SUMMARY
The Undersea and Hyperbaric Medical Society has approved indications for treatment that will be listed below. These may be classified as emergent, urgent or elective. Providers must consider the beneficial effects of HBOT and weigh them against the risks of therapy for each patient. It is imperative that the patient receives a thorough history and physical, and has the risks and benefits explained, and understands expectations of this type of therapy. Clinicians have the added obligation of familiarizing themselves with the Coding and Reimbursement guidelines for HBOT to ensure compliance with the Centers for Medicare and Medicaid Services.
CLINICAL
Overview
Hyperbaric oxygen therapy (HBOT) is a medical treatment in which the entire body is exposed to increased atmospheric pressure, (greater than 1.4 ATA). HBOT consists of breathing 100% oxygen (O2 ) in a hyperbaric chamber at pressures two to three times greater than atmospheric pressure (defined as 1 atmosphere absolute, ATA, at sea level).[1] HBOT treatments are usually administered daily for 90 to 120 min, over 20 to 40 consecutive sessions and HBOT may be utilized as either a primary or adjunctive therapy. The conditions currently approved for treatment with HBOT by the Undersea and Hyperbaric Medicine Society are listed in the section 'Indications' below.
This following is an introduction to hyperbaric oxygen therapy. For more detailed information and actionable tools, please refer to specific topics within the Hyperbaric Oxygen Therapy Knowledge Base.
Background
History of HBOT
Hyperbaric Oxygen Therapy (HBOT) is not a novel concept, with its origins tracing back to the 17th century. [2][3] The first recorded concept of compressed air for therapeutic purposes was by British physician Henshaw in 1662, who designed a chamber called a "Domicilium". [2][3] It has been suggested however, that Henshaw's legacy might be limited to idealizing the concept of hyperbaric medicine rather than being its first practitioner.[4] Despite this early experimentation, the toxic effects of oxygen reported in 1789 led to a reluctance to adopt HBOT widely.[2][3]
The 20th century saw a resurgence in interest and development in HBOT. In 1928, a significant milestone was achieved by Kansas City physician Cunningham, who constructed a large hyperbaric chamber capable of accommodating up to 40 patients at a time. This structure, known as Cunningham’s steel ball hospital, marked a significant advancement in the practical application of HBOT.[3]
The modern era of hyperbaric medicine began with Ite Boerema, often recognized as the father of contemporary hyperbaric medicine. In 1956, Boerema published the first clinical paper on HBOT at the University of Amsterdam, detailing its use during cardiac surgery to prolong safe operating times. He later reported on the therapy's beneficial effects in treating necrotizing infections and ischemic leg ulcers.[3]
The application of HBOT in chronic wound care was first reported by Kulonen in 1968. As research has elucidated the oxygen-dependent cellular processes involved in tissue repair, such as collagen production by fibroblasts and the microbicidal activity of macrophages, the use of HBOT in treating chronic wounds has become more prevalent. This growing body of evidence led the Centers for Medicare & Medicaid Services to begin reimbursing HBOT for the treatment of diabetic foot ulcers (DFU) in 2002.[3]
HBOT today
HBOT has continued to evolve, with ongoing updates and revisions to treatment protocols and clinical recommendations. The therapy is now a well-established treatment modality for various medical conditions, supported by a framework of clinical evidence and regulatory guidelines.
Overall, today HBOT is considered a safe, non-invasive therapy with very few adverse effects. The absolute contraindication to HBOT is an untreated pneumothorax because, this condition can progress with changes in environmental pressure and has the potential to develop into a tension pneumothorax.[5]
The hyperbaric medicine facility is equipped to treat a broad cross section of patient states. A majority of treatments are expected to be provided to electively referred outpatients. Treatments are provided using the monoplace or multiplace hyperbaric delivery system.
A physician with training and institutional credentials in hyperbaric medicine will provide consultation and manage cases. Additionally, a staff member trained in the operation of the hyperbaric chamber and related equipment will conduct the hyperbaric procedure. The Hyperbaric Medicine Services collaborate with the institutional physicians, nurses, and other services to fully integrate hyperbaric oxygen therapy into the overall medical care of each patient. See topic "Hyperbaric Program Staffing Guidelines".
