ABSTRACT
Diabetic Foot Ulcers (DFUs) are a chronic problem. Recurrence rates range from 8-59%[1] however, up to 75% of DFUs may be preventable. [2] Therefore, long-term maintenance must be addressed even for healed ulcers to prevent recurrence.
This topic provides a systematic approach to evaluating patients at risk for developing DFUs, primarily based on clinical guidelines by the International Working Group on the Diabetic Foot (IWGDF)[3] and the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine (SVS).[4]
- 1CAll people with diabetes, even those who never had a DFU before, should have a comprehensive foot evaluation at least annually (Grade 1C). The goal of the evaluation is to assess and classify risk of developing DFUs, so that preventative interventions can be implemented accordingly. Detailed foot assessments may occur more frequently in patients with histories of ulcers or amputations, foot deformities, insensate feet, and peripheral arterial disease (PAD). Simplified foot inspections should occur at every visit in all patients with diabetes.[5]
Preventative interventions include general measures (e.g., adequate glycemic control, treatment of pre-ulcerative signs), consults and referrals as needed, self-management (e.g, skin temperature monitoring), integrated foot care, offloading, and patient education. Indications and evidence of each preventative intervention according to risk category are provided below.
CLINICAL
Overview
Diabetic Foot Ulcers (DFUs) are a chronic problem. Recurrence rates range from 8–59% [1] however, up to 75% of DFUs may be preventable.[2] Therefore, long-term maintenance must be addressed even for healed ulcers to prevent recurrence. This topic provides a systematic approach to evaluating patients at risk for developing DFUs, primarily based on the clinical guidelines by the International Working Group on the Diabetic Foot (IWGDF) [3] and the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine (SVS).[4] All people with diabetes, even those who never had a DFU before, should have a comprehensive foot evaluation at least annually.[6] The goal of the evaluation is to assess and classify risk of developing DFUs, so that preventative interventions can be implemented accordingly.
For guidelines and quality measures related to DFUs, see topic "Diabetic Foot Ulcer - Overview". For an introduction and assessment of DFUs including epidemiology, risk factors, etiology, pathophysiology, history, physical examination, diagnosis, differential diagnoses, documentation and ICD-10 coding, see "Diabetic Foot Ulcers - Introduction and Assessment". For management of DFUs, see topics "Diabetic Foot Ulcer - Treatment", "Diabetic Foot Ulcer Associated with infection - Management","Diabetic Foot Ulcer Associated with Ischemia - Revascularization".
Frequency of foot evaluation
- 1CAll adults with diabetes should undergo a comprehensive foot evaluation at least annually by physicians (MD, DO, DPM) or advanced practice providers with training in foot care (Grade 1C).[3][7][8][4][5]
- Rationale: Identification of the high-risk foot is an essential component of diabetes care. It focuses attention and provides a means to direct limited resources to those patients most at risk of developing a DFU.[9] Detailed foot assessments may occur more frequently in patients with histories of ulcers or amputations, foot deformities, insensate feet, and peripheral arterial disease (PAD). Simplified foot inspections should occur at every visit in all patients with diabetes.[5]
Foot evaluation
- Clinical examination is useful in the classification and risk stratification of the disease for appropriate monitoring in a diabetic foot clinic.[5]
- A comprehensive foot examination, recommended at least annually for all patients with diabetes, is described in the section 'Assessment' in "Diabetic Foot Ulcer - Introduction and Assessment".
