History and Physical
Sample history for Central Retinal Artery Occlusion is shown below:
"Mr. Roberts is a 76 y/o man who awoke this morning with total blindness of the right eye. He went to bed at 10PM last night with good vision bilaterally. He states that he arose once in the middle of the night to urinate. He cannot remember his visual status at the time, but he was not concerned and turned on no lights. This morning at 7AM, he arose and noted no vision in the right eye.
He came to the emergency room for evaluation. The emergency room doctor confirmed that there was no vision in the right eye, and he also confirmed that the retina was pale. The ophthalmologist evaluated Mr. Roberts, performed an injection in the right eye and called us to evaluate the patient for Central Retinal Artery Occlusion.
We noted that the retina has been without blood flow for at least 9 hours from the middle of the night, and at most 12 hours from bedtime the night before. In this situation, time from onset of occlusion is vitally important. This patient is a good candidate for hyperbaric oxygen therapy in hopes to provide oxygen to the damaged retina for the next 36 - 48 hours while the retinal artery recanalyzes. This is an emergent indication for hyperbaric therapy. Failing to act will ensure total, irreversible blindness in the eye. We are happy to assist."
Physical Exam
- Sudden, painless visual loss, generally unilateral
- Findings on fundoscopic exam with dilation:
- Pale yellow/ white-appearing retina due to ischemia or necrosis
- A cherry red spot in the macula (this is finding may not always be present) (Figure 3)
- Other physical exam findings may include an afferent pupillary defect (Marcus Gunn pupil) and segmentation of blood in retinal arterioles (boxcarring)
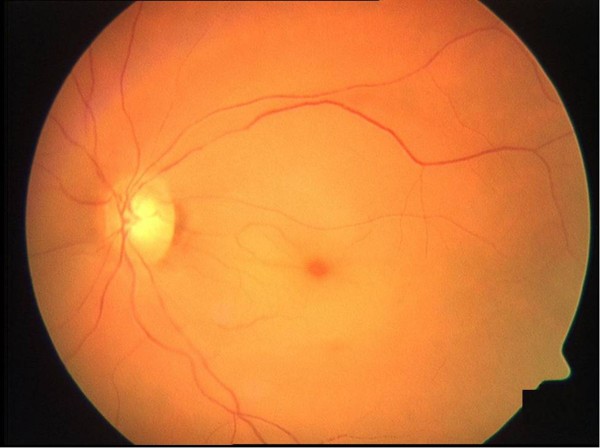
Figure 3. Central retinal artery occlusion with cherry-red spot, retinal edema and narrowing of the vessels.
Impression
- Central Retinal Artery Occlusion Refer to ICD-10 Crosswalk
Plan
There are several treatment options described in the medical literature. Hyperbaric oxygen can be delivered at 2.4 atmospheres absolute with 90 minutes of oxygen breathing during a 120 minute treatment. This will be repeated twice daily until maximum visual acuity is obtained. A second option for treatment involves treating at 2.4 atmospheres absolute for 30 minutes. If there is no improvement in visual acuity, the treatment pressure is increased to 2.8 atmospheres absolute, following a US Navy Treatment Table 6 protocol. Further treatments at 2.4 or 2.8 atmospheres absolute are administered on a twice daily regimen until visual acuity no longer improves.
Risk and Benefit of Hyperbaric Oxygen Therapy
- Please refer to topic "Documentation HBO: Risks and Benefits"
Indication for Hyperbaric Oxygen Therapy (HBOT)
Central retinal artery occlusion (CRAO) is a rare eye disorder that typically produces severe and irreversible vision loss in the affected eye. There is some anatomic variation to the arterial blood supply to the retina. However, these patients usually present to the ophthalmologist with sudden visual loss, generally unilateral, and painless. Once the arterial supply to the retina is occluded, variable degrees of tissue loss occur within 90 to 120 minutes. This may be irreversible without intervention.
A number of different treatment regimens have been used with variable degrees of success. Frequently, there has been no improvement in visual acuity once blood supply to the retina has been lost. There have been a number of different pathophysiologic etiologies described with a common denominator of interrupted arterial supply to the retinal tissue. Here have been several studies showing that addition of HBOT as soon as possible has resulted in increased visual acuity by 2 to 3 lines on a Snellen eye chart. This may make the difference between light perception only to finger counting or television vision.
