INTRODUCTION
Overview
This topic provides resources for starting or further developing a limb preservation program. For more on challenges and solutions when building a limb preservation program, watch the interview "Building a Limb Preservation Program: Challenges and Successes".
The scope of the problem
The ultimate goal of limb preservation programs is to restore pulsatile blood flow to an at-risk extremity and prevent major lower extremity amputation. Unfortunately, the literature shows that the vast majority of non-traumatic amputations are preventable.[1] More than 400 non-traumatic lower limb amputations are performed per day in the United States.[1] As many as 50% of those non-traumatic lower extremity limb amputations are associated with diabetes.[2]
There is a broad continuum of care for the limb preservation patient that ranges from limb preservation, limb salvage, wound care, palliative care, to end-of-life care. Throughout the continuum, there are significant differences in the care received for those at risk for limb loss. In fact, patients frequently move from one level of care to another based on the severity of vascular occlusion in the at-risk extremity, complications arising during treatment, and overall health status.
These variations in care and outcome are based on many factors that may include access to care, geographic location, and socioeconomic concerns. For instance, among patients with chronic limb threatening ischemia, up to 50% of patients who undergo a major lower extremity amputation never have a thorough vascular assessment in order to evaluate the potential for limb preservation.[2]
In 2017 Neville and Kayssi looked at the role of hospital networks, tertiary care hospitals, and community-based programs in managing limb preservation.[2] These authors described the benefits of limb preservation programs for both patients and medical providers [2]:
- For patients, benefits include rapid assessment, improved healing, and enhanced revascularization.
- For providers, advantages include the ability to efficiently manage complex patients with help from the appropriate specialties (a multi-disciplinary team), an increase in referrals, enhanced identity of the institution, and opportunity to participate in clinical research and therapeutic trials.
GOALS OF LIMB PRESERVATION
So, what is the primary goal in limb preservation?
Globally, the healthcare system attempts to deliver the highest quality of care with the best outcome that can be administered in a time-efficient and cost-effective manner. In reality, global healthcare is administered on an individual basis.
As the patient navigates the healthcare system in an effort to “save his/her limb”, access to a multidisciplinary team with expertise and commitment in limb preservation is effective in preventing lower extremity amputation.[3][4]
More specifically, to meet those needs we must:
- Have a dedicated multidisciplinary team focused on limb preservation
- Have access to care that is based on acuity
- Have a broad toolbox that includes both interventional and non-interventional capabilities to manage these patients
Goal 1. Identify the patient with an at risk limb
The first priority of a limb preservation program is early identification of patients with at-risk limbs. To do so, it is crucial to have a simple and efficient triaging system in place throughout the healthcare system.
Classifying a patient's urgency of care may be one way to proceed. A classification of the lower extremity as emergent, urgent or routine care can be utilized when screening patients. Having a clearly defined clinical pathway for each category with appropriate and timely referrals based on the level of acuity is vital. In order to achieve this goal, education of the primary care providers throughout the healthcare system is critical.
Follow-up education on an annual basis is also necessary.
Goal 2. Track, manage and follow up every patient with an at risk limb
The next step is to establish a way of tracking and following patients. Developing a tracking system to assure appropriate follow up, compliance and identifying any potential delays of care is an imperative.
Having an appropriate electronic medical record that can capture the data, then interfacing with an appropriate wound registry is also a high priority.
So, whether the patient first presents in the emergency department, urgent care center, or primary care physician office, the patient will be treated the same way throughout the healthcare system.
Triaging and tracking in practice
Ideally, a ‘limb preservation hotline’ staffed by a trained, dedicated clinician (e.g,. a nurse), is established and is available to all departments within the community and healthcare system. Whenever a clinician refers an at-risk patient, the nurse triages and dispatches the case according to the urgency of care.
The nurse keeps track and documents all cases and their ultimate disposition. The nurse then can follow up with the patient and referring provider in order to ensure that the patient is seen in a timely manner.
In addition, the record and database of each patient outcome stands as a quality assurance indicator for limb salvage.