- A more simplified short evaluation can be used at every visit in all patients with diabetes [5]:
- Simplified 60 Second Diabetic Foot Screening Tool [10]
- Inlow's 60-second Diabetic Foot Screen [11][12]
- 3-Minute diabetic foot evaluation [13]
- See Quick Reference Guides 'Clinician Guide for the Diabetic Foot Exam' and the '60-Second Screen For The Diabetic Foot' below:
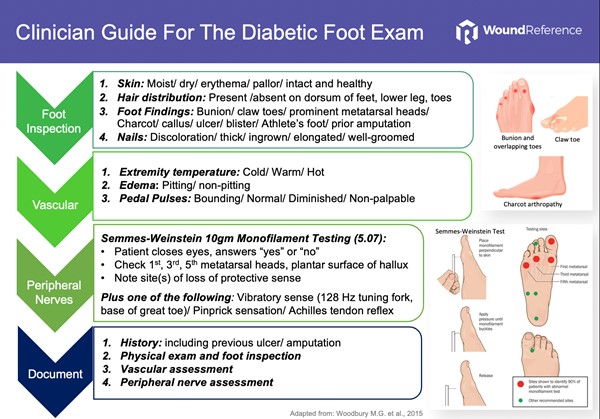
Quick Reference Guide 1: Clinician Guide for the Diabetic Foot Exam
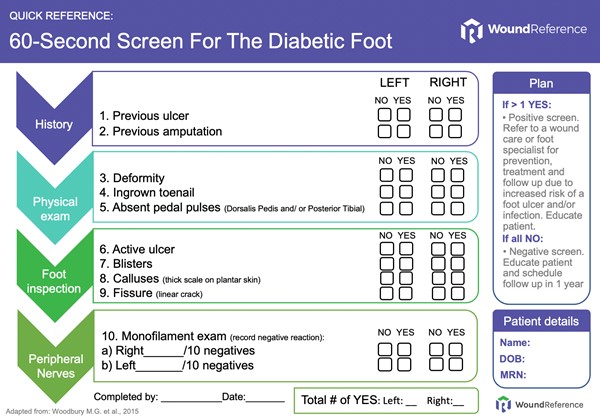
Quick Reference Guide 2: 60-Second Screen For The Diabetic Foot
Risk stratification tool
- Clinicians can choose among many risk classification tools.[6][7][8][9][12] Table 1 shows a risk stratification system developed by the International Working Group on Diabetic Foot (IWGDF) [3][14], along with ulcer and amputation estimated incidence per category, recommended follow up and preventative recommendations.
Table 1. The IWGDF Risk Classification System (2015), preventative screening frequency and interventions [3][7][9]
Abbreviations: LOPS, Loss of protective sensation; PAD, peripheral artery disease.
| IWGDF Category [3] | Characteristics [3] | Ulcer Incidence[9] | Amputation Incidence[9] | Follow up [3] | Preventative Interventions [3][7][9]
|
|
0
|
No LOPS and No PAD
|
2-6%
|
0
|
Once a year
|
General - Adequate glycemic control
- Treat pre-ulcerative signs or refer to foot specialist
Patient Education for Risk Category 0
|
|
1
|
LOPS or PAD
|
6-9%
|
0
|
Once every 6-12 months
|
General
- Adequate glycemic control
- Treat pre-ulcerative signs or refer to foot specialist
Self-management Footwear and offloading
- Properly fitted over-the-counter shoes and insoles or therapeutic shoes
Patient Education for Risk Category 1
|
|
2
|
LOPS + PAD, or LOPS + foot deformity or PAD + foot deformity
|
8-17%
|
1-3%
|
Once every 3-6 months
|
General - Adequate glycemic control
- Treat pre-ulcerative signs or refer to foot specialist
Consults/ referrals: - Vascular consultation if PAD
- Foot specialist if foot deformity
Self-management
- Self-care behavior
- Monitor foot skin temperature daily at home
Footwear and offloading - Properly fitted therapeutic shoes and insoles
Surgical procedures - Consider prophylactic surgery to correct deformity if deformity is not properly accommodated by shoes;
Patient Education for Risk Category 2
|
|
3
|
LOPS or PAD, and one or more of the following: history of a foot ulcer; a lower-extremity amputation (minor or major); end-stage renal disease
|
26-78%
|
10-18%
|
Once every 1-3 months
|
General - Adequate glycemic control
- Treat pre-ulcerative signs or refer to foot specialist
Consults/ referrals: - Vascular consultation if PAD
- Foot specialist if foot deformity
Self-management - Self-care behavior
- Monitor foot skin temperature daily at home
Integrated foot care - Professional foot treatment, adequate footwear and education
Footwear and offloading
- Properly fitted therapeutic shoes and insoles
Surgical procedures - Consider surgical offloading if DFU recurs despite adequate standard therapy
Patient Education for Risk Category 3 |
Preventative Interventions
The American Health Organization (PAHO) reported 3 key cost-saving health service interventions needed to fight diabetes in the Americas [9][15]: glycemic control in people with hemoglobin A1c >9%, blood pressure control in people with pressure >160/95 mmHG, and foot care in people with a high risk of ulcers. In the Western world, tight control with a target for hemoglobin A1c<7% and blood pressure < 130 /85 mmHg are suggested.[9] Foot care includes educating diabetic patients on recognizing and treating minor foot injuries, the use of appropriate footwear, and accessing knowledgeable health care personnel.[15]
General
For all patients with diabetes (IWGDF Categories 0-3)
- 2BFor all patients with diabetes, the Society for Vascular Surgery suggests adequate glycemic control (i.e., target hemoglobin A1c<7% with strategies to minimize hypoglycemia) to reduce the incidence of diabetic foot ulcers (DFUs) and infections, with subsequent risk of amputation (Grade 2B).[4]
