Last updated on 10/5/23 | First published on 9/21/20 | Literature review current through Jun. 2026
[cite]
Authors:
Elaine Horibe Song MD, PhD, MBA,
Kathryn Whiston-Lemm ACNP, CWON-AP,
Cathy Milne APRN, MSN, CWOCN-AP,
Scott A. Robinson MD,
more...
Coauthor(s)
Elaine Horibe Song, MD, PhD, MBACo-Founder and Editor, Wound Reference, Inc;
Professor (Affiliate), Division of Plastic Surgery, Federal University of Sao Paulo;
Volunteer, Association for the Advancement of Wound Care;
Google Scholar Profile
Disclosures: Nothing to disclose
Kathryn Whiston-Lemm, ACNP, CWON-AP
Disclosures: Nothing to disclose
Scott A. Robinson, MD
Disclosures: Nothing to disclose
Cathy Milne, APRN, MSN, CWOCN-AP
Disclosures: Nothing to disclose
Editors
For full access to this topic and more
premium content, upgrade today. Or get started with a Free Basic account (limited content and tools).
SURGICAL MANAGEMENT
Overview
This topic covers surgical management of arterial ulcers (AUs) with focus on surgical indications and selection criteria. For surgical treatment of patients with DFU associated with ischemia, see topic " Diabetic Foot Ulcer Associated with Ischemia - Management". For an introduction and framework for assessment of arterial ulcers, including epidemiology, risk factors, etiology, pathophysiology, history, physical examination, diagnosis, differential diagnoses, documentation and ICD-10 coding, see topic "Arterial Ulcers - Introduction and Assessment". For clinical guidelines and quality measures, see topic "Arterial Ulcers - Overview". For clinical management of arterial ulcers see "Arterial Ulcer - Treatment". For a patient education handout, see topic " Patient Education - Arterial Ulcer.
Background
AUs are leg ulcers that develop due to inadequate blood supply to the skin (arterial insufficiency). Most often, the decrease in blood supply is caused by underlying peripheral arterial disease (PAD) that results from narrowing of the arteries to the legs (atherosclerosis) and leads to chronic limb-threatening ischemia (CLTI), an advanced manifestation of PAD.[1] However, arterial insufficiency may also be caused by other non-atherosclerotic diseases.
AUs are best managed by a multidisciplinary team. A customized treatment plan is created with the patient's input, based on a comprehensive assessment. For details, see topics "Arterial Ulcers - Introduction and Assessment" and " Arterial Ulcer - Treatment". Patients with healable AUs should undergo either prompt revascularization or a 4-week trial of conservative treatment followed by revascularization if needed, depending on the Society for Vascular Surgery Lower Extremity Threatened Limb Wound/Ischemia/Foot Infection (WIfI) classification.[2]
The vascular specialist's decision on whether to offer revascularization is based on patient factors (i.e., perioperative risk and life expectancy) and limb condition (i.e., limb severity and anatomy). See topic " Arterial Ulcer - Treatment".
