The following hyperbaric medicine treatment protocol is based upon the recommendations of the Hyperbaric Oxygen Committee of the Undersea and Hyperbaric Medical Society. Clinical protocols and/or practice guidelines are systematically developed statements that help physicians, other practitioners, case managers and clients make decisions about appropriate health care for specific clinical circumstances.
These protocols allow health providers to offer evidence-based, appropriate, standardized diagnostic treatment and care services to patients undergoing hyperbaric oxygen therapy (HBOT). This section discusses acute traumatic ischemia, crush injury, and compartment syndrome. Evidenced-based medicine offers clinicians a way to achieve improved quality, improved patient satisfaction, and reduced costs. Utilization Review should be initiated when clinical decisions result in deviation from or modification of treatment protocols. This includes any course of treatment at or above the recognized threshold limits.
| Acute Traumatic Peripheral Ischemia |
Sample Physician Order | $ ICD-10 Crosswalk | Treatment Table | Emergent / Urgent Indication
|
| Crush Injury/Compartment Syndrome |
Sample Physician Order | $ ICD-10 Crosswalk | Treatment Table | Emergent / Urgent Indication
|
| Background | - Acute traumatic ischemia occurs when there is a severe injury to a limb that results in compromise of the arterial blood supply or perfusion differential pressure to that limb.
- The injury can be soft tissue only with disruption of the major arterial flow to the at risk/injured tissue. It may also involve fractured bones and/or disrupted joints, thus putting an extremity at risk.
- The immediate and emergent threat is determined by whether perfusion of the limb is sufficient to maintain viability of the downstream tissues.
- The pathophysiology is a picture of vasogenic edema as a consequence of the physical injury
- Compromised host responses to infection and ischemia
- Decrease in phagocytic ability of white blood cells
- Decrease in collagen secretion by fibroblasts
- Impairment of neovascularization due to hypoxic tissue
- While crush injuries are a direct result from trauma, skeletal muscle compartment syndromes arise from ischemia, venous outflow obstruction, exertion, external compression, or trauma [2]
- Acute traumatic ischemia, crush injury, and compartment syndrome are amenable to HBOT. However, HBOT must never be used as an excuse to delay a fasciotomy in the established skeletal muscle compartment syndrome.
- These are critically ill patients, many of whom are in the ICU, intubated, ventilated, and require aggressive fluid and pressor resuscitation.
- You must be comfortable treating critically ill patients in your chamber environment. If you cannot, then these patients should be transferred to a higher level facility as soon as they are stable.
|
|
Goals of HBOT
|
- Serve as a bridge and adjunctive therapy until definitive surgical intervention by:
- Increasing tissue oxygenation concentration to prevent cellular death
- Reducing ischemia-reperfusion injury
- Supporting host defense function of white blood cells in generating granulation tissue and fighting infection
- Preventing WBC degranulation, thus preventing clotting and inflammatory cascade complications:
- Increased edema
- Increased transudate
- RBC Rouleaux formation and capillary clogging
- Activation of the clotting cascade
- Enhance blood supply by:
- Supporting neovascularization through stimulation of collagen secretion by fibroblasts and macrophages
- Decreasing edema in injured tissue
|
|
Diagnosis
|
Acute traumatic peripheral ischemia- History of trauma to the affected area (e.g., blunt, penetrating, laceration)
- "Hard" signs of arterial injury:
- Active hemorrhage
- Expanding or pulsatile hematoma
- Arterial vibration upon palpation
- Bruit near or over the artery upon auscultation
- Six Ps of acute ischemia: pain, pallor, poikilothermia, pulselessness, paresthesia, and paralysis
Crush injury - History of trauma to the affected area
- Typically presents with involvement of multiple tissues (skin, subcutaneous tissue, muscles, bones, nerves, vessels)
Skeletal muscle compartment syndrome - History of severe trauma, especially involving crush injuries or fractures of long bones of the arm or leg
- Pain levels disproportionate to apparent injury
- Tense muscle compartment, painful to passive extension of affected limb
- Increased measured intra-compartmental pressure (not required for diagnosis)
- 5 P's:
- Pallor, paresthesias, pulse deficit, paralysis, and pain on passive extension of the compartment
- Pain is usually very severe and occurs early
- Paresthesias may occur early as well