- 1CFor all patients with diabetes with pre-ulcerative signs (e.g. callus, blisters, ingrown or thickened toe nails, fungal infections), the IWGDF recommends clinicians either treat the pre-ulcerative sign or refer to a foot care professional who can treat them (Grade 1C).[3]
- Rationale: Pre-ulcerative signs on the foot, such as callus, blisters or hemorrhage, appear to be a strong predictor of future ulceration and require immediate treatment by a foot care professional. The benefits of treatment of pre-ulcerative signs by a trained foot care professional outweigh the potential harm of such treatment and come at relatively low costs. [3]
For at-risk patients (IWGDF Categories 2 and 3)
- Consultation and follow up with specialists below are recommended [7]:
- Patients with peripheral neuropathy with foot deformity need a referral to a foot care specialist
- Patients with PAD need referral to a vascular specialist
Self-management interventions
For at-risk patients (IWGDF Categories 1-3)
- 2CFor at-risk patients, self-care behaviors should be included as part of an integrated foot care that includes professional foot care, education and therapeutic shoes and insoles.(Grade 2C).
- Rationale: Self-care behaviors include good foot care, daily foot and shoes inspection, daily foot washing (with careful drying particularly between the toes), avoidance of chemical agents or plasters to remove callus or corns, use of emollients to lubricate dry skin and cutting toenails straight across.[1][3][16] Good foot care and daily inspection alone without the other interventions will not reduce the recurrence of DFU.[1]
- 2BFor higher-risk patients (IWGDF Categories 2 and 3), the IWGDF recommends clinicians instruct patients to monitor foot skin temperatures at home to prevent a first or recurrent plantar foot ulcer. (Grade 2B)
- Rationale: The goal of temperature monitoring is to identify early signs of inflammation, so that timely action can be taken by patient and care provider to resolve the cause of inflammation.[3][16] There is moderate-certainty evidence (evidence level B) supporting use of infrared thermometer to prevent first or recurrent ulcer, by having the patient monitor plantar foot skin temperature on a daily basis, with subsequent preventative actions if elevated temperatures are noted.[3] However, cost-effectiveness is still unknown, and there are potential hurdles to adoption (e.g., calibrated equipment may be difficult to find, and patients - particularly those without an active ulcer - might see daily monitoring as a burden). [3]
Integrated Foot care
FOR AT-RISK PATIENTS WITH HISTORY OF ULCER OR AMPUTATION (IWGDF CATEGORY 3)
- 1CTo prevent a recurrent foot ulcer in an at-risk patient with diabetes, the IWGDF recommends clinicians provide integrated foot care, which includes professional foot treatment, adequate footwear and education (Grade 1C).[3] This intervention should be repeated or re-evaluated once every 1 to 3 months as necessary.[3]
Footwear and offloading devices to prevent DFU recurrence
For all patients with diabetes (IWGDF Categories 0-3)
- 1CFor all patients with diabetes, the IWGDF recommends clinicians instruct patients not to walk barefoot, in socks only, or in thin-soled standard slippers, whether at home or when outside (Grade 1C). [17]
For at-risk patients (IWGDF Categories 1-3)
- For at-risk patients (IWGDF Categories 1-3), the IWGDF recommends properly fitting footwear to prevent a first foot ulcer (Grade 1C). Patients with peripheral neuropathy only (IWGDF Category 1) and no calluses may wear properly fitting over-the-counter shoes and insoles; others should wear therapeutic shoes.[17]
-
- Rationale: There is some evidence that properly fitting footwear is effective in helping prevent DFU. Little harm has been reported from properly fitting therapeutic footwear, thus benefit likely outweighs potential harm.