Patients are accepted for hyperbaric oxygen therapy upon referral following a formal hyperbaric consultation. Unless directed otherwise, patients will usually remain under the general medical care of their primary physician team.
How the intervention works
Central to the mechanism of HBOT are gas laws describing the relationship between the volume, pressure, and temperature of gases during therapy.[5]
The air we breathe has approximately 21% oxygen at 14.7 pounds of pressure per square inch (psi) when measured at sea level. In the hyperbaric chamber, the atmospheric pressure can be increased to as much as 3 times normal (about 44.1 psi), with the patient breathing 100% oxygen. This increases the amount of oxygen in the blood plasma to approximately 3 times its normal levels at 1 atmosphere pressure. As a results, higher oxygen levels are delivered to end organ tissues throughout the body. This can result in many beneficial effects in a variety of disease processes that will be discussed in the paragraphs below.[6]
For details, see topic "Gas Laws And The Therapeutic Effects of HBOT".
Figure 1 shows an overview of the multiple primary and secondary effects of HBOT.[5][7]
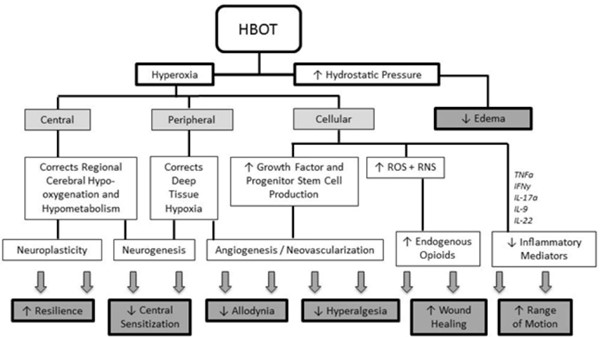
Fig. 1. Overview of the multiple primary and secondary effects of HBOT. HBOT: Hyperbaric Oxygen Therapy; ROS: reactive oxygen species; RNS: reactive nitrogen species; TNFα: tumor necrosis factor—alpha; IFNγ: interferon-gamma; IL: interleukin.
Indications
An Emergent indication would be defined as any medical condition in which hyperbaric oxygen therapy is the primary standard of care. The following are considered to be emergent conditions for the use of HBOT:
Medicare Covers the above indications
An Urgent condition is a medical condition in which hyperbaric oxygen therapy is an adjunctive modality. The following are considered to be urgent conditions for the use of HBOT:
Medicare Covers the above indications with the exception of Central Retinal Artery Occlusion, Idiopathic Sudden Sensorineural Hearing Loss, and Severe Anemia
An Elective condition is a medical condition in which HBOT is utilized in a supportive care modality. The following are considered to be elective indications for the use of HBOT:
Medicare Covers the above indications
In addition to indications covered by Medicare and approved by the UHMS, HBOT has shown benefits as adjunctive therapy for selected complex conditions (e.g. neurological and chronic pain) conditions because of its multiple primary and secondary beneficial effects.[5] See topic "Investigational HBOT Indications".
Emergent Indications
Acute Carbon Monoxide Poisoning
The toxicity of carbon monoxide is based on a number of pathophysiological mechanisms. Carbon monoxide can cause hypoxic stress to tissues (e.g., heart or brain) leading to injury. A second mechanism of injury is thought to be through an inflammatory response to the toxic chemical. This inflammation primarily attacks brain tissue. The blood level of carbon monoxide has not correlated well with resultant neurological injuries. Administration of supplemental oxygen has long been the cornerstone of therapy for patients suffering carbon monoxide poisoning. Oxygen inhalation hastens the dissociation of CO from the hemoglobin molecule, as well as providing enhanced tissue oxygenation. Hyperbaric oxygen causes this dissociation to occur at a much greater rate than that achievable by breathing pure oxygen at ambient atmospheric pressure. In addition, HBOT has shown to be anti-inflammatory and reduces tissue injury.