- Paralysis is a late sign
- Pulse loss is a late sign
|
Hyperbaric Criteria
| - Diagnosis of acute traumatic peripheral ischemia or crush injury
- Ischemic limb or tissue, at risk of amputation
- Treatment or prevention of ischemia-reperfusion injury
- Compartment syndrome in the impending stage (e.g. symptoms of compartment syndrome with no indication for fasciotomy). Indications for HBOT include (Figure 1):
- 3 or more clinical of the following findings: increasingly severe pain, paresthesia or anesthesia, muscle weakness, discomfort with passive stretch, tenseness of muscle compartment, OR
- 1 of the following manometric findings:
- Increasing compartment pressures with serial measurements AND/OR
- <= 45mmHg in "healthy" patient
- <= 35mmHg in "impaired" patient
- <= 25mmHg in "decompensated" patient
- Compartment syndrome in the established stage (i.e. with indication for fasciotomy) after fasciotomy has been performed. Specific indications for HBOT post-fasciotomy include presence of 1 or more of the following findings:
- Ischemic muscle, unclear demarcation between viable/non-viable tissue, prolonged swelling/ischemia time, threatened skin flap/graft, residual neuropathy, markedly impaired or decompensated patient
|
Evaluation
| - History: if possible have patient relay a detailed history of the mechanism of injury (traumatic vs non-traumatic event), presence of diabetes and vascular disease
- Physical examination: assess if cardiovascular instability, renal failure, metabolic acidosis, disseminated intravascular coagulopathy, hypothermia, myoglobinuria, skin injury and swelling, paralysis, and paresthesia
- Initiate tetanus prophylaxis if necessary
- Labs to order or review:
- Complete Blood Count (CBC)
- Comprehensive Metabolic Panel (CMP)
- Creatinine phosphokinase (CPK)
- Urinalysis; urinary myoglobin
- Arterial Blood Gas (ABG)
- Electrocardiogram (ECG)
- Chest X-ray
- Review current clotting studies
- Photograph extremity for signs of continued hypoxia or demarcation.
- Anaerobic and aerobic wound cultures
- Compartment pressure measurement (if applicable)
- Consult with surgeon for surgical intervention and debridement as necessary
- Transcutaneous oxygen (TCOM) assessment, if indicated
|
Treatment
| - Early application of HBOT within 4-6 hours of injury is recommended.
- Hyperbaric oxygen therapy, at 2.0-2.4 ATA oxygen for 90 minutes (Table 1). Use 2.4 ATA if an ischemia-reperfusion component has occurred, which requires two 5-10 minute air breaks (Table 3).
- Treat three times within the first 48 hours for critical ischemias, if possible. Logistics in critically ill patients frequently do not allow this schedule.
- Treat twice daily after 48 hours until the tissue at risk stabilizes or amputation is inevitable.
- Daily HBOT may be given once the injured tissue is stable and the neovascular status is improved.
- If the tissue begins to show evidence of recurring ischemia or progression of tissue destruction, twice daily treatments can be extended or renewed.
- These patients are typically in inpatient settings receiving critical care, therefore, blood pressure (arterial line), central pressures (Swan Ganz), ECG, and urinary output may be monitored, as directed.
- Aggressive fluid resuscitation is the mainstay of treatment for crush injury. The earlier fluid resuscitation is started, the more likely acute renal failure will be prevented.
- Crystalloid or colloid resuscitation for trauma is best left to the intensive medicine physicians. Be aware that there are significant fluid shifts in the first 3-5 days after major trauma.
- Photograph for signs of continued hypoxia even if vital signs are initially normal.
- Re-evaluate and document daily.
- Transcutaneous oxygen assessment if indicated. This may require in-chamber TCOM measurement.
|
Follow-Up
| - Repeat wound photography, usually weekly, but daily initially can be helpful
- Repeat transcutaneous assessment, if amenable
|
Treatment Threshold
| 3 – 9 treatments (Peer review should be based on the pathophysiology of the indication and the number of HBOT treatments needed to mitigate it. While the number of treatments is variable due to the extent of trauma, peer review is important for assessment of HBOT effect. The decision whether to extend HBOT treatments or stop them should be the consensus of the HBOT physician, the trauma/orthopedic surgeon, the plastic/reconstructive surgeon, and or the primary care physician.)
|
Coding
| Refer to the ICD-10 Guideline for the appropriate ICD-10 code
|
Comments
| - There are two trauma grading scales in current use. The Gustilo Scale applies:
- Grade III makes up the injuries amenable to HBOT. Grade I and II injuries are generally not limb threatening.
