RL is low in sodium (130 mEq/L) as well in potassium (4mEq/L), and thus not sufficient to cover daily electrolyte requirements.[5]
- Some patients (e.g. victims of electric burns or pulmonary/inhalation injury) may present with additional fluid requirements.[6]
Inhalation injury management
- Inhalation injury is accompanied by plugs formed from dead epithelial cells, fibrin clots, and mucus, which potentiate the obstruction of the airways and result in inadequate ventilation. Diagnosis is confirmed by bronchoscopy. For details on assessment of inhalation injury, see 'Assessment of Inhalation Injury' in topic "Acute Burns - Introduction and Assessment".
- Patients with inhalation injury require prompt management, including maintenance of airway patency and adequate ventilation to ensure optimal tissue oxygenation. Frequently, patients with severe inhalation injury require intubation.
- Respiratory physiotherapy combined with mucus-thinning/anti-inflammatory medications have been reported to improve outcomes. Despite the lack of globally-accepted standard for treatment, current data support use of bronchoscopy to remove plugs, nebulization with heparin, bronchodilators and N-acetylcysteine.[7]
- Prophylactic antibiotics and corticosteroids are not indicated for treatment of inhalation injury.[2]
Infection management
- For patients with partial or full-thickness burns with spreading or systemic clinical signs and/or symptoms of infection, hospital admission and treatment with systemic antibiotics are recommended.
- 1CFor patients with acute burns of any extent or depth without symptoms or signs of infection, we recommend against use of systemic antibiotic prophylaxis to prevent infection (Grade 1C)
- Rationale: a 2013 Cochrane systematic review did not find evidence that systemic antibiotic prophylaxis improves any of the primary outcome variables assessed (burn wound infection, sepsis, bacteraemia, urinary tract infection, or death associated with infection), when compared to placebo or to no active treatment.[8]
Tetanus immunization
- For patients with burns deeper than superficial, the Centers for Disease Control (CDC) recommends that tetanus immunization be updated.[9][10]
- If the number of previous doses of tetanus toxoid is unknown or fewer than 3 doses, patients should receive tetanus immune globulin as well as tetanus vaccination.
Nutrition
Relevance
- The metabolic response to burns is characterized by hypermetabolism, increased protein catabolism, and loss of lean body mass. The degree of hypermetabolism is approximately proportional to the extent of the burn; if TBSA exceeds 30%, significant changes in metabolism occur. This hypermetabolic state contributes directly to mortality.[11]
- The presence of malnutrition also dampens the immune response, further compromising the capacity of the patient to prevent and/or recover from infections and other metabolic insults.[11] Scar formation in burns is also compromised by malnutrition, causing further delay in definitive healing.[11]
- The increase in protein catabolism leads to loss of more than one kilogram of skeletal muscle per day, which may compromise movement of the diaphragm, potentially impairing respiratory function; it also contributes to the loss of strength and endurance, thereby prolonging the rehabilitation period. [11] Despite aggressive nutritional support, protein catabolism often exceeds anabolism, making weight loss after severe burn injuries a common occurrence.[2]
Nutrition goals
- The objective of nutrition in the context of a comprehensive plan of care is to minimize the amount of weight loss during recovery.
Nutritional assessment
To achieve the goal above, serial calculated assessments of nutritional status are necessary in order to appropriately estimate the daily caloric requirements.
- The initial assessment must take into consideration pre-existing nutritional deficiencies such as marasmus or vitamin deficiency syndromes.[12]
- Follow up assessments must include routine measurements (at least twice a week) of the patient’s weight.[8][12]
- Various formulas for assessing nutritional status have been tested in adult and pediatric patients. The majority of these equations estimate the base caloric requirements per kilogram body weight or additional requirements above the calculated base quantity (based on the Harris-Benedict equation), adjusted by a factor due to stress from systemic trauma. Unfortunately, all these formulas suffer from some degree of imprecision, likely due to fluctuations in the metabolism of each patient that arise in association with inflammation, sepsis or surgical procedures. [13] However, use of these formulas is still considered best practice in burn centers all over the world.[2]
Nutrition plan
A review [14] of the most recent international clinical guidelines on nutrition for patients with severe burns found that the European Society for Parenteral and Enteral Nutrition (ESPEN) guidelines [15] provided the majority of information concerning nutrition support and medical nutrition therapy, compared to the other 7 appraised guidelines. A summary of the recommendations on nutrition for major burn injuries (i.e. > 20% TBSA, with or without inhalation injury) by the ESPEN guideline and others is provided below:
- Indication: Nutritional therapy should be initiated early, within 12 hours of injury.[15][16]
