Audible handheld Doppler ultrasound and waveforms have been gaining acceptance as a tool for non-invasive arterial assessment of lower limbs. It has been shown to be a reliable and inexpensive test that can be carried out at the bedside to exclude significant peripheral artery disease (PAD) in individuals with or without diabetes, with sensitivity of 42.8% and specificity of 97.5%.[1] Recently, the British Lymphedema Society issued a position statement on the use of ankle brachial pressure index (ABPI) and handheld audible Doppler and waveform for patients with lower limb lymphedema. The statement supports the consensus across specialists that routine ABPI is not required for lymphedema patients, due to the frequent barriers to ABPI completion (e.g., pain, tissue thickening, cellulitis) Instead, the Society recommends clinical vascular assessment along side the use of audible handheld Doppler ultrasound and waveforms to rule out PAD prior to compression.[2] Despite its increasing acceptance, audible handheld Doppler ultrasound and waveform are operator dependent, and experience interpreting sounds and waveform is needed.
Background
In general, use of audible handheld Doppler ultrasound and/or continuous waveform analysis [1] is preferable over ABPI in the following cases [3]:
- Clinician is able to interpret audible Doppler signals or waveforms AND
-
Patient has diabetes, age > 70 years old (populations with tendency for non-compressible vessels due to calcification) [4][5][6], or
- ABI greater than 1.3 (may be elevated due to non-compressible vessels), or
- Active ulcer is present over the area of blood pressure cuff occlusion, or
- Severe local pain limits the ability to perform the ABI test, or
- Patient has lower limb lymphedema [2]
For patients for whom compression therapy is under consideration, see algorithm based on 'audible handheld Doppler ultrasound and/or continuous waveform analysis' in topic "How to Select Adequate Compression Therapy Pressure Levels and Products"
AUDIBLE HANDHELD DOPPLER ULTRASOUND AND WAVEFORMS
Selecting an audible handheld Doppler ultrasound (AHDU) device
Items to take in consideration when selecting a device include:
- Primary purpose of the device: ideally, it should be vascular assessment, specifically for detection of PAD. These devices will have probes that can be used for specific situations, such as:
-
- 4MHz vascular probe for deep vessels
- 5MHz vascular probe for edematous limbs and deep vessels
- 8MHz vascular probe for peripheral vessels and calcified arteries. Some probes have additional technology that allows for easy location of vessels
- 10MHz vascular probe for smaller vessels
- Portability: Most are portable and can be used at the bedside
- Ability to connect to recorder software and printer for waveform recording: waveform recording is required for insurance reimbursement.
See examples of different brands in topic "Vascular - Doppler"
Conducting the test
- In general, an 8 MHZ probe can be used
- Have patient rest for at least 5 min in supine resting position
- Apply ultrasound gel generously over the area to be assessed [over dorsalis pedis (DP) and/or posterior tibial (PT) arteries] (Figure 1)
- Float the probe in the gel and look for audible pulses
- Assess the DP and/or the PT arteries
- Ensure waveforms are generated and printed for test to be billable and reimbursable.
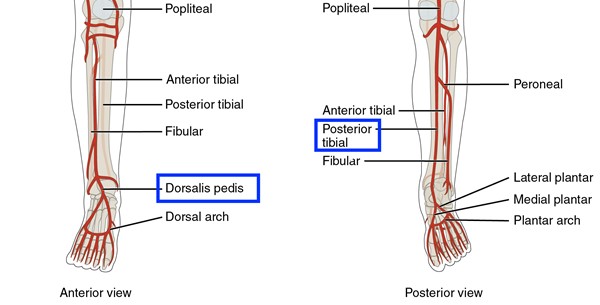
Figure 1. Dorsalis pedis and posterior tibial arteries
Interpreting the test
Waveforms
Doppler instruments used in combination with a recording device provide a graphic representation of blood flow through arterial vessels, which is traditionally characterized as triphasic, biphasic and monophasic (Figure 2).[7]
-
Triphasic waveform: Normal flow. Comprised of three phases: systolic forward flow, early diastolic flow reversal, and late diastolic forward flow [7]
-
Biphasic waveform: Indicates stenosis, in which the artery looses its diastolic components. Comprised of two phases: can be high resistive (systolic forward flow with diastolic flow reversal) or low resistive (sharp systolic acceleration/deceleration with pandiastolic forward flow) but both are considered biphasic.[7] Biphasic waveform may be normal in older individuals or when there is no clear transition from triphasic signal along the vascular tree.
-
Monophasic waveform: Denotes severe stenosis. Consists of one phase: systolic forward flow and no flow reversal, suggesting significant obstruction proximally.[7] Referral to a vascular specialist for formal duplex segmental exam is recommended for patients with monophasic waveform.
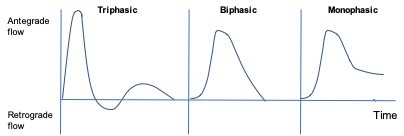
Figure 2. Peripheral artery waveforms: triphasic, biphasic and monophasic
Pulses
It is important to understand the difference between biphasic and monophasic pulses (Videos 1 and 2). Interpreting pulses within the patient's clinical context is highly recommended, as patients with heart conditions (e.g. atrial bigeminy) may have severe PAD and monophasic pulses that mimic biphasic pulses. A normal, triphasic pulse is demonstrated in Video 3.
BIPHASIC PULSE
Video 1. Biphasic pulse (some degree of stenosis, but may be normal)
MONOPHASIC PULSE
Video 2. Monophasic pulse (severe arterial stenosis)
TRIPHASIC PULSE
Video 3. Triphasic pulse (normal)
REVISION UPDATES
| Date |
Description |
| 4/28/19 |
Updated title, added Video (triphasic pulse) and figure (peripheral arteries) |