Hyperbaric Plan
There are several treatment options described in the medical literature. Hyperbaric oxygen can be delivered at 2.4 atmospheres absolute with 90 minutes of oxygen breathing during a 120 minute treatment. This will be repeated twice daily until maximum visual acuity is obtained. A second option for treatment involves treating at 2.4 atmospheres absolute for 30 minutes. If there is no improvement in visual acuity, the treatment pressure is increased to 2.8 atmospheres absolute, following a US Navy Treatment Table 6 protocol. Further treatments at 2.4 or 2.8 atmospheres absolute are administered on a twice daily regimen until visual acuity no longer improves. There is currently AHA Level IIb evidence suggesting that hyperbaric oxygen is helpful.
Sample Order
- See sample physician order
Documentation by Certified Hyperbaric Nurse and Certified Hyperbaric Technician
The certified hyperbaric technician (CHT) and certified hyperbaric nurse (CHRN) should maintain an accurate record of the care and related support services delivered during each patient’s course of hyperbaric oxygen therapy. The patient's chart is a legal document and as such, must reflect in meaningful terms the patient's condition, progress, and care rendered. The provider and nurse's notes must be concise, accurate, and support medical necessity for the treatment ordered. The notes must reflect responsibility for the care rendered. For details, see topic "Documentation: Hyperbaric Treatment Notes by the CHRN and CHT"
Daily treatment should include, but is not limited to the following:
- Physician Order - confirm daily HBO treatment order.
- Patient Assessment (by the CHRN or CHT)
- Pre-treatment Safety Check (by the CHRN or CHT)
- Documentation of the Treatment Log (by the CHRN or CHT)
- Physician Supervision (by the CHRN or CHT)
- Care Provided (by the CHRN or CHT)
- Plan of Care (by the CHRN or CHT, based on physician orders)
CODING
OPERATIONAL CONSIDERATIONS
Providing HBOT in a safe manner is the primary objective with each and every treatment. The clinical team (physician, CHT, CHRN, etc) providing HBOT goes to great lengths to ensure patient safety with every treatment. A summary of operational considerations pertaining to adjunct HBOT for central retinal artery occlusion is provided below:
Chamber Inspections
- Routine chamber inspections should be conducted to confirm chamber maintenance procedures and the safe operation of all equipment utilized during HBOT.
- To ensure the safety of the environment in the hyperbaric medicine facility, chamber inspections are to be performed routinely (i.e. daily, monthly, semi-annually, as needed). Processes and systems that meet standards set forth by The Joint Commission (TJC) and the Undersea and Hyperbaric Medical Society (UHMS) should be utilized, and elements that have been developed within the field (in some cases through “near misses”) may be incorporated. These processes and systems can be implemented through customized patient-centered checklists. Checklists have a wide range of applications, with the potential to improve patient education, pre-procedure planning, discharge instructions, care coordination, chronic care management, and plans for staying well.
- For resources on chamber inspections, see topic "HBO Safety Inspections".
Ground testing
- NFPA 99 requires that all hyperbaric chambers are grounded and patients inside chambers filled with 100% oxygen are likewise grounded. Wrist continuity tests prior to each treatment and daily chamber checks including chamber stud to wall measurements and patient ground jack to chamber stud measurements ensure ongoing continuity.
Prohibited Item(s), Assessment and Authorization
- Wound dressings, devices, and other objects that go in the hyperbaric chamber with the patient may raise important safety concerns, including the production of heat, production of static electricity, production of flammable vapor, ignition temperature, and total fuel load. It is critical that clinicians understand which dressings, devices, and objects are prohibited, restricted or allowed inside a hyperbaric chamber during HBOT for Central Retinal Artery Occlusion.
- Frequently, questions arise in regard to which items are prohibited, restricted or allowed inside a hyperbaric chamber during HBOT. The NFPA 99 2018 edition, chapter 14 "Hyperbaric Facilities", provides the process for effectively managing patient care product(s) during HBOT. The NFPA 99 2018 edition - 14.3.1.6.4.4 states “Physician and Safety Director approval to use prohibited items shall be stated in writing for all prohibited materials employed”.[10]
- Each hyperbaric facility should maintain an internal list of items that are approved for use, should be used with caution and should not be used in the chamber. An authorization form is required for items that should be used with caution. To facilitate assessment, clinicians might opt to utilize the Go-No-Go Risk Assessment Tool. The tool is an interactive process that enables hyperbaric technicians, Safety and Medical Directors to document the product information necessary to complete the risk assessment process. Upon completion of the process, the user will have the ability to print or email the document. In addition, clinicians can review lists of items that are approved for use, should be used with caution and should not be used in the chamber. See " Go-No-Go Lists / Prohibited Items" and "Go-No-Go: Frequently Asked Questions".