- Conventional oral diets or enteric feeds must be initiated as soon as possible (during the first 24 hours). The physiologic impetus for early nutrition in burn injury involves maintaining the thickness of the intestinal mucosa, controlling intestinal permeability, stimulating the gut-associated lymphoid tissue, supporting the processing of bacterial translocation.[2]
- Route: Guidelines recommend favoring the enteral route in the majority of cases, as parenteral administration is rarely indicated and carries increased rate of complications.[15]
- The general expectation is that early enteral feeding will improve clinical outcomes, specifically by reducing post-burn hypermetabolism and improving the immune response, resulting in less weight loss and fewer infections.[17] The few exceptions where parenteral nutrition may be preferred is in the setting of short bowel syndrome, gastrointestinal fistulas, or bowel obstruction.[2] Post-pyloric feeding seems to be more efficient than gastric feeding in ensuring tolerance to enteral nutrition and energy supplementation. If intolerance to enteral nutrition develops, parenteral nutrition may be required.[18]
- Energy requirements & predictive equations: ESPEN recommends considering indirect calorimetry as a gold standard to assess energy requirements. If not available or not suitable, the guideline recommends using the Toronto equation for adult burn patients. For children, we suggest use of Schoffield formula.[15]
- Proteins:
- Protein requirements are higher than in other categories of patients, and should be set around 1.5-2.0 g/kg in adults and 3 g/kg/day in children.[2][15]
- ESPEN suggests glutamine supplementation (or ornithine alpha-ketoglutarate) but not arginine.[15] There is low certainty evidence that glutamine may reduce mortality among patients with severe burn injury.[19]
- Glucose and glycemic control:
- ESPEN suggests limiting carbohydrate delivery (prescribed for nutritional and drug dilution purpose to 60% of total energy intake, and not to exceed 5 mg/kg/min in both adults and children), and suggests keeping glucose levels under 8 mmol/l (145 mg/dl) and over 4.5 mmol/l (81 mg/dl), using continuous intravenous infusion of insulin.[15]
- Lipids: ESPEN suggests monitoring total fat delivery, and maintaining fat calories at < 35% of total energy intake.[15]
- Micronutrients: ESPEN suggests, in both adults and children, supplementation of zinc, copper and selenium, as well as of vitamin B1, C, D and E.[15]
- Metabolic modulation: ESPEN strongly recommends using non-nutritional strategies to attenuate hypermetabolism and hypercatabolism in both adults and children (e.g. warm ambient temperature, early surgical burn excision, non-selective beta-blockers, and oxandrolone).[15] The guideline recommends administering rhGH to children with burns with TBSA >60%, but not to adults.[15]
Address Patients' Concerns
Pain control
- Pain level will differ according to patients’ pain tolerance, as well as burn extent and severity. It is important to obtain pain control to promote comfort and optimize healing conditions. The WHO Analgesic Ladder provides guidance on appropriate pain management.[20]
- Novel analgesic medication regimens including agents such as ketamine are becoming increasingly prevalent in burn management, namely in severe burns where patients are intubated and require sedation.[21][22]
Local Wound Care
The primary goals of local wound management are the prevention of desiccation of viable tissue and the control of bacteria.[2] Topical management will follow the same basic principles of wound management, including cleansing, debridement of nonviable tissue, infection control, and moisture management.[2] See summary in Table 2 below.
Table 2. Local wound care interventi ons for burn injuries [2]
| Intervention | Superficial burn injury | Superficial partial thickness burn injury
| Deep partial thickness and full thickness burn injury
|
| Cleansing | - Gently cleanse by irrigation with neutral, non-irritating, non-toxic, non-antimicrobial cleansers such as tap water/ sterile saline
| - Gently cleanse by irrigation with neutral, non-irritating, non-toxic, non-antimicrobial cleansers such as tap water/ sterile saline
- Cleanse with antimicrobials/antiseptics (e.g. chlorhexidine) after mechanical or surgical cleansing/debridement
| - Gently cleanse by irrigation with neutral, non-irritating, non-toxic, non-antimicrobial cleansers such as tap water/ sterile saline
- Cleanse with antimicrobials/antiseptics (e.g. chlorhexidine) after mechanical or surgical cleansing/debridement
|
| Debridement | | - Effective debridement can be obtained with conservative sharp, mechanical and/or enzymatic debridement techniques
- Bullae: when deciding whether unroof bullae or leave intact, factors such as potential for local infection, patient comfort, and ease of treatment must be considered
| - Non-viable tissue can be effectively removed via sharp debridement or surgical excision
|
| Infection and bioburden control | - Usually not a concern, as involves only the epidermis
| - If no signs of infection, consider limiting use of topical prophylactic antibiotics such as silver sulfadiazine (SSD) for prevention of infection or to promote wound healing
- If signs of infection, collect wound culture, initiate topical antimicrobial dressings and empiric systemic antibiotic therapy
| - If no signs of infection, early tangential excision of necrotic tissue helps prevent infection
- If invasive infection, surgical excision and systemic antimicrobial therapy are recommended
|
| Moisture management | - Patient can self-apply moisturizers with essential fatty acids or vegetable oils to promote faster wound healing