- IIIA There is no arterial injury and sufficient tissue remains to close the injury primarily (Does not usually require HBOT)
- IIIB Exposed bone remains. Will require secondary coverage.
- IIIC With concomitant injury to major blood supply.
- Be aware that there is a 50% complication rate with Gustilo IIIB/C injuries, including:
- Osteomyelitis
- Fracture non-union
- Failed tissue flaps
- Amputations
- The second grading scale is usually an academic or research scale: The Johansen Mangled Extremity Severity Score (MESS).
- Scores > 7 predict most severe injuries, amputations, and poor outcomes.
- If diabetes mellitus is present, blood glucose should be checked within an hour prior to treatment and immediately post-HBOT.
- Avoid petroleum-based dressings and ointments whenever possible. If these are a necessary part of the surgical dressing, ensure that they are not exposed to air and are completely covered with 100% moistened cotton during HBOT.
- There is one randomized controlled trial using HBOT in severe trauma/crush injury patients. The HBOT group required fewer surgical exposures and had less amputations than the sham/control group. [3]
- For severe traumatic ischemias, use of the Wellness Score along with the Gustilo classification can help decision making on whether to engage in primary amputation or limb salvage (e.g. HBOT) (see Tables 1 and 2)
|
Primary Sources: Whelan and Kindwall [4], Moon [5], Thom [6], Bouachour [3], Strauss [7], Huang [8]
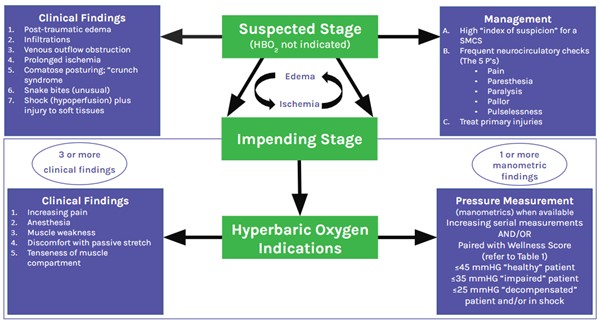
Figure 1: Indications for HBOT in the skeletal muscle-compartment syndrome [7][8]
The skeletal muscle-compartment syndrome starts with an injury or an insult (see findings in Suspected Stage above). If the edema-ischemia “vicious cycle” progresses, the 'Suspected Stage' evolves to the 'Impending Stage'. HBOT helps mitigate the edema-ischemia "vicious cycle" progression.
Table 1: The Wellness Score - Quantifying Health and Function [8]
Note: Five aspects as shown above are assessed to determine how healthy and functional the patient is. Each aspect is graded from 2 points (best) to 0 points (worst) and added to generate a score that can vary from 0 to 10. "Healthy" patients generate scores in the 7½ - 10 range, "impaired" patients in the 3½ - 7 range and decompensated patients in the 0 - 3 range.
| Assessment (Use half points if mixed or intermediate between 2) | 2 Points
| 1 Point | 0 Point |
| Activities of daily living | Full | Some | None |
| Ambulation (Subtract ½ point if aids are used) | Community | Household | None |
| Comorbidities (Omit neurological deficits which is separate assessment below) | No significant | Impaired | Decompensated |
| Inhibitors (smoking, collagen vascular diseases, and immunosuppressors) | None | Past | Current |
| Neurological deficits | None | Some/Minor Sensation, imbalances | Major Cognitive, paralysis |
Table 2: Guidelines for using Hyperbaric Oxygen in Crush Injuries using the Gustilo Classification Paired with the Patient's Wellness Score [8]
The Wellness Score is used alongside the Gustilo open fracture grading system to provide objective guidance on the use of hyperbaric oxygen therapy (HBOT) for crush injuries. ¹ A Wellness Score above 4 points (indicating healthy or impaired hosts) supports efforts to salvage injured tissue, including the adjunctive use of HBOT. ² Complications may include infection, delayed or non-union of fractures, and amputation. Amputation is generally indicated in cases of significant soft tissue loss, non-correctable ischemia, absence of healing, uncontrollable deformity, or intractable pain. ³ Consider primary amputation based on injury severity (Gustilo Type) in combination with the Wellness Score.