- Medicare will not cover therapeutic footwear for patients with diabetes and peripheral neuropathy without evidence of calluses. Therefore if patient does not have calluses, patient may opt to wear properly fitting over-the-counter shoes and insoles instead. Patients who have not yet suffered from a DFU may be more inclined to wear regular over-the-counter shoes, as those are less bulky. [17]
-
1C For patients with diabetes at-risk of developing DFUs (IWGDF Categories 1-3), we recommend use of therapeutic shoes, custom-made insoles or toe-orthosis to prevent a first foot ulcer, either plantar or non-plantar, or a recurrent non-plantar foot ulcer. If foot deformity or pre-ulcerative lesion is present, therapeutic shoes are recommended (Grade 1C) [1][4][17]
- 1BTo prevent a recurrent plantar foot ulcer in an at-risk patient with diabetes (IWGDF Categories 1-3), the IWGDF recommends therapeutic footwear that can relieve plantar pressure during walking (i.e., 30% relief compared with plantar pressure using standard care therapeutic footwear) (Grade 1B) [17]
- Rationale: Few adverse effects have been reported, such that benefits outweigh potential harms. Patients need to be encouraged to constantly wear their therapeutic footwear, even at home. Unfortunately, patient adherence to prescription footwear is often insufficient and requires further attention to reduce the risk for re-ulceration.[17] If for religious, cultural reasons patients prefer not to wear same street shoes at home, a pair can be prescribed for indoor use (although a second pair in the same year will not be covered by Medicare). To ensure effective offloading, when resources allow, footwear should be designed or evaluated using plantar pressure measurement. Use of pressure measurement devices to ensure adequate offloading is likely cost-effective as it has been shown to reduce risk of ulcer recurrence by 50%.[17] If plantar foot pressure cannot be measured, clinicians should prescribe therapeutic footwear that effectively offload the foot. Medicare covers therapeutic shoes for patients with diabetes at higher risk of DFU. [18][19]
Preventative Surgical Procedures
For patients with PAD at higher risk of DFU (IWGDF Category 2 and 3)
- 1CFor patients at higher risk of developing DFU, but with no peripheral artery disease, the Society for Vascular Surgery recommends against prophylactic arterial revascularization to prevent DFU (Grade 1C, against).[4]
-
- Rationale: Assessment of ischemia as a factor contributing to development or non-healing of ulceration is essential. However, the neuropathy seen in diabetes is not primarily ischemic in nature, and there is no evidence that revascularization reverses ischemic neuropathy except in the setting of acute ischemia.[4] Thus, primary foot ulcerations in diabetic neuropathy are unlikely to be directly related to impaired large-artery blood flow; rather, they are related to abnormal gait and foot weight distribution. Indications for arterial revascularization should be based on the standard indications of severe claudication, rest pain, and tissue loss.[4]
- For patients at higher risk of developing DFU and foot deformity, consider prophylactic surgery to correct deformity if deformity is not properly accommodated by therapeutic shoes/insoles.[7]
-
For patients at risk of DFU recurrence (IWGDF Category 3)
-
2C For patients at high-risk of recurrence of DFU, with a plantar forefoot DFU that recurred despite adequate preventative interventions (e.g., therapeutic footwear), the IWGDF suggests surgical offloading to prevent recurrence (e.g. Achilles tendon lengthening, joint arthroplasty, single or pan metatarsal head resection) (Grade 2C) [17]
-
- Rationale: Interestingly, surgical offloading seems more effective in preventing than in healing ulcers.[17][20] However, due to the possible complications and side effects of these surgical offloading techniques (e.g. infection, gait problems, acute Charcot neuro-osteoarthropathy (CN), transfer ulcers) and also due to higher costs compared to non-surgical prevention, surgical offloading procedures should be considered only if standard offloading fails.