| - Benefit from occlusion for long periods (at least one week) if injury is clean. If not clean, change every other day until signs of healing
- Dressing choice depends on ulcer characteristics, clinical experience, patient preference, care setting and cost
- May apply moisturizers with essential fatty acids or vegetable oil on the wound and periwound
- Maintain wound moisture or provide moisture to dry wounds with:
- Hydrogel, foam dressings, honey gel, contact layer
- Manage exudate with:
- Alginate, fiber gelling dressing (hydrofiber), foam dressings
- See Wound Prep and Dress Tool, WoundReference's Dressing Feature Matrices
| Definitive wound coverage with autografts/ flaps is indicatedWound bed preparation for definitive coverage can be accomplished by closed or open dressings. For cases in which early tangential excision is planned, closed dressing technique is indicated. Topical antimicrobial is applied and covered with dressings to soften eschar.For cases in which early excision is not feasible (e.g. palliation, lack of resources), or on face/ perineum, open technique is appropriate until eschar separation begins.Open technique: apply vaseline-based gauze and/or topical antimicrobials on wounds. Once eschar separation begins, trim loose edges of eschar.After eschar is removed by tangential excision or is naturally separated, remaining full-thickness defect (raw area) is managed as a chronic wound until definite wound closure, as follows:For dry wounds, maintain wound moisture or provide moisture with: Hydrogel, foam dressings, honey gel, contact layerFor exudate management, consider using: Alginate, fiber gelling dressing (hydrofiber), foam dressingsSee Wound Prep and Dress Tool, WoundReference's Dressing Feature Matrices |
Cleansing
- For all acute burns regardless of size and depth: Keeping the wound bed clean helps prevent infections and is essential for expeditious healing.
- Technique: cleansing with gentle washing is the most important component of burn wound cleansing. Cleansing by irrigation decreases bacterial count and helps promote healing. [2]
- Cleanser: the beneficial effect of using antiseptics or antimicrobial agents for cleansing is unclear.[2] The ISBI Guidelines recommend [2]:
- For non-infected wounds: use tap water for cleansing non-infected wounds.
- For heavily infected wounds with evident biofilm: use of antiseptics/antimicrobials as topical antimicrobials and not cleansing agents, after tap water/saline irrigation, to combat the exposed bacteria and organisms that became ‘‘accessible’’ after cleansing.
- For burn injuries that need mechanical or surgical cleansing: cleansing with antimicrobials/antiseptics (e.g. chlorhexidine) is of great value after mechanical or surgical cleansing as this helps prevent the possible passage of the ‘‘denuded’’ bacteria to the newly opened spaces and/or bloodstream.
Debridement
- For all acute burns regardless of size and depth: Essential practices for local treatment include removal of contaminants, debris, foreign bodies, fibrinous exudates, and any nonviable tissue from the wound bed.
- At each dressing change, remove previously used dressing materials, as well as exudates and crusts. Additionally, maintain the personal hygiene and comfort of the patient.[2]
- For partial thickness burns (Figures 1 to 3):
- Effective debridement can be obtained with conservative sharp, mechanical and/or enzymatic debridement techniques.
-
- Conservative sharp debridement may be performed with curettes, scissors, etc.
- Mechanical debridement can be accomplished by brushing off non-viable tissue with sterile saline-moistened gauze or chlorhexidine surgical scrub brushes.
- An enzymatic debrider (e.g. collagenase) may be applied over non-viable tissue after cleansing and before application of secondary dressings. Clinical studies support use of collagenase as a debriding agent for burns, however evidence is of high uncertainty due to high risk of bias of these studies.[23] Collagenase may also mitigate need for surgical excision by preventing burn conversion via down-regulation of the local inflammatory response.[24] Contraindications to collagenase include local infection, allergic reactions, and use in combination with certain dressings .
- Bullae (or blisters) (Figure 3): Bullae are often present in acute partial thickness burn injuries. There is little consensus in literature as for whether or not they should be unroofed. Patients often present with blisters that have already been intentionally or inadvertently ruptured.[25] One advantage of unroofing bullae is the ability to visualize and appropriately assess the wound bed, as intact vesicles obscure the true depth. When deciding whether to unroof or leave bullae intact, factors such as potential for local infection, patient comfort, and ease of treatment must be considered.[26] There is some evidence supporting leaving bullae smaller than 6 mm intact.[26]
- For full-thickness burns: Non-viable tissue can be effectively removed with sharp debridement or surgical excision (see ‘Surgical management’)
- For longstanding raw areas (i.e., full-thickness burns after eschar has been detached or surgically removed): like with other chronic wounds, biofilm is often present. Its removal is critical for healing, and this can be accomplished through mechanical debridement (fibrous pads, curettage) or sharp debridement.[2]

Fig. 1. Right leg with partial thickness burn injury, covered with non-viable tissue. By Lebendiskaya N.