Ancillary Equipment
- All equipment utilized by the hyperbaric medicine facility is maintained through a program of regular preventative maintenance. The manufacturer maintains the hyperbaric chambers during the regularly scheduled service contract. Ancillary equipment (e.g. cardiac monitor leads, TCOM sensors) should be serviced by the Hospital's Biomedical Department and maintained in accordance with the recommendations of the manufacturer. See topics "Ear Exam - Barotrauma" and "Ancillary Equipment".
Air Breaks
- During HBOT for central retinal artery occlusion, it is necessary to provide an alternative air breathing source. This may also be necessary to reduce the risk of central nervous system oxygen toxicity. The air breathing system consists of an independent high-pressure air source, capable of providing flow that is sufficient to meet the patient's inspiratory demand. Air breathing systems may be provided by institutional gas outlet (wall outlet) or via portable "H" cylinders utilizing a diameter index safety system (DISS) regulator. Delivery of the air break to the patient may be provided by disposable non-rebreather mask, demand valve and resuscitation mask or trach collar. For purposes of infection control, masks should be single patient use and cleaned or replaced (per patient) as needed.
- While the use of air breaks to decrease the incidence of CNS oxygen toxicity has not been directly demonstrated, there is a large amount of published data on the cause of oxygen toxicity related directly to a combination of the level of FiO2, and time. As such, these air breaks limit the interval time exposure and are expected to decrease the risk of oxygen toxicity. [11]
Infection Control - Cleaning/ Disinfection of the Hyperbaric Chamber
- The cleaning and disinfection of acrylic monoplace chambers is done with caution because many commercial biohazard-cleaning agents contain alcohol. While alcohol is adequate to kill many pathogens, it is destructive to acrylic and can produce flammable fumes and vapors creating a fire hazard in the chamber and the immediate area. Therefore, only manufacturer-approved cleaning products are used for disinfection of the hyperbaric chamber and accompanying equipment. Particular cleaning and disinfecting tasks are divided among staff from environmental services, equipment or biomedical device services, respiratory services, nursing, and other departments of the health care team.
- Adverse outcomes related the risk of infection stands at the forefront of concern for patients with Central Retinal Artery Occlusion. Particular attention should be given to cleaning and disinfection of the hyperbaric chamber acrylic, stretcher and associated equipment, including observing the specific kill times of the solution used prior to the delivery HBOT. See topic: "Cleaning and Disinfection of Hyperbaric Oxygen Monoplace Chamber"
Barotrauma
- Assessment of the patient and their past medical history is necessary to identify and minimize the risk of barotraumas. If the patient has history of sinus, tooth, and ear problems, compress slowly and observe patient for signs of pain.
- Middle-ear barotrauma: The most common type of barotrauma experienced by patients receiving HBOT is middle-ear barotrauma (MEB). Normally, the middle ear is a closed, vascular lined space and therefore subject to pressure change. The normal means by which the middle ear remains at an equal pressure with the surrounding tissue is through the opening of the Eustachian tube. During descent, the increasing pressure of the surrounding water leads to “middle-ear squeeze.” If a patient is suffering from Eustachian tube dysfunction, he or she likely will be unable to equalize and will subsequently develop middle-ear barotrauma. [8]
- Pneumothorax: A complete and accurate pulmonary assessment is essential to avoid or prevent gas expansion problems. Assessing the patient with a significant pulmonary history is a key starting point. Identify any history of asthma, chronic obstructive pulmonary dysfunction (COPD), fibrosis, spontaneous pneumothorax, or chest trauma.
- The absolute contraindication for HBOT is the unvented pneumothorax.
- Signs and symptoms of pneumothorax include: Sudden shortness of breath, Sudden stabbing chest pain, Tracheal shift to affected side in cases of tension, Asymmetrical chest movement (lack or reduced chest excursion on affected side), Increase in respiratory distress with decompression, with relief on recompression. [8]
Blood Glucose Level and HBOT
- It is necessary to ensure that all patients who are currently being treated for irregular blood glucose levels do not experience a hypoglycemic event as a result of ongoing HBOT. Most studies suggest that blood glucose decreases in patients with diabetes who undergo HBOT. This decrease in blood glucose is estimated at 50 mg/dl. HBOT might not be as effective in patients with non-insulin dependent diabetes mellitus patients, compared to patients without diabetes. [8]
- If diabetes mellitus is present, blood glucose should be checked within 1 hour prior to treatment and immediately post-HBOT. The goal is to ensure that all patients who are currently being treated do not experience a hypoglycemic event as a result of ongoing HBOT. Hypoglycemia in the hyperbaric environment may present similar symptoms as oxygen toxicity, including but not limited to sweating, pale skin, shakiness, anxiety, tingling or numbness of the tongue or cheek. See section 'Blood Glucose Level and HBOT' in topic "Patient Care".