- For patients at high-risk of recurrence of DFU, with a toe DFU that recurred despite adequate conservative offloading, the IWGDF suggests digital flexor tenotomy to prevent recurrence (Grade 2C)
-
- Rationale: Evidence drawn from observational studies (evidence level C) support digital flexor tenotomy to prevent recurrence of toe DFUs, if standard offloading fails. This procedure can be performed in an outpatient setting and is not likely to have a negative impact on foot function.[17] See topic "Case: Surgical offloading of a lesser toe DFU with flexor tenotomy".
PATIENT EDUCATION (for clinicians)
Preventing first-time and recurrent DFUs
- 1C For all patients with diabetes (IWGDF Categories 0-3), we recommend repeated educational sessions aimed at improving foot care knowledge and adherence to foot care advice to prevent first or recurrent DFU (Grade 1C)
-
- Rationale: There is some evidence that short (1-hour) educational sessions on foot care do not decrease DFU incidence among patients with diabetes compared to patients who do not receive any education (Evidence level C).[21][22] However, there is also evidence that patients who are adherent to the advice given in the education program are at much lower risk of developing a first ulcer than those who are not adherent (evidence level C). [21] In order to be adherent to any advice though, patients need to be told and understand their role in foot care. As a result, clinical guidelines recommend clinicians provide education regularly.[3][4][17] Reinforcing foot care education to patients and their caregivers at every follow up visit is likely cost-effective[4], and considered a need for adequate foot care by the PAHO. [15]
- Patient education topics and frequency can be tailored according to which IWGDF risk category the patient falls under. See section 'Risk stratification tool' above. See Table 2 for suggested programs
Table 2: Suggested patient education program according to IWGDF Risk Categories [3][4]
|
Patient Education topics tailored to Risk Category IWGDF Risk Category (*)
|
0
|
1
|
2
|
3
|
|
Follow up frequency
|
1 x year
|
1 x 6 months
|
1x 3-6 months
|
1 x 1-3 months
|
|
Adequate glycemic control
|
|
|
|
|
|
Adequate foot protection - no walking barefoot, socks or thin slippers, indoors or outdoors
|
|
|
|
|
|
Early recognition of pre-ulcerative signs (e.g. callus, blisters, ingrown or thickened toe nails, fungal infections) and timely access to professional help
|
|
|
|
|
|
Proper shoe fitting
|
|
|
|
|
|
Self-management (basics of foot, callus and nail care):
- daily foot and shoes inspection,
- daily foot washing (with careful drying particularly between the toes),
- avoidance of chemical agents or plasters to remove callus or corns,
- use of emollients to lubricate dry skin
- cutting toenails straight across
|
|
|
|
|
|
Therapeutic Shoes: how to select, importance of wearing them
|
|
(**)
|
|
|
|
Monitoring of foot skin temperature at home
|
|
|
|
|
|
Consideration of prophylactic surgery if deformity is not properly accommodated by shoes;
|
|
|
|
|
|
Consideration of surgical offloading if DFU recurs despite standard care
|
|
|
|
|
(*): IWGDF Risk Categories:
- No peripheral neuropathy (Category 0)
- Peripheral neuropathy (Category 1)
- Peripheral neuropathy with peripheral artery disease and/or foot deformity (Category 2)
- Peripheral neuropathy and history of foot ulcer or lower-extremity amputation (Category 3)
(**): For therapeutic shoes be covered by Medicare, diabetic patients need to have peripheral neuropathy and at least pre-ulcerative signs such as calluses
Increasing patient adherence
Atreja et al.[23] have used the mnemonic “SIMPLE” to help clinicians formulate regimens that patients can adhere to:
|
SIMPLE method to increase patient adherence through education
- Simplifying regimen characteristics: for example, trying to match the regime to the patient's lifestyle
- Imparting knowledge: for example, ensure that the information meets the needs of the patient
- Modifying patient beliefs: for example, think about cultural as well as individual beliefs
- Patient and family communication: for example, active listening, provide clear, direct messages
- Leaving the bias: for example, make sure you work to the patient's level of understanding, leave your biases behind
- Evaluating adherence: for example, work with the patients to find a way to see what works for them.