Air or gas embolism
Gas embolism occurs when gas bubbles (regardless of source) enter arteries or veins. Arterial gas embolism (AGE) was classically described during submarine escape training, caused by pulmonary barotraumas during free ascent after breathing compressed gas at depth. AGE commonly occurs when a pulmonary bleb ruptures during normal SCUBA ascent, asthma with air trapping, a concussive blast injury (in or out of the water), mechanical ventilation, penetrating chest trauma, chest tube placement, or bronchoscopy. Venous gas embolism (VGE) is more rare and can occur after compressed gas diving. A large amount of venous bubbles overcome the pulmonary arterial capillary network and are passed to the left side of the heart. There are numerous causes for gas embolism outside of diving, some of which are iatrogenic accidents during invasive procedures. Hyperbaric oxygen remains the definitive treatment for gas embolism. Indications for treatment include neurological or cardiac manifestations of gas embolism in any procedure at risk. Gas bubbles can persist for many days, so a trial of hyperbaric oxygen treatments should be started on any patient with symptoms, even days after the event. Recompression and hyperbaric oxygen administration has 3 main effects: 1) decreasing bubble size, 2) oxygenation of compromised tissues, and 3) an anti-inflammatory effect.
Decompression illness
Decompression illness (DCI) arises from the generation of bubbles of inert gas in tissue and/or blood in volumes sufficient to interfere with organ function. This state can be caused by rapid decompression during ascent from diving, flying after diving, or a hyperbaric/ hypobaric chamber exposure. Bubble formation occurs when the rate of decompression exceeds the rate at which diffusion and perfusion reduce the tissue inert gas partial pressure. There are a variety of clinical expressions of DCI, the most serious of which causes neurologic deficits as evidenced on the physical examination. The diagnosis of DCI is a diagnosis of exclusion and depends greatly upon the history and physical examination of the diver.
A wide variety of hyperbaric regimens have been described in the medical literature. These vary in treatment pressure, time at pressure, partial pressure of oxygen, and use of other mixed gases. There have been no broad scientific studies in a prospective, randomized controlled fashion. However, the following points are generally accepted: 1) Complete resolution occurs when patients are treated early in the disease process, and 2) the US Navy oxygen treatment tables (TT6) with initial recompression to 60 fsw have been the most widely used treatments and have a high degree of success. Recompression and hyperbaric oxygen administration has 3 main effects: 1) decreasing bubble size, 2) oxygenation of compromised tissues, and 3) an anti-inflammatory effect.
Urgent Indications
Acute peripheral arterial insufficiency
Acute peripheral arterial insufficiency covers a spectrum of diseases that includes acute traumatic and non-traumatic events sharing the common feature of sudden occlusion of the arterial blood supply. The resultant tissue hypoxia and ischemia leads to increased local concentrations of cellular byproducts, compromised microcirculation, advancing hypoxia, decreased nutrient delivery to the end tissues, vascular membrane breakdown, and edema formation. These factors threaten wound healing and contribute to advancing infectious processes.
Hyperbaric oxygen can be beneficial in managing acute peripheral arterial insufficiency by several mechanisms: 1) Increasing tissue oxygen concentrations, thus preventing cellular death, 2) stimulating fibroblasts and macrophages to secrete collagen and enhance neovascularization, 3) reducing edema formation by reducing capillary leakage and tissue swelling, thus increasing tissue perfusion, and 4) maintaining the bacterial killing ability of leukocytes after phagocytosis.
Acute traumatic ischemia (Trauma, Crush Injuries, Compartment Syndrome)
Acute traumatic ischemia occurs when there is a severe injury to a limb that results in compromise of the arterial blood supply or perfusion differential pressure to that limb. The immediate, emergent threat is determined by whether perfusion of the limb is sufficient to maintain viability of the tissues. Crush injuries are directly associated with trauma while skeletal muscle compartment syndromes arise from ischemia, venous outflow obstruction, exertion, external compression, or trauma. There are 3 common features: 1) ischemia and hypoxia at the injury site, 2) a gradient of injury, and 3) the potential for self-perpetuation of the injury.