Medications in the hyperbaric environment
- The hyperbaric environment creates numerous considerations for the use of drug therapies within it. Physiologic changes to the body due to HBOT may lead to pharmacokinetic changes in drug disposition. In addition, HBO acting as a drug can interact and enhance or lessen the physiologic effect of the drug. Most drugs will not interact unfavorably with oxygen. Unless specific contraindications or precautions have been addressed, it is generally safe to assume a medication can be used. [8] Pharmacodynamic interactions result in modification of the pharmacologic effect of the drug after administration. These interactions will increase or decrease the effects of oxygen or the drug. [8]
- Patients receiving antibiotics with elastomeric infusion pumps (also known as "space balls") may continue to receive antibiotics in the chamber, however infusion amounts during changes of atmospheric pressure should still be monitored. If the pump is full of air, then it may not provide standardized infusion rate. A study shows that the antibiotic flow rate for ceftazidime 6 g is not significantly affected by increases in ambient pressure across the pressure range of 101.3 kPa to 284 kPa. However, there was evidence that the specific antibiotic solution might affect flow rates and this requires further study.
- For potential interactions of drugs administered to patients with chronic refractory osteomyelitis, see topic "Medications In The Hyperbaric Environment".
Oxygen Toxicity
- The hyperbaric staff should be skilled in reducing the potential for and management of oxygen toxicity for the patient receiving HBOT.
- Central Nervous System (CNS) oxygen toxicity can occur in patients breathing oxygen at pressures of 2.0 ATA (atmosphere absolute) or greater. Convulsions may occur abruptly or may be preceded by other signs of central nervous system irritability. [8] Early estimates of the seizure rate during therapeutic oxygen exposures at 2-3 ATA reported a convulsion incidence of about one per 10,000 therapies or 0.01%. [8]
- The hyperbaric physician will be notified immediately if a patient experiences signs or symptoms of oxygen toxicity during HBOT.
CNS toxicity
- Observe patient closely for premonitory signs and symptoms of CNS Oxygen Toxicity such as:
- V : vision-visual changes, blurred vision, visual hallucinations
- E : Ears- Auditory hallucinations, ringing in the ears
- N : Nausea- May include emesis
- T : Twitching- Restlessness, numbness, focal twitching (note time, duration and site)
- I : irritability- Change in personality
- D : Dizziness- Vertigo
- C : Convulsions- Seizure activity
- C : Change in mentation - Change in affect or of a non-descriptive complaint like, “I just don’t feel right” [12]
Pulmonary Oxygen Toxicity
- Most current applications of HBOT do not cause pulmonary symptoms or clinically significant pulmonary functional deficits. [13] Prolonged exposure to oxygen pressures greater than 0.5 ATA is associated with the development of intratracheal and bronchial irritation. Pulmonary oxygen toxicity is not expected from routine daily HBOT. The possibility of development does exist with prolonged exposure most typically related to long treatment tables such as US Navy Treatment Table 6 used for decompression illness, but even these cases would be mild and self-limiting. [14]
- Continued oxygen exposure may lead to impaired pulmonary function and eventually acute respiratory distress syndrome (ARDS). Symptoms include:
- Substernal burning,
- Chest tightness
- Cough
- Dyspnea
- These changes are seen over the course of days to weeks at lower oxygen pressures and occur more rapidly as the oxygen pressure is increased. [8]
Ocular Oxygen Toxicity
- Vision changes as a side effect of HBOT have been observed in patients undergoing prolonged periods of daily HBOT. The rate of these changes has been reported in the literature to be ∼0.25 diopter per week and progressive throughout the course of ongoing treatment. Myopia has been reported in 25–100% of patients undergoing HBOT after several weeks at pressures of 2.0 ATA and greater. [14] When providing HBO for the patient being treated for chronic refractory osteomyelitis it is important to discuss the risks, hazards and potential side effects with the patient and family. Documentation of this discussion and patient/ family's understanding should be clearly stated in the patient record. For further information See topic:"Hyperbaric Oxygen Therapy and Visual Acuity"
NURSING INTERVENTIONS
Nursing interventions that are relevant for adjunct HBOT of chronic refractory osteomyelitis are presented below. [15] For further information see topic "Nursing Interventions".
Knowledge deficit related to hyperbaric oxygen therapy and treatment procedures
- Assess and document the patient and/or family's understanding of purpose and goals of hyperbaric oxygen therapy (HBO), procedures involved, and potential hazards of HBO.