| Gustilo Type | Findings (Soft tissue injury with the fracture) | Outcomes in Healthy Hosts
| Healthy (HBOT Indications paired with Wellness Score¹) | Impaired (HBOT Indications paired with Wellness Score¹) | Decompensated (HBOT Indications paired with Wellness Score¹) |
| I | Minimal (<1 cm wide) puncture wound from inside to out | Usually no different from a closed fracture of the same severity |
|
| Yes |
| II | Laceration with minimal deep soft tissue damage | Same as above |
|
| Yes |
| III | Crush Injuries (Depends on Subtypes A, B and C) |
|
|
|
|
| A | Sufficient soft tissue to close the wound (after debridement) | ~10% completion rate² |
| Yes | Yes |
| B | Flaps and/or grafts needed for bone coverage | >50% incidence of complications² | Yes | Yes | Yes/No³ |
| C | III-B injuries with major vascular damage | >50% incidence of complications² | Yes | Yes/No³ | Yes/No³ |
DOCUMENTATION
History
Sample history for crush/traumatic ischemia is shown below:
"Peggy S. is a 26 y/o woman who was involved in an auto/pedestrian accident earlier this morning. She had a work truck malfunction along the highway. A second work truck was parked in front of her and offering assistance. She was standing on one leg with the other raised up to the bumper of her work truck. A 16 y/o driver in a car was distracted and crashed into the rear of Peggy's work truck at 50 mph. The ensuing destruction pinned Peggy's left leg between the two trucks. She was extricated and taken to the University Level 1 trauma center. Both orthopedic and vascular surgeons took her to the operating room to begin the process of saving her left leg.
Plain X-Ray and CT scan of the left leg revealed a compound, comminuted fracture of both tibia and fibula of the left leg. The tibial plateau of the left leg is shattered with a short section of tibia remaining. Should reconstruction fail, this short section of tibia and a shattered tibial plateau is unlikely to support a below knee amputation. Hence, should limb salvage fail, an above the knee amputation will be required.
In the operating room, the vascular supply at the trifurcation was disrupted requiring emergency bypass surgery and arterial repair by the vascular surgeons. This makes her trauma a Gustilo IIIC trauma score with a 50% likelihood of permanent injury and complications.
Her pertinent past history includes treated depression and body image disorder.
We have been asked to see Peggy and to provide hyperbaric oxygen therapy as an adjunctive therapy to assist limb salvage and healing her multiple fractures. We are happy to do so with a diagnosis of crush injury to the left lower leg."
[Note that compartment syndrome would be a similar history of closed leg crush, fracture, or injury with resultant impending/established compartment syndrome. Brief sample:
"John T. is a 36 y/o man with a short history of work injury this evening. A 400 pound piece of steel fell and trapped his right leg between the steel and bench. He did not sustain any fractures but came to the emergency room with a tight, swollen right leg below the knee. The emergency room physician measured compartment pressures using ultrasound and needle measurements. Pressures were at least 30mmHg higher than diastolic pressure in each compartment. He has been taken to the operating room for emergent compartment releases.
In the operating room, the surgeon noted that several muscles were hypoxic and dying. When stimulated by the electrical cautery, there was no muscle movement. Because of this finding, the surgeon asked us to provide hyperbaric oxygen in adjunctive fashion to attempt limb/muscle salvage. We will start therapy this evening with a diagnosis of acute, established compartment syndrome of the right lower leg."
Physical Exam
Acute traumatic peripheral ischemia
"Hard" signs of arterial injury:
- Active hemorrhage
- Expanding or pulsatile hematoma
- Arterial vibration upon palpation
- Bruit near or over the artery upon auscultation
- Six Ps of acute ischemia: pain, pallor, poikilothermia, pulselessness, paresthesia, and paralysis
Crush injury
- Typically presents with involvement of multiple tissues (skin, subcutaneous tissue, muscles, bones, nerves, vessels)
Skeletal muscle compartment syndrome
- History of severe trauma, especially involving crush injuries or fractures of long bones of the arm or leg
- Pain levels disproportionate to apparent injury
- Tense muscle compartment, painful to passive extension of affected limb
- Increased measured intra-compartmental pressure (not required for diagnosis)
5 P's:
- Pallor, paresthesias, pulse deficit, paralysis, and pain on passive extension of the compartment
- Pain is usually very severe and occurs early
- Paresthesias may occur early as well
- Paralysis is a late sign
- Pulse loss is a late sign
Impression
- Acute Traumatic Peripheral Ischemia Refer to ICD-10 Crosswalk
- Crush Injury Refer to ICD-10 Crosswalk
- Compartment Syndrome Refer to ICD-10 Crosswalk
Plan
A typical hyperbaric regimen for a traumatic ischemia consists of an aggressive treatment protocol. Patients will be treated at 2.0 or 2.4 ATA with oxygen breathing from 90 minutes. Initially, treatment will be twice daily. Once the extremity is stable and the neurovascular status is improved, treatments will be once daily for several days. If the tissue begins to show evidence of advancing ischemia or progression of tissue destruction, the twice daily regimen can be extended or renewed.