While hyperbaric oxygen is a useful adjunct to healing, surgery and aggressive medical interventions will often be required in order to manage the condition. Conditions with related pathophysiology, which are also amenable to hyperbaric oxygen therapy, include threatened flaps, grafts, re-implantations, and frostbite.
The pathophysiology is a picture of vasogenic edema as a consequence of physical injury that is exacerbated by cytogenic edema because the injured tissues are no longer able to maintain intracellular water. When tissue oxygen tensions fall below 30 mmHg, the host responses to infection and ischemia are compromised. White blood cell phagocytic killing becomes ineffective, fibroblasts are no longer able to secrete collagen, and neovascularization cannot occur in hypoxic tissue.
Hyperbaric oxygen (at 2.4 atmospheres absolute) increases blood oxygen content and raises plasma and tissue oxygen tensions by several times over surface oxygen breathing. Hyperbaric oxygen also induces vasoconstriction (decreasing blood flow by 10-20%) in normal tissues, thus reducing edema in the injured tissues. In this indication, hyperbaric oxygen enhances oxygen concentration at the tissue level, increases oxygen delivery per unit of blood flow, and reduces edema.
CENTRAL RETINAL ARTERY OCCLUSION
Central Retinal artery occlusion (CRAO) is an emergent rare eye disorder that typically produces sudden, severe, painless, and irreversible vision loss in the affected eye. Patients at risk include those with giant-cell arteritis, atherosclerosis and thromboembolic disease. Once the arterial supply to the retina is occluded, variable degrees of tissue loss may occur within 90-120 minutes. This may be irreversible without immediate diagnosis and intervention. Early HBOT appears to have a beneficial effect on visual outcome in patients with CRAO.
A number of different treatment regimens have been used with variable degrees of success. Frequently, there has been no improvement in visual acuity once blood supply to the retina has been lost. There have been a number of different pathophysiologic etiologies described with a common denominator of interrupted arterial supply to the retinal tissue. Here have been several studies showing that addition of HBOT as soon as possible has resulted in increased visual acuity by 2 to 3 lines on a Snellen eye chart. This may make the difference between light perception only to finger counting or television vision.
There are several treatment options described in the medical literature. Hyperbaric oxygen can be delivered at 2.4 atmospheres absolute with 90 minutes of oxygen breathing during a 120 minute treatment. This will be repeated twice daily until maximum visual acuity is obtained. A second option for treatment involves treating at 2.4 atmospheres absolute for 30 minutes. If there is no improvement in visual acuity, the treatment pressure is increased to 2.8 atmospheres absolute, following a US Navy Treatment Table 6 protocol. Further treatments at 2.4 or 2.8 atmospheres absolute are administered on a twice daily regimen until visual acuity no longer improves. There is currently AHA Level IIb evidence suggesting that hyperbaric oxygen is helpful.
gas gangrene
Gas gangrene (Also known as clostridial myositis, myonecrosis, or spreading clostridial cellulitis with systemic toxicity) is an acute, rapidly progressive, non-pyogenic, invasive clostridial infection of the muscles, characterized by profound toxemia, extensive edema, massive death of tissue, and a variable degree of gas production. The infection is caused by anaerobic, spore-forming, Gram-positive, encapsulated bacilli. The most common organism in Clostridium Perfringens, however, there are more than 150 clostridial species which can cause the disease. While there are many toxins produced in this infection, the alpha toxin (Lecithinase and Phospholipase-C) cause most of the tissue destruction.
Hyperbaric oxygen therapy increases tissue oxygen levels to more than 250 mmHg, thus reaching levels that stop alpha-toxin activity. Hyperbaric oxygen has been shown to be bacteriocidal/bacteriostatic to the Clostridium organisms. Hyperbaric oxygen should not be used alone but is adjunctive to aggressive surgical and medical management. Early hyperbaric oxygen treatment is 1) lifesaving because less heroic surgery needs to be performed, and 2) it is limb- and tissue-saving because no major amputations are performed prematurely. Hyperbaric oxygen treatments clarify the demarcation between viable and dead tissue, thus the total amount of tissue lost is greatly reduced.