Figure 2. The same patient in Figure 1, 1 week after conservative debridement (sharp and enzymatic), moisturizer, petroleum gauze and Unna's boot

Figure 3: Partial thickness burn injury with bullae
Infection and Bioburden Control
- Superficial burns or burns in the final phase or repair with no signs of infection do not benefit from topical antibiotics. Instead, an ointment (e.g, with essential fatty acids or vegetable oils) should be used to expedite wound healing.
- 2CFor partial thickness burn injuries with no signs of infection, we suggest clinicians consider limiting use of topical prophylactic antimicrobial agents such as silver sulfadiazine to prevent infection or promote wound healing (Grade 2C).
-
- Rationale: Although commonly utilized on burn injuries, evidence gathered by 2 meta-analyses and 1 systematic review [8][27][28] shows that patients treated with prophylactic 1% silver sulfadiazine (SSD) have a higher risk of burn wound infection and longer length of hospital stay than those treated with dressings or skin substitutes (low certainty evidence, level C). As a result, use of SSD as a prophylactic topical antimicrobial agent is no longer routinely recommended. Despite its antimicrobial effect, there is no direct evidence that SSD prevents infection.[27] Furthermore, it is known to inhibit the growth of keratinocytes and fibroblasts, which may explain why partial thickness burns treated with SSD take longer to heal compared with silver dressings or dressings without silver.[27][28]
- Contraindications: If SSD is utilized on partial of full-thickness burns, it should be discontinued when epithelialization is complete. Also, eschars will not absorb topical antimicrobials and application of SSD will be ineffective until eschar is excised.[29] SSD should not be applied on patients with sulfa allergy and must be used with caution in pregnant/breastfeeding women, children younger than 2 years, individuals with G6pD deficiency, porphyria, hepatic, renal or hematological disease.[30]
- Drug interactions: SSD should not be used with the enzymatic debriders collagenase or papain, as silver inactivates these enzymes. See topic "Products that inhibit collagenase enzymatic activity".
- For partial-thickness burn injuries with clinical signs of infection, wound culture should be collected, then topical antimicrobial agents and empiric systemic antibiotics should be initiated.
- Topical antimicrobial agents include antimicrobial dressings (e.g. with silver, honey).
- Empiric antimicrobial therapy should be effective against local strains of microbes and cover gram positive and gram negative organisms. Consult infectious disease professionals or hospital microbiology department to confirm that selected empiric antibiotics are appropriate.
- For full-thickness burn injuries, early tangential excision of the necrotic tissue has been shown to prevent wound infection.[31] For invasive infection, surgical excision of the infected wound and appropriate systemic antimicrobial therapy may be required.[32]
- For patients being managed at healthcare facilities, if systemic signs of infection are present, investigation of potential sources of infection other than the burn wounds is also recommended (e.g., catheter-related infection, pneumonia, etc).[33]
Dressings
Specific dressing regimes for non-operative and post-operative management of burns will vary widely by geographic location; there is no current consensus or guideline that recommends specific types of dressing for the various types of burn injuries. Important factors to consider for dressing selection include clinical evidence, product availability, cost, facility resources, clinician familiarity and comfort with product application, patient status and condition (inpatient, bed-bound or ambulatory, or outpatient), exudate, burn depth and % TBSA, expected level of activity and mobility, any concomitant orthopedic injuries, and necessary invasive lines or devices. For specific information on dressings see Table 3 below, Wound Prep and Dress Tool, WoundReference's Dressing Feature Matrices
- 2CFor partial thickness burn injuries with no signs of infection, we suggest use of dressings with or without silver to promote wound healing, instead of SSD (Grade 2C).[27][28]
- Rationale: A systematic review and meta-analysis evaluated healing rates and incidence of infection among burn patients treated with SSD, dressings with and without silver. Authors concluded that dressings with and without silver promote faster wound healing compared to SSD, and that burns treated with dressings without silver are less likely to become infected than burns with SSD. Authors found no differences between SSD and new silver materials in regards to infection rates.[27]
- Dressings that have shown increased effectiveness in healing partial thickness burn injuries include:
- Honey-based dressings (compared to SSD or mafenide acetate, moderate certainty evidence level B) [34]
- Hydrogel (compared with usual care, low certainty evidence level C) [28]
- Dressings with nanocrystalline silver or merbromin (compared to petroleum gauze or other non-antimicrobial treatments, moderate or low certainty evidence level B or C) [34]
- When choosing dressings, humid and heat-preserving dressings are preferred.
- Maintain wound moisture or provide moisture to dry wounds with:
- Hydrogel, foam dressings, honey gel, contact layer
- Alginate, fiber gelling dressing (hydrofiber), foam dressings
- Superficial partial thickness burns and donor sites of split-thickness skin grafts benefit from occlusion for long periods (at least one week) if the burn injury is clean. If the injury is dirty (e.g. covered with materials incorrectly used for first-aid such as coffee or sand), or if the patient presents more than 24 hours after the accident, it is advisable to change the dressing more frequently (e.g., every other day) until infection is ruled out and the wound has started to heal.