Risk and Benefit of Hyperbaric Oxygen Therapy
- Please refer to topic "Documentation HBO: Risks and Benefits"
Indication for Hyperbaric Oxygen Therapy (HBOT)
"Acute traumatic ischemia occurs when there is a severe injury to a limb that results in compromise of the arterial blood supply or perfusion differential pressure to that limb. The immediate, emergent threat is determined by whether perfusion of the limb is sufficient to maintain viability of the tissues. Crush injuries are directly associated with trauma while skeletal muscle compartment syndromes arise from ischemia, venous outflow obstruction, exertion, external compression, or trauma. There are 3 common features: 1) ischemia and hypoxia at the injury site, 2) a gradient of injury, and 3) the potential for self-perpetuation of the injury.
While hyperbaric oxygen is a useful adjunct, surgery and aggressive medical interventions will often be required in order to manage the condition. Conditions with related pathophysiology, which are also amenable to hyperbaric oxygen therapy, include threatened flaps, grafts, re-implantations, and frostbite. The pathophysiology is a picture of vasogenic edema as a consequence of injury exacerbated by cytogenic edema because the injured tissues are no longer able to maintain intracellular water. When tissue oxygen tensions fall below 30 mmHg, the host responses to infection and ischemia are compromised. White blood cell phagocytic killing becomes ineffective, fibroblasts are no longer able to secrete collagen, and neovascularization cannot occur.
Hyperbaric oxygen (at 2 ATA) increases blood oxygen content by 125%, where plasma and tissue oxygen tensions are increased by 1000%. Hyperbaric oxygen also induces vasoconstriction (decreasing blood flow by 20%), thus reducing edema. In this indication, hyperbaric oxygen enhances oxygen concentration at the tissue level, increases oxygen delivery per unit of blood flow, and reduces edema."
Sample Order
- See Sample Physician Order - Acute Traumatic Peripheral Ischemia
- See Sample Physician Order - Crush Injury/ Compartment Syndrome
CLINICAL EVIDENCE AND RECOMMENDATIONS
Hyperbaric Oxygen Therapy for Crush Injuries and Acute Traumatic Ischemia
- 1BFor patients with crush injuries and acute traumatic ischemias, adjunctive HBOT is recommended to mitigate resulting tissue damage, preferably within 4-6 hours of the injury. (Grade 1B)
- Rationale: HBOT increases oxygen availability to hypoxic tissues during the immediate post-injury period and increases tissue oxygen tension needed to support host response to trauma.[9][10] Use of adjunct HBOT for this indication is backed by moderate certainty evidence (level B), drawn from a positive randomized controlled trial (RCT) and over 600 case reports in more than 20 publications.[3][2][11][12][13][14] As one would expect, there is a great deal of variability in these case reports, such as: time from injury to HBOT, mechanism of injury, injury kinetic energy sources, and 'standard care.' We note that the vast majority of these cases improved with adjunctive HBOT. Improvements were more dramatic when HBOT was introduced early on after the injury, and injuries responded better when more than one HBOT treatment was undertaken in the first few days post-injury.
- For optimal results, HBOT should be initiated in those crush injuries where complications (e.g. flap necrosis, osteomyelitis) are predictable but not yet established, such as fractures Gustilo III-B and C, or lower Gustilo grades if the patient is impaired/decompensated.[9] However, we need to note that, on many occasions in daily clinical practice, clinicians are asked to provide HBOT for injuries that have already started to fail or other serious complications have appeared. Even then, the evidence will support the use of HBOT and encourage earlier intervention whenever possible.