MULTIDISCIPLINARY TEAM AND CARE COORDINATION
A limb preservation program requires the coordinated effort of physicians, nurses, allied health professionals, and healthcare administrators dedicated to the preservation, restoration and salvage of functional limbs. Adoption of a multidisciplinary clinical team has been shown to decrease major amputation rates by more than 50%, decrease wound healing times and to increase wound healing rates.[1][5] The key to a successful program is cooperation and communication among the participants who have a single goal of limb preservation. This process depends on the vision and zeal of a limb salvage champion. This role can be filled by any full-time, trained clinician. In many successful centers, this figure is a podiatrist, vascular surgeon, plastic surgeon, or wound care physician. Having a limb salvage clinician champion is necessary in order to build a multidisciplinary team. Table 1 illustrates how members of the multidisciplinary clinical team contribute to the limb preservation program. [6]
Table 1. Multidisciplinary approach and full-time wound specialist clinician(s) are needed for a successful wound clinic with a focus on limb salvage program [6]
| Member | Contribution |
| Anesthesiology | Anesthesia induction in high-risk patients |
| Endocrinology | Glucose management |
| Hematology | Coagulopathy assessment and management |
| Hyperbaric medicine | Hyperbaric oxygen therapy |
| Internal medicine | Acute inpatient management |
| Infectious disease | Infection management |
| Interventional medicine (radiology, cardiovascular) | Assessment and endovascular intervention |
| Nutrition | Optimization of healing potential through counseling and supplementation |
| Orthotics/ Prosthetics | Orthotics, prosthetics, bracing |
| Physical therapy | Rehabilitation and mobility training |
| Plastic surgery | Soft tissue reconstruction and coverage |
| Podiatry | Wound care and surgical biomechanical management |
| Psychiatry | Behavior modification and psychological assessment |
| Rheumatology | Vasculitic and autoimmune response |
| Wound care | Wound management |
Other elements that are beneficial to a limb preservation program include [2]:
- An identifiable physical space
- A vascular laboratory
- Hyperbaric oxygen therapy
- Protocol-driven care involving diagnostic and therapeutic modalities such as endovascular revascularization, open bypass, and soft tissue reconstruction
- Prosthetic expertise in order to maintain function
- Comprehensive foot care and a remission clinic:
- Comprehensive foot care, including regular visits with a podiatrist, has been associated with reducing diabetes-related amputations by up to 80% [7]
- Three critical factors that contribute to reducing amputations are 1) patient education, 2) regular visits with doctor and/or podiatrist, 3) appropriate footwear [7]
Required skills for a successful limb preservation program
Table 2 illustrates eight collective clinical skills that are essential in a limb preservation program.[8] The accompanying list of selected WoundReference premium topics will help members of a limb preservation program build clinical skills. The WoundReference Competency Tool can be leveraged for optimal training and skill building (learn more about the tool).
Table 2. Eight collective clinical skills and selected topics for members of a limb preservation program [8]
Clinical Skills
| Selected WoundReference Topics
|
1. Ability to perform hemodynamic and anatomic vascular assessment with revascularization, as indicated
| |
2. Ability to perform neurologic workup
| |
3. Ability to perform site-appropriate culture technique
| |
4. Ability to perform wound assessment and staging/grading of infection and ischemia
| |
5. Ability to perform site-specific bedside and intra-operative incision and debridement
| |
6. Initiate and modify culture-specific and patient-appropriate antibiotic therapy
| |
7. Provide appropriate postoperative follow up to reduce risks of re-ulceration and infection
| |
8. Provide basic foot care education and referral into (and monitoring of) a home education program
| |
Other: Identify indications for HBOT
| |
OPERATIONS
Traditional models
Ideally, a limb preservation program will have a dedicated multidisciplinary team, and an all-inclusive/equipped clinic with administrative support that offers accessible and affordable care. There are many excellent limb preservation programs throughout the United States. Those programs offer care in a variety of clinical models. Most commonly, these programs are part of larger tertiary care hospitals with administrative support and most, if not all, of the resources mentioned above.
Some of the practices shared by some of these traditional limb preservation programs are listed below.
Clinical staffing
- Wound care centers have an essential role in the program. Ideally, wound care clinics are staffed with at least 1 full-time prescribing provider every day. Having a dedicated clinician present daily shows better outcomes than a ‘platoon’ staffing with multiple providers.
Referral flow patterns
Collaboration between vascular surgery and wound center
- Limb preservation programs that are based on the collaboration between a vascular surgery department and a wound center have demonstrated benefits for both parties.
- The standard of care on initial evaluation requires an appropriate vascular assessment. An abnormal vascular assessment requires immediate vascular surgical referral.