|
CODING, COVERAGE AND REIMBURSEMENT
According to the National Coverage Determination (NCD) 70.2.1, foot exams for people with diabetic sensory neuropathy with LOPS are reasonable and necessary to allow for early intervention in serious complications that typically afflict diabetics with the disease.[23] Routine foot care policies are covered by Local Coverage Determinations and Articles.[24][25][26]
Relevant Codes
Diagnosis and Treatment of Diabetic Sensory Neuropathy with Loss of Protective Sensation
- G0245 - Initial foot exam pt lops. Initial physician evaluation and management of a diabetic patient with diabetic sensory neuropathy resulting in a loss of protective sensation (lops) which must include: (1) the diagnosis of lops, (2) a patient history, (3) a physical examination that consists of at least the following elements: (a) visual inspection of the forefoot, hindfoot and toe web spaces, (b) evaluation of a protective sensation, (c) evaluation of foot structure and biomechanics, (d) evaluation of vascular status and skin integrity, and (e) evaluation and recommendation of footwear and (4) patient education
- G0246 - Followup eval of foot pt lop. Follow-up physician evaluation and management of a diabetic patient with diabetic sensory neuropathy resulting in a loss of protective sensation (lops) to include at least the following: (1) a patient history, (2) a physical examination that includes: (a) visual inspection of the forefoot, hindfoot and toe web spaces, (b) evaluation of protective sensation, (c) evaluation of foot structure and biomechanics, (d) evaluation of vascular status and skin integrity, and (e) evaluation and recommendation of footwear, and (3) patient education
- G0247 - Routine footcare pt w lops. Routine foot care by a physician of a diabetic patient with diabetic sensory neuropathy resulting in a loss of protective sensation (lops) to include, the local care of superficial wounds (i.e. superficial to muscle and fascia) and at least the following if present: (1) local care of superficial wounds, (2) debridement of corns and calluses, and (3) trimming and debridement of nails
Routine Foot Care
- 11055 Trim skin lesion
- 11056 Trim skin lesions 2 to 4
- 11057 Trim skin lesions over 4
- 11719 Trim nail(s) any number
- 11720 Debride nail 1-5
- 11721 Debride nail 6 or more
- G0127 Trim nail(s)
Clarifications
- CMS’s National Correct Coding Initiative (CCI) edits consider G0245 to be a part of an E/M code. For this reason, reimbursement for both G0245 and an office or outpatient E/M code (99201-99215) for the same date of service cannot be claimed together, as those codes are bundled.