- For deep partial thickness or full-thickness burn injuries, definitive wound coverage with autografts/ flaps is indicated (see section 'Wound coverage with autologous skin grafting' below) Wound bed preparation for definitive coverage can be accomplished by closed or open dressings.[2]
- For cases in which early tangential excision is planned, closed dressing technique is indicated. Topical antimicrobial is applied on the wounds and covered with dressings to soften eschar. By the end of the first week after injury, virulent organisms begin active invasion of the unburned tissue. Closed technique allows eschar to remain soft to allow tangential excision. It also prolongs contact of the antimicrobial agent with the eschar, helping prevent infection and desiccation.
- For cases in which early excision is not feasible (e.g. palliation, lack of resources), or on face/ perineum, open technique is appropriate until eschar separation begins. In the open technique, vaseline-based gauze and/or topical antimicrobials are applied on wounds. Once eschar separation begins, trim loose edges of eschar. Risk of infection is higher and patient might experience pain during eschar removal.
- After eschar is removed by tangential excision or is naturally separated, remaining full-thickness defect (raw area) is managed as a chronic wound until definite wound closure is performed.
As it relates to the application of dressings, a few practical points are listed below:
- Bandages/wraps (e.g. elastic dressing retainers, elastic roll bandages, etc) may be required to retain primary dressings. In limbs with burns, the entire limb is typically wrapped distally to proximally to control edema. If possible, fingers should be spared from the dressing and the hand wrapped in a fashion that maximizes the patient's functional independence.
- There are some specialty dressings manufactured specifically for burn injuries, including burn vests, arm, leg, and buttock pads; these can be somewhat bulky, and are ideally used for bedbound patients whose wounds require higher absorbency.
- For bedbound burn patients, moisture management to prevent moisture-related pathogen proliferation (e.g. Pseudomonas infections) is an additional consideration. Sheets, and dressings with microclimate control may be used.
- Prevention of hypothermia is crucial in burn patients, but prevention of hyperthermia and subsequent vasodilation and moisture loss is of equal importance. Specialty bed surfaces covers (e.g. KCI Skin IQ mattress cover) can draw away excess moisture from the skin/surface interface and assist with microclimate management.
The following Table 3 provides a brief overview of common dressing utilized in burns.
Table 3. Dressings and topical products commonly utilized in burn injuries [35][28][36][37][38][39][40][41][42][43][44]
| Product Category | Product Type | Attributes |
|
Skin care
|
Therapeutic Moisturizers
- Oat Beta Glucan Ointment (e.g. Glucan Pro 3000).
- Aloe vera (e.g. Fruit of the Earth 100% Aloe Vera Gel, Trader Joe’s 99% Aloe Vera Gel)
- Calendula (e.g. Califlora, Calendula ointment)
- Water-based (e.g. Light: Aveno Daily, Moderate: Eucerin, Heavy: Aquaphor)
|
- for periwound skin, superficial burns, and partial thickness burns
|
|
Skin care
|
Drying agents (e.g. Zeasorb powder)
|
- for use under skin folds to prevent skin maceration
|
|
Debridement
|
Collagenase ointment (e.g. Santyl)
|
- provides enzymatic debridement of adherent fibrinous exudates and nonviable tissue
- anti-inflammatory action
- used on partial thickness burns, sometimes used on deeper facial burns
|
|
Topical antimicrobials
|
Polysporin (powder or ointment)
|
- overall gram+/- coverage
- often mixed with collagenase to provide concurrent antimicrobial coverage with enzymatic debridement
|
|
Topical antimicrobials
|
1% silver sulfadiazine cream (Silvadene)
|
- broad-spectrum antimicrobial coverage
- twice daily dressing changes required
- can delay healing, stain tissue, and create "pseudo-eschar"
- relatively contraindicated in pregnant or nursing mothers, newborns, patients with sulfa allergy or glucose-6-phosphate dehydrogenase deficiency
|
|
Dressing
|
Silver Foam (Mepilex AG, Mepilex AG Transfer)
|
- absorbent and non-adherent
- broad-spectrum antimicrobial coverage
- decreased total cost compared with SSD
- good for skin graft donor sites and large surface areas
|
|
Dressing
|
Honey Dressings (Medihoney gel sheets, etc)
|
- has been shown to promote faster healing compared to silver sulfadiazine
|
|
Dressing
|
Hydrogel sheets (e.g. Aqua clear and Nu-gel, Johnson & Johnson)
|
- maintain wound moisture
- fluid donating properties may also aid autolytic debridement
- In its sheet form, gel is presented with a fixed three-dimensional macro structure
|
|
Dressing
|
Impregnated non-adherent gauze (Xeroform, Adaptic)
|
- Xeroform contains bismuth which is bacteriostatic and supports epithelialization
- Adaptic is not impregnated with active agents
- impregnated gauzes can be used for superficial burns, or postoperatively over skin grafts until the areas are completely healed
|
|
Dressing
|
Silicone sheets (Mepitel, Mepitel AG, Adaptic Touch)
|
- can decrease pain and dressing change frequency
- may remain intact while secondary absorptive dressings are changed
|
|
Compression
|
Compression therapy (e.g, Unna's boot for legs, Viscopaste/ Kerlix wrap for arms)
|
- help secure dressings, maintain moisture, and decrease edema
|
Surgical Management
Escharotomy
Indications
- Escharotomy is indicated for full-thickness circumferential burns of the limbs with signs of reduced tissue perfusion (diminished or absent peripheral pulses) (Figure 4), and circumferential injuries of the thorax and chest that compromise ventilation and oxygenation (Figure 5).[2]
-
- Although retrospective studies have been published, most studies do not describe in details when escharotomies should actually be performed.[45] Also, to date no randomized controlled study has explored the treatment of compartment syndromes in the thorax or extremities.[2]
- When indicated, escharotomy is generally performed after the initiation of fluid resuscitation.[46] This procedure must be performed early in order to avoid complications from inadequate mechanical ventilation, such as atelectasis.