Compromised Grafts & Flaps
Hyperbaric oxygen therapy is not needed for routine, uncompromised skin grafts or flaps. However, in cases where there is decreased perfusion or frank hypoxia, hyperbaric oxygen can help maximize the viability of the compromised tissue thus reducing the need for re-grafting or repeat flap procedures. There are multiple clinical studies showing the benefit of hyperbaric oxygen for failed or failing flaps and skin grafts. Types of grafts and flaps studied include pedicle flaps, random flaps, irradiated wounds and flaps, composite grafts and axial pattern flaps. Although the types of flaps and grafts are different, the common denominator to flap necrosis is tissue hypoxia.
Hyperbaric oxygen can be beneficial in managing failing flaps and skin grafts by several mechanisms: 1) Increasing tissue oxygen concentrations, thus preventing cellular death, 2) stimulating fibroblasts and macrophages to secrete collagen and enhance neovascularization, 3) reducing edema formation by reducing capillary leakage and tissue swelling, thus increasing tissue perfusion, and 4) maintaining the bacterial killing ability of leukocytes after phagocytosis.
Necrotizing Soft Tissue Infections
Hyperbaric oxygen therapy is an accepted adjunct to surgical and antibiotic treatment for necrotizing soft tissue infections. Such conditions may result from a combination of anaerobic and aerobic bacteria. Necrotizing infections appear in a wide variety of clinical settings, including trauma, surgical wounding, and/or foreign bodies. The patient is frequently compromised with diabetes, vasculopathy, or other immune-affecting diseases. Infections frequently cause local hypoxia and an infection-induced occlusive endarteritis. This hypoxic condition profoundly impairs white blood cell bacterial killing actions. Clinical signs of mixed soft tissue infection include tissue necrosis, a putrid discharge, gas production (often visible on x-ray), and infection burrowing through soft tissue and fascial planes. This is often seen without the typical inflammatory response in severe infections.
Hyperbaric oxygen works by increasing local tissue oxygen levels, thus helping white cell-mediated bacterial killing and by stopping synergistic interaction present in mixed bacterial infections. Aggressive hyperbaric oxygen treatment is clearly recommended for necrotizing fasciitis, Fournier’s gangrene, crepitant anaerobic cellulitis, progressive bacterial gangrene, and non-clostridial myonecrosis (synergistic necrotizing cellulitis).
IDIOPATHIC SUDDEN SENSORINEURAL HEARING LOSS
Idiopathic Sudden Sensorineural Hearing Loss (ISSHL) is clinically defined as a hearing loss of at least 30 dB occurring within 3 days over at least 3 contiguous frequency ranges. The common presentation is unilateral hearing loss, tinnitus, a sensation of aural fullness, and dizziness or vertigo. The ear, nose, and throat surgeon will have ruled out mass lesions of the eighth cranial nerve. The specific etiologies of this syndrome remain unclear and multiple drug regimens have been used with moderate success.
Addition of hyperbaric oxygen therapy in addition to drug regimens has been shown to impart a 37.7 dB improvement in hearing in those with severe hearing loss and a 19.3 dB gain in those with a moderate hearing loss. Nine of 11 studies in the literature demonstrate positive results with the addition of HBOT to the treatment regimen. There is Class IIa evidence to support its use.
Patient selection criteria include patients with the collection of signs and symptoms above who present during the first two weeks after symptom onset. The patient should be evaluated carefully by an otolaryngologist and audiologist with appropriate imaging and hearing tests performed. In addition to appropriate medical management, hyperbaric oxygen should be administered.
INTRACRANIAL ABSCESS
An intracranial abscess involving the brain or its membranes. It is seldom primary but usually occurs secondary to infections of the middle ear, nasal sinuses, face, or skull or from contamination from penetrating wounds or skull fractures. It may also have a metastatic origin arising from septic foci in the lungs (bronchiectasis, empyema, lung abscess), in bone (osteomyelitis), or in the heart (endocarditis). Infection of nerve tissue by the invading organism results in necrosis and liquefaction of the tissue, with edema of surrounding tissues. Brain abscesses may be acute, subacute, or chronic. Their clinical manifestations depend on the part of the brain involved, the size of the abscess, the virulence of the infecting organism, and other factors.