- For carriers, each physician or physician group of which that physician is a member may receive reimbursement only once for G0245 for each beneficiary. However, should that beneficiary need to see a new physician, that new physician may also be reimbursed once for G0245 for that beneficiary as long as it has been at least 6 months from the last time G0245 or G0246 was paid for the beneficiary, regardless of who provided the service. [27]
- In order for CWF to process and edit LOPS claims correctly, G0247 must be billed on the same claim with the same date of service as either G 0245 or G0246 in order to be considered for payment.[27]
- Once a beneficiary’s condition has progressed to the point where routine foot care becomes a covered service, payment will no longer be made for LOPS evaluation and management services. Those services would be considered to be included in the regular exams and treatments afforded to the beneficiary on a routine basis The physician or provider must then just bill the routine foot care codes along with the appropriate modifier. The CWF will edit to reject LOPS codes G0245, G0246, and/or G0247 when on the beneficiary’s record it shows that one of the following routine foot care codes were billed and paid within the prior 6 months: 11055, 11056, 11057, 11719, 11720, and/or 11721.[27]
- Covered routine foot care services are considered medically necessary once (1) in 60 days.[24]
APPENDIX
Summary of Evidence
SOE - Offloading to prevent DFU(back to text -therapeutic shoes) (back to text - surgical offloading)
- A 2016 IWGDF systematic review [28] included 2 systematic reviews and meta-analyses, 32 RCTs, 15 other controlled studies, and another 127 noncontrolled studies. Authors found that:
- As for prevention of DFU recurrence, at least 1 RCT at high risk of bias [29] demonstrated the efficacy of prescription custom-made therapeutic footwear (versus non-prescription) in relieving plantar pressure when footwear is worn by the patient
- Due to the limited number of controlled studies, clear evidence on the efficacy of surgical offloading and felted foam is not yet available. Interestingly, surgical offloading seems more effective in preventing than in healing ulcers. A number of controlled and uncontrolled studies show that plantar pressure can be reduced by several conservative and surgical approaches.
- The 2016 International Working Group on the Diabetic Foot (IWGDF) [17], the 2016 Society for Vascular Surgery in association with American Podiatric Medical Association (SVS) [4], the 2016 Wound Healing Society (WHS) [1], the 2012 Wound, Ostomy, and Continence Nurses Society (WOCN) [30] guidelines recommend offloading to prevent DFU
Intervention | IWGDF | SVS | WHS | WOCN | Properly fitting footwear to prevent a first foot ulcer,either plantar or non-plantar, or a recurrent non-plantar foot ulcer. If foot deformity or pre-ulcerative lesion, present, consider prescribing therapeutic shoes, custom-made insoles or toe orthosis
| 1CGrade 1C |
|
|
| Offloading with therapeutic footwear with demonstrated pressure relief that is worn by the patient to prevent plantar DFU | 1BGrade 1B | 1CGrade 1C | Level I | n/a | Surgical Achilles tendon lengthening, single or pan metatarsal head resection, or joint arthroplasty to prevent first time or recurrent DFUs | 2CGrade 2C | n/a | n/a | n/a | Digital flexor tenotomy to prevent distal toe DFU | 2CGrade 2C | n/a | n/a | n/a |
|
SOE - Patient Education (back to text) Systematic reviews - A 2016 systematic review and meta-analysis [21] analyzed 2 RCTs and 3 non-controlled studies that evaluated the effect of patient education (one 60 minute session) in addition to standard care on DFU incidence among diabetic patients at risk of developing DFU. The 2 RCTs did not find any statistically significant difference between the control and intervention groups. One RCT was considered at high risk [31] and the other one at low risk of bias. [32]
- A 2014 Cochrane systematic review [22] that included 12 RCTs evaluated the effect of 1 hour of patient education on incidence of first ulcer or DFU recurrence and other outcomes, concluded that In some trials, foot care knowledge and self reported patient behaviour seem to be positively influenced by education in the short term. Yet, based on the only two sufficiently powered studies reporting the effect of patient education on primary end points, that there is insufficient robust evidence that limited patient education alone is effective in achieving clinically relevant reductions in ulcer and amputation incidence.
|
MAJOR REVISIONS UPDATES
| Date | Comment |
| 10/17/20 | Added section "Coding, Coverage and Reimbursement" |