Fig. 4. Full-thickness circumferential burn of right leg. Signs of reduced tissue perfusion may be present

Fig. 5. Full-thickness circumferential burn injury of the thoracic and abdominal regions
Procedure
- Extremities: Incisions are made on the lateral and medial aspects along the longitudinal axis of the limbs, avoiding the path of the blood vessels (Figure 6); it is preferable to begin distally and proceed proximally, so that the incision can be discontinued when viable tissue is reached and bleeding is visualized.
-
- In the event of electrical burns or circumferential burns in involving the hand, early decompression of the hand is indicated (Figure 7). In circumferential or electric burns of the upper extremity, it is often necessary to free the carpal tunnel and retinaculum of the forearm flexor muscles. Various structures are present in the reduced space of the wrist and decompression ensures effective return of perfusion to the distal aspect of the fingers.[1]

Fig. 6. Escharotomy performed along the upper right extremity.

Fig. 7. Escharotomy of the hand
-
- Circumferential burns of the thorax: For circumferential burns of the thorax, incisions over the anterior axillary lines and between the abdomen and thorax are indicated in order to facilitate chest excursion and subsequent lung expansion. Of note, an escharotomy in this area will not follow longitudinal lines (Figure 8).
-
Abdomen: Abdominal escharotomy must be performed whenever a circumferential or semi-circumferential burn is associated with evidence of abdominal compartment syndrome (ACS). ACS is a critical issue that may be associated with many forms of trauma (Figure 8). Burn injuries are a relatively uncommon cause of ACS, but burn patients may develop ACS even in the absence of severe abdominal wall burn injury. In these patients, ACS may result from massive blunt trauma, fluid overload with crystalloids, or septic shock. Therefore, the presence of full-thickness circumferential burns of the abdomen does not predicate ACS and inversely, the absence of abdominal burns does not exclude the presence of ACS. Furthermore, there is a notable mortality rate among burn patients with ACS despite undergoing abdominal escharotomy, which raises questions about the efficacy of escharotomy in the treatment of ACS. ACS can be diagnosed by measuring the intravesical pressure (IVP) through a catheter inserted inside the urinary bladder. The normal IVP value is lower than 5 mmHg, but a value of up to 12 mmHg is accepted in trauma cases. Values higher than 25 mmHg indicate raised intra-abdominal pressure and require intervention, while values between 12 and 25 mmHg indicate the need for observation and serial assessments.[2]

Fig. 8. Thoracic and abdominal escharotomy
Surgical excision
Indications:
Surgical excision of burns with or without skin grafting is employed in the treatment of most full thickness burns, and often in patients with burn TBSA greater than 10%. Early excision (as early as 1 day post injury) and grafting reduces the length of hospital admission, improves long-term functional and cosmetic outcomes, and results in a better cost-benefit ratio.[47][48]
Types of surgical excision:
Surgical excision of burns may be described based on time (i.e. how long has elapsed since the burn injury) and based on depth of the excision.
- By time elapsed since injury:
-
- Early excision is the removal of necrotic tissue before invasive infection begins; however, the length of time is not universally defined and generally ranges from the first week to a maximum of 10 days after trauma; it is also dependent upon timing/onset of diuresis.
- In late excision, a greater length of time is allowed to pass in order to allow for the observation of areas that are evolving, either toward repair or conversion to deeper injury. This period of time is also not defined, but generally ranges from 10 to 21 days. However, in the presence of infection, imminent surgical intervention is indicated.
- By depth:
-
- Tangential excision is a sequential strategy whereby pieces of necrotic tissue are gradually removed until viable tissue is exposed.