- As a result, the implementation of a limb preservation program leads to a medically justified increase in referrals between vascular surgery and wound clinic, which in turn allows both services to identify patients in need of interventions sooner (e.g., infrapopliteal bypass, debridements).[9]
Toe, flow and go model
The toe, flow and go is a model in which someone takes care of the foot medically and surgically, someone takes care of the flow into the foot medically and surgically, and someone manages wounds.[8]
There are four components for a successful program based on this model: foot hotline, wound healing clinic, remission clinic, and screening clinic (see Figure 1).[8]
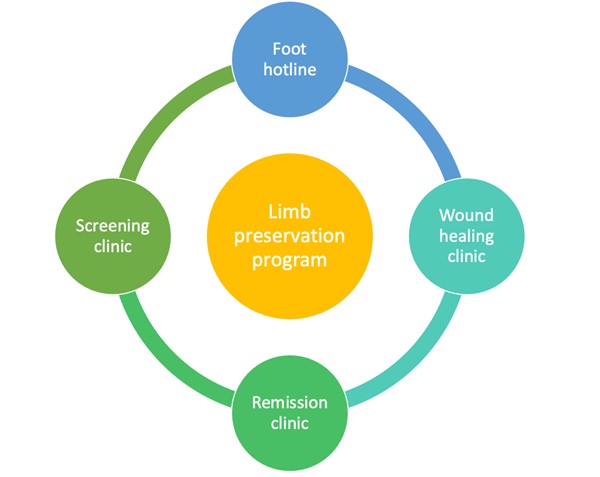
Figure 1. Four components of a limb preservation program (toe, floe and go) [8]
Non-traditional models
Although ideal, having a dedicated all-inclusive onsite limb preservation clinic that has Vascular Surgery, Interventional Radiology, Wound Care, Podiatry, Hyperbaric Oxygen Therapy, Vascular Testing, Orthotists, Physiatry, Research requires significant commitment and resources and is not always possible.
An alternative is to offer care in a community based, ambulatory setting.
For communities with no formal limb preservation programs, clinicians can still develop a virtual limb preservation program. In a virtual limb preservation program, a wound center or podiatry clinic can act as a central hub for the management of these patients. Key elements include:
- Development of a clearly defined relationship with a multidisciplinary team within the community of medical providers and medical resources
- An appropriate and timely referral pathway to a higher level of care when indicated
- Understanding of both quality and safety measures
- Development of an appropriate mechanism to document and track various metrics of quality of care.
- Collecting data that is tracked and monitored in a wound registry is another way to evaluate the quality of an individual program.
For more information on virtual limb preservation programs, watch the interview "Building a Limb Preservation Program: Challenges and Successes".
RESOURCES
Limb Preservation Alliances
Several limb preservation societies and foundations are devoted to the global goal of a standardized approach to limb preservation care (see sample below). Those entities offer a network of resources as well as serve as a vehicle to network amongst colleagues with similar goals, such as conferences and workshops that address concerns and best practice models of limb preservation.
Resources for Patients
WoundReference Clinical and Reimbursement Decision Support
Wound Reference is an accessible, comprehensive resource with evidence-based, always current information on the role of wound care, hyperbaric oxygen therapy and the multidisciplinary approach to limb preservation.
SUMMARY
A successful limb preservation program has a visible and identified limb preservation champion. This clinician takes the lead in building a multidisciplinary team that operates with tight guidelines with best-practice care coordination. Another key pillar is administrative support and commitment to building and maintaining such a program.
Having it all is often a challenge, given common scenarios of limited resources that may result in decreased patient access. This challenge is further intensified during public health emergency situations, such as the one observed in the COVID-19 pandemic.
As medical resources are both vital and limited, it is imperative that at-risk patients are identified and managed along the limb preservation continuum of care, which includes limb preservation, limb salvage, wound care, palliative care and end of life care. Early identification and appropriate management of these patients can reduce morbidity and mortality, and improve patient outcomes and quality of life. Ambulatory patients have greater longevity than those who lose limbs, and hence, lose mobility. [4]
CURATED ARTICLES
Official reprint from WoundReference® woundreference.com ©2026 Wound Reference, Inc. All Rights Reserved
NOTE: This is a controlled document. This document is not a substitute for proper training, experience, and exercising of professional judgment. While every effort has been made to ensure the accuracy of the contents, neither the authors nor the Wound Reference, Inc. give any guarantee as to the accuracy of the information contained in them nor accept any liability, with respect to loss, damage, injury or expense arising from any such errors or omissions in the contents of the work.