REVASCULARIZATION
Effective revascularization is the cornerstone of limb salvage in chronic limb-threatening ischemia CLTI. Multiple techniques are available and the vascular surgeon will choose the most appropriate modality after assessing the patient. [2]
Indications
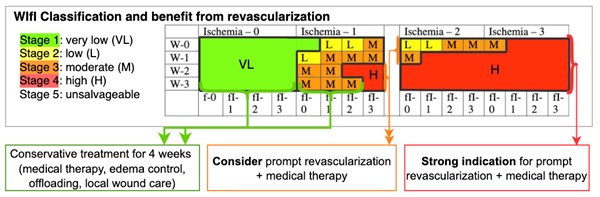
Fig. 1. Interventions and estimated benefit from revascularization for each WIfI stage
For the following patients with healable AUs, clinical guidelines suggest revascularization if the ulcer does not decrease in size by 50% in 4 weeks despite appropriate infection control, wound care, and offloading [2][3]
- Patients with low-risk limbs (e.g. WIfI stage 1) without significant ischemia (WIfI ischemia grade 0), but with an isolated region of poor perfusion in conjunction with major tissue loss (eg, WIfI wound grade 2 or 3)
- 2CPatients with low-risk limbs (e.g. WIfI stage 1) with moderate ischemia (e.g, WIfI ischemia grade 1) (Grade 2C)
- 2CPatients with intermediate limb threat (e.g, WIfI stages 2 and 3) with moderate ischemia (e.g, WIfI ischemia grade 1) (Grade 2C)
For the following patients with healable AUs, clinical guidelines recommend prompt revascularization, combined with medical therapy [2]:
- 2CPatients with intermediate limb threat (eg, WIfI stages 2 and 3) and significant ischemia (eg, WIfI ischemia grades 2 and 3) (Grade 2C)
- 2CPatients with advanced limb threat (eg, WIfI stage 4) and moderate ischemia (eg, WIfI ischemia grade 1).(Grade 2C)
- 1CPatients with advanced limb-threatening conditions (eg, WIfI stage 4) and significant perfusion deficits (eg, WIfI ischemia grades 2 and 3) (Grade 1C)
For patients with mild-to-moderate ischemia and tissue loss, a conservative approach has been shown to achieve complete wound healing in 76.8% of limbs in 4.4 ± 4.1 months; and limb salvage at long-term follow-up of 89.3%, with limited need for deferred revascularization (14%).[4][5][6]
Contraindications
- For patients with DFU and PAD for whom, from the patient perspective, the risk-benefit ratio for the probability of success is unfavorable, the clinical guidelines recommend clinicians avoid revascularization.[3][7] Some examples are patients who:
- Are severely frail
- Have a short life expectancy
- Have poor functional status or are bed bound
- Have a large volume of tissue necrosis that renders the foot functionally unsalvageable
- For patients with DFU and PAD for whom, from the patient perspective, the risk-benefit ratio for the probability of success is unclear, revascularization may not be appropriate. In clinical decision-making, it should be taken into account that even severely ischemic ulcers can heal without a revascularization; as noted, two observational studies reported healing rates of about 50% (with or without minor amputations). [3][7][8][9]
- Patients who are not good candidates for revascularization may be treated with an approach for non-healable ulcers (i.e. palliative wound care, medical therapy, mechanical offloading).[10] Non-revascularization treatments of the limb may be considered. See section 'Non-revascularization Treatment of the Limb' in topic "Arterial Ulcers - Treatment".
- If amputation is under consideration, transcutaneous oximetry is recommended to determine amputation level.[11] See topic "Transcutaneous Oximetry".
Techniques
Revascularization techniques can be roughly classified as endovascular and open surgical bypass. Endovascular procedures are preferred over open surgical approach in most cases.
-
Endovascular approach: utilizes less invasive procedures such as angioplasty, which uses a balloon to open the blockages in the arteries, or laser atherectomy, which uses high energy light to vaporize the blockage inside the arteries. Either procedure may be performed with or without placing a stent inside the artery to help keep the artery patent. Endovascular procedures are performed by “interventionists” (cardiologists, radiologists, vascular surgeons who utilize endovascular technologies).[12]
- Open surgical approach: vascular bypass surgery, in which a prosthesis or segments of a healthy vein are used to bypass the affected arterial segments, allowing blood to bypass the arterial obstruction and reach distal areas. Performed by vascular surgeons.