The beneficial influence of HBO on increased intracranial pressure has been documented for more than 50 years. HBOT provides sufficient oxygen delivery to potentially hypoxic brain areas potentiating the effects of antibiotics. HBOT acts against specific anaerobic microorganisms as the predominant cause of intracranial abscess. [8]
SEVERE ANEMIA
Patients who have marked blood loss of red blood cell mass by hemorrhage, hemolysis, or aplasia run the risk of lacking adequate oxygen-carrying capacity by blood. The more quickly the patient develops the anemia, the less tolerant the body is of that insult. Patients may not be able to be transfused for a variety of reasons. Common reasons include refusal of transfusion on religious grounds or inability to crossmatch blood for transfusion.
Blood substitutes are still undergoing randomized clinical trials. No blood substitute is currently recommended for safe clinical use. Pulsed hyperbaric oxygen therapy provides a way to rectify accumulating oxygen debt in exceptional blood loss anemia when transfusion is not possible. Hyperbaric oxygen is considered adjunctive to pursuing adequate crossmatching, transfusion of red blood cells, and/or use of hematinic agents.
Elective Indications
DIABETIC FOOT
Patients with diabetes are at high risk for developing foot ulcers due to neuropathy and peripheral arterial occlusive disease. The pathophysiology of diabetic foot ulcers include progressive development of a sensory, motor, and autonomic neuropathy leading to loss of protective sensation, deformity causing increased plantar foot pressure, and alterations in autoregulation of dermal blood flow. Diabetes causes advanced peripheral vascular disease generally at the trifurcation level just below the knee.
Neuropathy, vascular disease, impaired white blood cell response to infection, and cellular dysfunction all contribute to the poor clinical outcomes of diabetic foot ulcers. Despite standard wound care, these foot ulcerations can progress and are associated with cellulitis, deep tissue necrosis, abscess formation, and the development of osteomyelitis. This type of ulcer is a Wagner grade III ulcer, an equivalent of the University of Texas IIB, IID, IIIB, or IIID ulcers. Progression to frank distal foot gangrene (Wagner grade IV) or gangrene involving the whole foot (Wagner grade V) can occur.
Hyperbaric oxygen therapy has been proven to be a beneficial adjunct to advanced wound care in diabetic foot ulcers meeting the following criteria: 1) the patient has type 1 or 2 diabetes and a lower extremity ulcer due to diabetes, 2) the ulcer is a Wagner grade III or higher, and 3) the patient has failed a 30-day standard wound therapy regimen that included assessment and attempts to correct vascular abnormalities, optimizing diabetes control, nutrition, debridement, moist wound dressing, off-loading, and treatment of underlying infection.
CHRONIC REFRACTORY OSTEOMYELITIS
Refractory osteomyelitis is a chronic osteomyelitis that persists or recurs after appropriate interventions have been performed, or where acute osteomyelitis does not respond to accepted management techniques. Hyperbaric oxygen, when combined with appropriate antibiotics, nutritional support, surgical debridement and reconstruction, provides a useful clinical adjunct in the management of refractory bone infections. Addition of hyperbaric oxygen to appropriate clinical management produces an infection arrest rate of nearly 80%.
Hyperbaric oxygen benefits healing by enhancing bacterial killing activity of white blood cells. Next, certain antibiotics require an oxygen-mediated pathway in order to transport the medication across bacterial walls. Third, there is evidence that osteogenesis and osteoclast remodeling is an oxygen-dependent activity. Finally, osteomyelitis is characterized by both acute and chronic forms of hypoxia. Hyperbaric oxygen raises tissue levels of oxygen, decreases edema, decreases tissue hypoxia, enhances neovascularization, and supports new collagen and bone formation.
DELAYED EFFECTS OF RADIATION
Delayed effects of radiation are a complication of modern radiotherapy that can be treated with hyperbaric oxygen therapy. Some examples of delayed radiation effects include soft tissue radionecrosis, osteoradionecrosis, radiation cystitis, radiation proctitis, and laryngeal chondroradionecrosis. The basic pathophysiology of delayed radiation tissue damage is endarteritis with resultant tissue hypoxia and secondary fibrosis.