-
Total excision, also called fascial excision, is the removal of the burned tissue in addition to the subcutaneous tissue at a predetermined depth; it is normally performed to the level of the deep fascia for full-thickness burns.[2]
- Dermal preservation during excision is crucial in order to obtain better healing and scar outcomes. Although standard of care remains early tangential excision through sharp excision with a knife or guarded straight blade, current evidence does not show superiority of one tool over another. As for methods, options besides sharp excision with knives/blades include enzymatic debridement (e.g. NexoBridTM, UK) or hydrosurgery (e.g. Versajet).[49]
- Geographic location and size of burn unit, staff experience level, and provider board certification, can contribute to variations in practice. A survey by the American Burn Association showed that among respondents, 56% of surgeons will perform excision as early as post-burn day 1 and 73% will excise greater than 20% TBSA in one setting.[50]
IMPROVED HEMOSTASIS DURING EXCISION AND GRAFTING OF BURNS
Strategies that may contribute to improved hemostasis include.[2]:
- Infiltration of the subcutaneous tissue below the eschar of the burn and the donor site with a solution containing epinephrine, or the topical application of a solution containing epinephrine, or both;
- Use of tourniquets when limb surgery is performed;
- Prevention of hypothermia;
- Use of compression dressings and limb elevation;
- Total excision with electrocautery when indicated;
- Limiting area of excisions and length of procedure.
Wound coverage with autologous skin grafting
Indications
-
For full-thickness and deep partial thickness burn injuries: autologous skin grafting (Figures 9 to 18) has been shown to substantially improve outcomes compared to scar formation from healing by secondary intention. The accelerated healing of full-thickness burns afforded by skin grafting results in expedited patient recovery and reduces the incidence and severity of contractures. The benefits of skin grafting for full-thickness burns are so evident that there is a scarcity of controlled research to provide proof for these benefits.[51]
Types of autologous skin grafts
- Sheet: considered by many as the gold standard for coverage of burn wounds of up to 20% TBSA. Sheets are partial thickness skin grafts, harvested with pneumatic dermatomes (Figures 9 and 10) or special skin graft knives. Sheets offer superior cosmetic results compared to meshed grafts and are preferred for cosmetically sensitive areas such as face, neck and hands (Figures 11-16). Disadvantages of sheet skin grafts include the creation of a donor site scar (Figure 17) and the potential for collecting hematoma under the sheet, resulting in partial graft loss.[52]
- Meshed: sheet skin grafts may be fenestrated with a mechanical meshing device and become “meshed” (Figure 18). Meshing allows for expansion of the graft and coverage of larger surfaces in the burn patient while using relatively smaller donor sites when compared with sheet grafting. Common mesh ratios include 2:1, 1.5:1, and less commonly 1:1, but expansions of up to 9 times are sometimes needed in patients with extensive burns and limited donor sites. Fenestrations in the graft allow exudates to drain, decreasing the risk of hematoma formation and graft loss. Disadvantages include worse scarring compared to sheet grafts (usually following a “meshed” pattern).[52]
 Fig. 9. Dermatome |  Fig. 10. Dermatome. Harvest of a split-thickness skin graft |
 Fig. 11. Full-thickness burn injury on right forearm and hand |  Fig. 12. Sheet split-thickness skin grafts on right hand
|
 Fig. 13. Same patient shown in Figure 11, 3 months after sheet split-thickness skin grafts
|  Fig. 14. Range of motion preserved after sheet split thickness skin grafts
|
 Fig. 15. Deep partial thickness burn injury on face and neck
|  Fig. 16. Deep partial thickness burn injury on face and neck 2 months after sheet skin grafting |
 Fig. 17. Split-thickness skin graft donor area, right thigh | 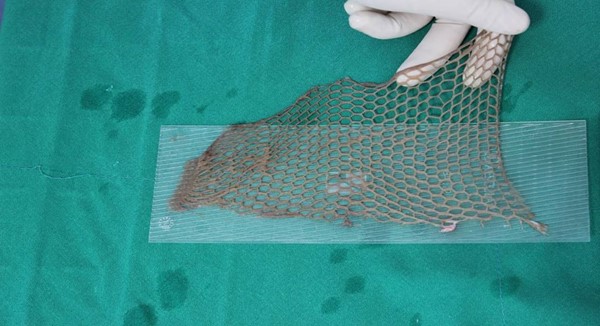 Fig. 18. Appearance of a meshed skin graft |
AUTOLOGOUS SKIN CELL SUSPENSION
Recently, devices have been approved by the FDA for preparation of autologous skin cell suspension at the point-of-care using a small sample of the patient's skin (e.g., Recell).