The choice of revascularization approach should be based on patient risk, anatomic pattern of disease, and other clinical factors. Anatomic complexity is often classified according to the Global Limb Anatomic Staging (GLASS) system. The GLASS system is a new, clinically oriented framework for classifying the pattern of arterial disease in CLTI.[2] Guidelines recommend that vascular surgeons decide on the approach (e.g., open bypass, endovascular, no revascularization) based on the GLASS system and WIfI staging.[2]
Below are the recommendations by the Society for Vascular Surgery, European Society for Vascular Surgery, and World Federation of Vascular Societies [2]:
- 1BFor CLTI patients with moderate to severe (eg, GLASS stage IA) aortoiliac disease, endovascular first approach is recommended, depending on the history of prior intervention.(Grade 1B)
- 2CFor average-risk CLTI patients with extensive (eg, GLASS stage II) aortoiliac disease or after failed endovascular intervention, open surgical reconstruction is suggested. (Grade 2C)
- 1CFor CLTI patients with hemodynamically significant ( > 50% stenosis) disease of the common and deep femoral arteries, common femoral artery endarterectomy with patch angioplasty, with or without extension into the PFA, is recommended. (Grade 1C)
- 2CFor aortoiliac disease with concomitant common femoral artery involvement (eg, GLASS stage IB inflow disease), surgeons might opt for a hybrid procedure combining open common femoral artery endarterectomy and endovascular treatment. (Grade 2C)
- 2CFor selected patients who are deemed to be at high surgical risk or to have a hostile groin, surgeons might opt for endovascular treatment of significant common femoral artery disease. (Grade 2C)
- 2CFor patients with significant wounds (eg, WIfI wound grades 3 and 4), particularly those involving the midfoot or hindfoot, and when the appropriate target arterial path is available, surgeons might consider angiosome-guided revascularization. (Grade 2C)
Postoperative care
Systemic therapy
- 1AFor all patients who have undergone lower extremity revascularization, clinical guidelines recommend initiating or maintaining best medical therapy for PAD, including long term use of antiplatelets (aspirin plus clopidogrel), statin therapy, and smoking cessation.(Grade 1A)
Local post operative care
Surgical site
- Patients should be frequently monitored and any abnormality should be immediately communicated to the vascular surgeon.
-
- Distal pulses: presence of distal pulses signals effectiveness of the revascularization procedure.
- Surgical sites: signs of infection or hematoma require immediate attention.
Wound management
- For patients with AU, the main goal after revascularization is to promote wound healing through adequate local wound care, offloading and compression (if no contraindications).
-
- Pressure offloading is one of the single most important, but frequently neglected aspects of therapy. See topic "Offloading Devices" and "How to Select Offloading Devices"
- For selected full-thickness AUs, wound coverage with skin grafts or cellular and/or tissue based products, or negative pressure wound therapy may be required.
- After the wound is healed, the goal is to maximize ulcer-free days.
LOWER LIMB AMPUTATION
For patients with CTLI, goals of surgical interventions include the preservation of the ability to walk in carefully selected patients, and/or resolution of ischemic pain, ulceration and infection.
- For patients who are revascularization candidates, vascular reconstruction is the most direct method for achieving functional limb salvage.
-
- Many patients (especially those with diabetes) undergoing revascularization still require removal of distal necrotic or infected tissue through debridement/amputation in order to achieve a completely healed and functional extremity.
- For patients who are not revascularization candidates, limb amputation can often allow an opportunity for patients to ambulate independently or to have resolution of ischemic pain, ulceration and infection. Patients undergoing a toe or foot amputation can ambulate in as little as 2 - 4 weeks after surgery, provided they have adequate blood flow to the extremity. [13]
- Multiple debridements and reamputations are required in 4% to 40% of patients, depending on the level of amputation.[2]
Types of amputation
Lower limb amputations due to CLTI can be roughly categorized as:
- Minor or major
- Primary or secondary
Minor amputation
- Definition: Minor amputations of the foot include digital and ray amputation of the toe, transmetatarsal amputation of the forefoot, and Lisfranc and Chopart amputations of the midfoot.
- Indication: For patients with distal necrosis (e.g. toe tip, toe), minor amputation can be considered if distal perfusion and offloading after amputation are expected to be adequate, with the goal of preserving foot function.