Delayed radiation complications are often manifest as non-healing wounds located in previously irradiated areas and are precipitated by an additional insult such as surgery or trauma within the field of radiation. Hyperbaric oxygen has been shown to induce neovascularization and increase cellularity in irradiated, hypoxic tissues. The success with randomized controlled studies in patients with mandibular osteoradionecrosis has led to successful use of hyperbaric oxygen in other body areas affected by radiation. Dental extractions or other surgical procedures are fraught with high complication rates and a much higher incidence of non-healing when performed in heavily irradiated tissues without the benefit of preoperative hyperbaric oxygen therapy.
Risks versus benefits
The risks and benefits of hyperbaric oxygen therapy should be discussed with each patient.
The benefits include:
- Reduction in the volume of blood’s and tissue’s gas bubble, improved tissue oxygenation and acceleration of nitrogen elimination from the tissues
- Raising the tissue oxygen levels in order to enhance healing of difficult wounds thru neovascularization.
- Raising the tissue oxygen levels to reverse toxic effects of chemicals and inhaled gases.
- Improved post-ischemic tissue survival after reperfusion.
- Bacteriostatic and bacteriocidal effects
- Prevention of bone loss from hypoxic bone lesions [8]
Potential risks include:
- Ear, sinus, tooth, or pulmonary barotraumas. This can result in pain and discomfort in the ears, sinuses, or teeth, and rarely to pneumothorax of the lung
- There are several potential eye changes, most commonly slight worsening of far vision with improvement of near vision. This is reversible without intervention in most cases. Rarely, certain types of cataracts may mature more quickly than in patients not treated with hyperbaric oxygen.
- There is a remote risk of fire. Prohibited items that will not be allowed into the chamber at any time.
- There is the risk of oxygen toxicity that can be manifest as a seizure or lung changes.
- Confinement anxiety [8]
- Chamber fire
Contraindications
Contraindications
Due to Trapped Gas
- Pneumothorax (unvented)
- Intraocular Gas (except for bubble manifestation with decompression sickness)
- Hollow orbital prosthesis
- Acute severe bronchospasm unresolved
- Other rare, gas-filled structures that might develop gas trapping [8]
Due to Oxygen Toxicity
- Bleomycin- concurrent use with HBOT should be avoided
- Doxorubicin- concurrent use with HBOT should be avoided [8]
- Amiodarone- potentially worsening outcome of pulmonary toxicity.The ultimate result of Amiodarone in the face of HBOT is unknown
Relative Risks
Due to trapped Gas
- Chronic Obstructive Pulmonary Disease, specifically emphysema
- Recent pneumothorax
- History of spontaneous pneumothorax
- Chest surgery/trauma
- Dental problems: cavities, incomplete or cracked root fillings [8]
Due to Oxygen Toxicity
- Optic Neuritis if acute
- Retrobulbar optic neuritis
- Retinopathy of prematurity
- Current Bleomycin
- Current Doxorubicin [8]
- Amiodarone - potentially worsening outcome of pulmonary toxicity.The ultimate result of amiodarone in the face of HBOT is unknown
Due to Pressure Change
- Acute upper Respiratory Infection
- Otitis Media- Inability to equalize middle-ear pressure
- Mastoidectomy- Inability to equalize middle-ear pressure
- Cochlear implant- malfunction of internal components
- Implanted devices- pacemakers, defibrillators, shunts-malfunction [8]
Various other Systemic effects
Considerations for Active Cancer and HBOT
Can I treat a patient with HBOT who has active cancer? There is no straight forward answer. Some patients with cancer recur and some develop rapid growth (probably after collapse of their inherent immune response.) This happens whether or not they have HBOT treatments. It would be prudent to include a statement like this into your consent form: "While the vast majority of published papers show no evidence of cancer recurrence or enhanced growth, based on a few papers with very few patients some authors have expressed their concerns about cancer growth. You should take this information under consideration if you decide to have hyperbaric treatments." See attached article by John Feldmeier, DO, FACRO, FUHM in the UHMS Resource Med FAQ's Medical and Patient Care for additional information on this topic. [9][10]
Other considerations to consider are the patients current state of health. Are they nutritionally or immunologically deprived. If the tumor were to grow as a coincidence rather than being caused by HBOT, then the HBOT would be to blame. Please refer to the UHMS Resource Med FAQ's Medical and Patient Care for additional information on this topic.