- Utilize the teach-back method to confirm patient understanding and identify and address barriers to learning. Involve an interpreter if indicated, apply age-specific teaching, consider cultural/religious factors, assess readiness to learn, and identify patient's expectations of treatment.
- See section 'Knowledge deficit related to hyperbaric oxygen therapy and treatment procedures' in topic "Nursing Intervention"
Anxiety related to hyperbaric oxygen treatments or other medical problems
- Assess the patient for a history of confinement anxiety and implement preventative measures as appropriate. It is important to reinforce to patient that someone will always be with them, and the staff are well trained for emergency procedures. Identify signs of symptoms of anxiety before and during HBO treatment such as:
- Patient states anxiety
- Tense-appearing facial/body posturing
- Complaint of nausea or diarrhea
- Feelings of being confined or smothered
- Defensive or argumentative attitude
- Hyperventilation
- Diaphoresis and hyperventilation
- Tachycardia
- Restlessness
- Sudden feeling of being hot
- See section 'Anxiety related to hyperbaric oxygen treatments or other medical problems' in topic "Nursing Intervention"
Potential for injury within the hyperbaric facility related to transferring the patient in and out of the chamber
- When transferring a patient that is being treated for chronic refractory osteomyelitis, comply with the facility's fall risk prevention policy. Prior to transfer of the patient assess fall risk and safety precautions. Communicate and involve patient with the plan of action and provide patient education regarding safety precautions. Provide assistance with transfers as patient needs apply to ensure compliance with institutional/facility policy.
Potential for injury related to fire within the hyperbaric chamber
- Fuel sources in an oxygen-enriched environment are an unavoidable circumstance of HBOT and include linens, equipment, dressings, and the patient. The fire triangle consists of oxygen, fuel, and an ignition source (heat). In HBOT an ignition source is needed to complete the fire triangle. This may occur due to a spark in the chamber. Follow facility fire prevention steps and NFPA chapter 14 probes for Class A and Class B hyperbaric chambers. HBOT teaching and consent should include the risks of fire in the chamber. Provide the patient and family with written instructions regarding the risk of prohibited materials during HBOT. Prior to each hyperbaric treatment, staff should perform and document the pre-treatment safety checklist. Ensure this has been performed and time-stamped prior to descent. Patients receiving treatment for chronic refractory osteomyelitis may have surgical dressings that are ordered to remain intact. A risk assessment per the Safety Director in collaboration with the Medical Director to determine if they may enter the chamber on a case by case basis. Safety measures should be initiated if the risk assessment allows for item to enter the chamber as well as completion of a prohibited item's authorization form signed by the Safety and Medical Directors.
Potential for injury related to changes in atmospheric pressure within the hyperbaric chamber
- Assess patient's and inside attendant's knowledge of ear clearing techniques and ability to equalize pressure. Collaborate with provider to assess tympanic membrane (TM) for suspected barotrauma prior to and after the first HBO treatment and per patient complaint. Collaborate with the provider to describe and document observations including color and visibility of TM, presence of wax, blood/fluid/air and any hearing deficits or changes. Methods to equalize pressure in the middle ear during HBO treatment include: yawning, swallowing, jaw thrust, head tilt, Valsalva, Toynbee, Roydhouse, Frenzel, etc. Reinforce the importance of notifying the chamber operator immediately when pressure or fullness is felt in the middle ear.
Potential for unstable blood glucose level related to hyperbaric oxygen therapy and disease pathology
- Literature notes hyperbaric oxygen therapy carries its own mechanism for increased glucose usage through oxygen-mediated transport of glucose into muscle cells and may also increase insulin sensitivity. Prevention of acute hypoglycemia in the hyperbaric chamber is vital for patient safety. Follow facility policy and procedure guidelines for pre and post-treatment glucose control. Prior to treatment assess the patient's knowledge level, recent hypoglycemic events, and patient-specific symptoms of hypoglycemia. Proper glucose control < 200mg/dL is vital for wound healing. Consider timing of short and long-acting glycemic control medications when scheduling HBO to avoid peak action time while at depth in the chamber.
CATEGORY A CONTINUING EDUCATION CREDIT
This topic has been reviewed and approved by the National Board of Diving and Hyperbaric Medical Technology (NBDHMT) for one (1) Category A Credit.
To claim the credit:
- 1. Read the topic
- 2. Answer the examination and course critique questions.
- Take the quiz via CliniPaths by Wound Reference
- To receive a certificate, a passing score of 70% is required
- 3. After passing, click the provided link to access your certificate. If prompted, sign into your WoundReference account.
For more information on Category A continuing education credits see blog post "Hyperbaric Certification and Continuing Education for Technicians & Nurses".
REVISION UPDATES