-
-
Toe amputation: indications include toe tip ulcers with exposed bone/ osteomyelitis or hammertoe deformities that are dislocated and no longer functional. Toe amputations may be performed in the office setting, under local anesthesia.[13]
-
Transmetatarsal amputation: indicated for correction of forefoot ischemia and infection.[13]
-
Chopart amputation: indicated for severe forefoot ischemia and infection, or as a revision of the transmetatarsal amputation stump when the skin breaks down. This procedure is less desirable than a transmetatarsal amputation from a functional recovery (ambulation) standpoint.[13]
Major amputation
- Definition: Major amputations of the lower limb are amputations that are proximal to the midfoot.
- Indication: Major amputation may be considered in situations in which an aggressive attempt at limb salvage is unlikely to succeed, poses excessive physiologic stress on the patient, or is of limited value because of other causes of limb dysfunction. The goal in these cases is to preserve the walking ability in selected patients or resolution of ischemic pain, ulceration and infection.
Primary amputation
- Definition: lower extremity amputation without an antecedent open or endovascular attempt at limb salvage.
- The 5 major indications for primary amputation are:
-
- Patients with arterial disease that cannot be reconstructed because of lack of patent vessels distal to the arterial obstruction, as confirmed by imaging studies.
- Patients whose major weight-bearing portions of the foot have been destructed, rendering it incompatible with ambulation. Weight-bearing areas consist of the calcaneus, the first and fifth metatarsal heads, and a functional arch.
- Non-functional lower extremity due to paralysis or persistent flexion contractures.
- Severe comorbid conditions or limited life expectancy due to terminal illness. Goal for these patients is to relieve ischemic pain and improve quality of life.
- The need for multiple surgical procedures in order to restore a viable lower extremity. If multiple procedures with high morbidity are required, primary amputation should be strongly considered to permit early ambulation.
-
- For all patients considered for primary amputation, also consider revascularization to improve inflow in an attempt to reduce the level of amputation.
Secondary amputation
-
Definition: lower extremity amputation after a failed attempt at limb salvage with an open or endovascular approach.[2]
- Indication: major amputation with a goal of rehabilitation to independent ambulation should be considered for patients with unsuccessful revascularization and low probability of a successful redo.
Pre-operative assessment
- Indication for an nonurgent amputation should be done by a multidisciplinary team, based on a full functional and vascular assessment, and discussion with the patient.
- Selection of the initial level of amputation is a critical step for a successful amputation procedure and postoperative rehabilitation.
-
- Determination of the level of amputation should be made based upon clinical assessment (by the surgeon, a rehabilitation and occupational physiotherapist, and a prosthetic specialist) and assessment of tissue perfusion.
-
- For assessment of tissue perfusion, the use of TcPO2 has been extensively evaluated. Data show that wound complications increase as TcPO2 levels fall below 40 mm Hg.
- A named discharge coordinator should ensure that there is a defined post amputation care pathway.
Postoperative care
-
1CFor all patients undergoing amputation, clinical guidelines recommend involvement of a multidisciplinary rehabilitation team from the time a decision to amputate has been made until successful completion of rehabilitation has been achieved.(Grade 1C) [2][12][13][14]
-
- Rationale: The stump evolves with time, and the prosthetic requirements continue to change. An ill-fitted prosthesis will cause stump ulcerations
- CLTI patients who have undergone amputation should follow up at least yearly with the vascular specialist, to monitor progression of disease in the contralateral limb and to maintain optimal medical therapy and risk factor management.
Official reprint from WoundReference® woundreference.com ©2026 Wound Reference, Inc. All Rights Reserved
NOTE: This is a controlled document. This document is not a substitute for proper training, experience, and exercising of professional judgment. While every effort has been made to ensure the accuracy of the contents, neither the authors nor the Wound Reference, Inc. give any guarantee as to the accuracy of the information contained in them nor accept any liability, with respect to loss, damage, injury or expense arising from any such errors or omissions in the contents of the work.