- Coverage: Medicare covers adjunct HBOT for crush injuries and acute traumatic ischemia on an outpatient basis, but not for hospitalized patients.[1]
Hyperbaric Oxygen Therapy for Skeletal Muscle Compartment Syndromes
- 1CFor patients with skeletal muscle compartment syndrome (SMCS) in the impending stage (i.e., symptoms of SMCS with no indication for fasciotomy), adjunct HBOT is recommended to prevent progression to the established stage (i.e., SMCS with indication for fasciotomy). (Grade 1C)
- 1CFor patients with SMCS in the established stage, adjunct HBOT is indicated to prevent wound healing complications and promote recovery. (Grade 1C)
- Rationale: HBOT increases oxygen availability to hypoxic tissues during the immediate post-injury period and increases tissue oxygen tension needed to support host response to trauma.[9][10] Use of adjunct HBOT for this indication is backed by low certainty evidence (level C), based on expert opinion, experimental studies and case reports.[9][15][16][17][18][19] There are no RCTs in the area of extremity compartment syndromes. There are, however, multiple papers involving case presentations and case series that suggest early intervention with HBOT will be beneficial in preserving muscle in the injured compartment. Benefits of adjunctive HBOT outweigh the risks. Adjunctive HBOT is regarded as the only intervention with the potential to prevent progression of SMCS from the impending to the established stage.[9]
APPENDIX
Summary of Evidence
Crush Injuries and Acute Traumatic Ischemia
(back to text)
Systematic review
- In 2024, Kwee et al published a systematic review that aimed to evaluate the effectiveness of HBOT in the management of severe lower limb soft tissue injuries. A total of seven studies met the inclusion criteria, involving 229 patients. The studies included two randomized clinical trials, one retrospective cohort study, three case series and one case report. Authors concluded that HBOT is generally considered a safe therapeutic intervention and seems to have a beneficial effect on wound healing in severe lower limb soft tissue injuries when implemented as an addition to standard trauma care.[14]
Randomized controlled trial (RCT)
- In 2022, Millar et al. published a randomized controlled trial (n=120 patients) in which open tibial fractures were randomly assigned within 48 hours of injury to receive standard trauma care or standard care plus 12 sessions of HBOT. The primary outcome was the incidence of necrosis or infection or both occurring within 14 days of injury. Tissue necrosis occurred in 29% of HBOT patients and 53% of controls (OR 0.35, 95% CI 0.16 to 0.78, P = 0.01). There were fewer late complications in patients receiving HBOT (6/53 vs 18/52, OR 0.22, 95% CI 0.08 to 0.64, P = 0.007) including delayed fracture union (5/53 vs 13/52, OR 0.31, 95% CI 0.10 to 0.95, P = 0.04). Quality of life measures at one and two years were superior in HBOT patients. Authors concluded that in severe lower limb trauma, early HBOT reduces tissue necrosis and the likelihood of long-term complications, and improves functional outcomes.[20]
- In 1996 Bouachour et al. published a randomized, controlled, sham, blinded study using HBOT as an adjunctive addition to surgical care.[3] This is a complicated study because of the vagaries of trauma care. The HBOT intervention was 2.5 ATA and administered twice daily for 6 days post-injury. The results show dramatic improvement in the HBOT group (N = 36) and equally divided between sham and intervention groups. Complete healing occurred in 17 of the HBOT group and 10 of the sham. Additional surgical interventions (like skin grafts, vascular surgery, and/or amputation) was undertaken in 1 patient in the HBOT group and 6 in the sham group. The research group documented that regional perfusion indices (affected limb vs. non-affected limb) were consistently 0.9 or greater during HBOT, suggesting that episodic exposure to HBOT and increased oxygen to the injured area improved outcome.
CATEGORY A CONTINUING EDUCATION CREDIT
This topic has been reviewed and approved by the National Board of Diving and Hyperbaric Medical Technology (NBDHMT) for one (1) Category A Credit.
To claim the credit:
- 1. Read the topic
- 2. Answer the examination and course critique questions.
- Take the quiz via CliniPaths by Wound Reference
- To receive a certificate, a passing score of 70% is required
- 3. After passing, click the provided link to access your certificate. If prompted, sign into your WoundReference account.
For more information on Category A continuing education credits see blog post " Hyperbaric Certification and Continuing Education for Technicians & Nurses".
REVISION UPDATES
| Date | Description |
| 10/31/24 | Expanded section 'Treatment Protocol' |
| 4/24/24 | Updated references, enhanced “Comment” sections |
| 1/8/20 | Added section 'Category A Continuing Education Credit' |
| 4/29/19 | Added section on Documentation |
| 12/3/19 | Added section 'Clinical Evidence and Documentation', updated Table, section 'Hyperbaric Criteria' |