PATIENT EDUCATION FOR CLINICIANS
How to explain an HBOT intervention to your patients
Below is a brief outline:
"The treatment is painless. At the beginning and end of your treatment, you may notice a feeling of “fullness” in your ears, very much like the feeling when changing altitude in an airplane, driving in the mountains or diving underwater. As your eardrums respond to the changing pressure, you may hear “popping” or “crackling” noises. It is not usually painful, but if you do not fully clear your ears, you may develop an earache. To clear or pop your ears, you will have a water bottle with you in the chamber to help you swallow. We may also treat you with a decongestant spray before each treatment.
After entering the chamber, the door is closed and compression of the oxygen inside begins. You may feel warm for a moment until you reach the desired depth of treatment. After 10 to 15 minutes, compression is complete and the usual feeling of fullness in your ears will disappear. You will continue breathing oxygen for 90 minutes. After 90 minutes, the treatment will come to an end. You may again notice a “popping” or fullness in your ears. If you wear glasses for reading, you may have a few weeks in which you can read without your glasses. If your eyes are normal, your reading vision may temporarily worsen. This does not hurt in any way and is temporary. Do not discard your old corrective lenses.
Heart rhythm is routinely monitored on all patients for the first treatment. For patients with a preexisting heart condition, monitoring may be done with each treatment. If you are diabetic, your blood sugar will need to be taken before and after each treatment."
Hyperbaric Oxygen Therapy patient education materials
CODING, COVERAGE AND REIMBURSEMENT 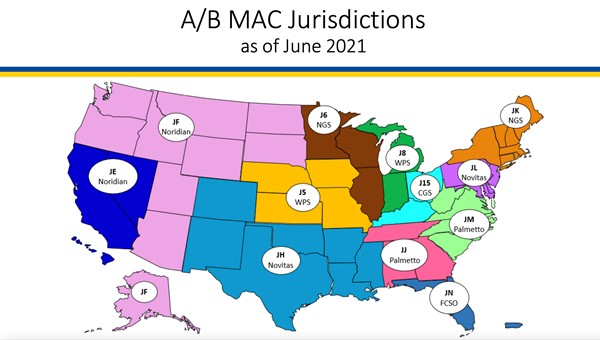
Medicare Administrative Contractor (MAC)
| National or Local Coverage Determination (NCD or LCD)
|
| Novitas Solutions, Inc. |
LCD Hyperbaric Oxygen (HBOT) Therapy (L35021) - Retired [11], NCD 20.29 [12] |
| CGS Administrators, LLC |
NCD 20.29 [12] |
| First Coast Service Options, Inc. (FCSO) |
LCD Hyperbaric Oxygen (HBOT) Therapy (L36504) - Retired [13], NCD 20.29 [12] |
| Noridian |
NCD 20.29 [12] |
| Wisconsin Physicians Service Insurance Corporation (WPS) |
NCD 20.29 [12] |
| National Government Services, Inc. (NGS) |
NCD 20.29 [12] |
| Palmetto |
NCD 20.29 [12] |
More details on requirements, medical necessity and documentation in specific Medicare National and Local Coverage Determinations (if available). To go to NCD or LCD, click on the reference number and on the reference page, click on the green button "View Source Site".
Official reprint from WoundReference® woundreference.com ©2025 Wound Reference, Inc. All Rights Reserved
NOTE: This is a controlled document. This document is not a substitute for proper training, experience, and exercising of professional judgment. While every effort has been made to ensure the accuracy of the contents, neither the authors nor the Wound Reference, Inc. give any guarantee as to the accuracy of the information contained in them nor accept any liability, with respect to loss, damage, injury or expense arising from any such errors or omissions in the contents of the work.