- Indications: autologous skin cell suspension is indicated for direct application on acute partial-thickness burn wounds or application in combination with meshed autografts for acute full-thickness thermal burn wounds. Potential benefits include minimization of donor skin harvesting requirements and enhancement of re-epithelialization of widely meshed skin grafts.[53][54]
- An industry-sponsored cost-effectiveness study concluded that use of autologous skin cell suspension compared to standard of care may reduce hospital costs and length of stay of severe burns in the U.S.[55]
Fasciotomy
In deeper burns (e.g. full thickness burns), especially in those caused by high-voltage electricity, early fasciotomy is indicated in the extremities to preserve perfusion and function (Figures 19 and 20). Necrotic tissue must be totally removed - particularly necrotic muscle which may cause potentially fatal cardiac, renal, and infectious complications, which could be prevented with aggressive burn excision. In some cases, amputation of a limb or a severely-compromised portion of it could be a life-saving measure.[2]
Fig. 19. Full-thickness burn caused by high-voltage electricity on right hand

Fig. 20. Same patient shown in Figure 16. Fasciotomy was required to treat acute carpal tunnel syndrome due to compartment syndrome
Plan Reassessment
Patient follow up intervals vary by case, but generally:
- For superficial burns: treated as an outpatient with visits every 5 days
- For superficial partial thickness burns: may be treated as outpatient or inpatient, depending on severity and location of the burn injury (see Table 1). If treated as an outpatient, follow up visits usually scheduled every 2-3 days
- For deep partial thickness or full thickness burn injuries: patients are usually admitted to the hospital depending on severity and location of the burn injury (see Table 1), with daily or more frequent assessments.
Plan reassessment may happen at every visit or dressing change due to the dynamic nature of this acute condition, however use of adjunctive therapy may be indicated only when standard therapy fails to promote desired outcomes.
Adjunctive Therapy
Biophysical interventions
Negative pressure wound therapy
- For wounds that do not require grafting, Negative Pressure Wound Therapy (NPWT) has been reported to facilitate epithelial closure. [56][57] NPWT has also been used to promote engraftment (AKA "graft take") of split-thickness skin grafts by bolstering, or enhancing immobilization of the grafts.[57][58] Nevertheless, evidence supporting use of NPWT to promote healing of burn wounds is of low certainty, derived primarily from case reports and retrospective studies. Randomized controlled clinical trials are needed to validate any putative benefits of NPWT in burns.[57]
Hyperbaric oxygen therapy
- For burn patients with carbon monoxide toxicity due to inhalation injury, Hyperbaric Oxygen Therapy (HBOT) is recommended as administration of supplemental oxygen has long been the cornerstone of therapy for patients suffering CO poisoning. See HBO topic "Acute Carbon Monoxide Poisoning"
- For severe burn patients, adjunct HBOT 24-48 hours after injury has been studied for its potential to promote faster wound healing, decrease pain and prevent partial to full-thickness conversion.[59][60][61][62] However evidence to date is not sufficient to justify widespread routine use in clinical practice. Studies have been mostly carried out in animal models, and the few randomized controlled trials (RCTs) published so far have contradictory results.[61]
Wound Coverage
Cellular and/or Tissue Products
Cellular and/or Tissue Products (CTP), also referred to as skin substitutes, have been long utilized in burns. CTPs were originally designed to replace autologous skin grafts in the treatment of burns and chronic wounds.[63]
For the management of partial thickness burns, evidence derived from RCTs suggests that:
- Bioengineered skin substitutes, namely Biobrane, TransCyte, Dermagraft, and allogeneic cultured skin, are at least as efficacious as topical agents/wound dressings or allograft. [64]
- Apligraf combined with autograft is at least as efficacious as autograft alone.[64]
- Suprathel, a polylactide-based copolymer, was shown to result in satisfactory skin quality and scar formation outcomes for deep dermal burns as compared with autologous skin.[65] Another study compared Suprathel with Omiderm and concluded that although less cost-effective than Omiderm, Suprathel provided more patient comfort. [66]
For the management of full thickness burns, evidence derived from RCTs suggests that:
- In a 3-arm comparison among Integra(®), viscose cellulose sponge Cellonex™ or partial thickness skin autograft, all treatments after 12 months demonstrated equal clinical appearance, as well as histological and immunohistochemical findings.[67]
- When compared with cadaveric skin allograft, Integra for treatment of full-thickness burns in pediatric patients was associated with statistically significant superior outcomes upon long term follow up (2 years). Outcomes included improved scarring in terms of height, thickness, vascularity, and pigmentation.[68]
- For chronic burn wounds, amniotic membrane (fresh, lyophilized and/or irradiated) showed superiority in increasing the success rate of graft take in chronic burn wounds compared to conventional dressing.[69]
Biologics
Cell-based therapy utilizing mesenchymal stem cells (MSCs), also known as mesenchymal stromal cells, is still considered experimental. Cell-based therapy with MSCs is currently being investigated as a therapeutic avenue for severe thermal burns, due to their ability to repair and replace cellular substrates, attenuate inflammation, increase angiogenesis and enhance migration of reparative cells. [70] Randomized clinical trials underway include studies evaluating use of MSCs to accelerate healing in patients with <20% TBSA partial thickness burns (NCT02104713) and in patients with partial or full thickness burns needing autologous skin grafts (NCT03113747).[71]
CURATED ARTICLES