SECTION I: ACTIVE DIAGNOSES
This section includes three items that identify active diagnoses and co-morbidities.
Background
Definitions
- Primary diagnosis: the chief reason the patient is receiving home care and the diagnosis most related to the current home health Plan of Care
- Other diagnoses: comorbid conditions that exist at the time of the assessment that are actively addressed in the patient’s Plan of Care - OR - that have the potential to affect the patient’s responsiveness to treatment and rehabilitative prognosis, even if the condition is not the focus of any home health treatment itself.
- ICD-10-M: a morbidity classification published by the United States for classifying diagnoses and reasons for care in all healthcare settings. The ICD-10-CM is based on the ICD-10, the International Classification of Disease published by the World Health Organization (WHO).
- Active diagnoses: active diagnoses are diagnoses that have a direct relationship to the patient’s current functional, cognitive, mood or behavior status; medical treatments; nurse monitoring; or risk of death at the time of assessment
Wound-related ICD-10 Coding
- For wound-related ICD-10 codes, refer to:
M1021/M1023: Primary Diagnosis/Other Diagnoses
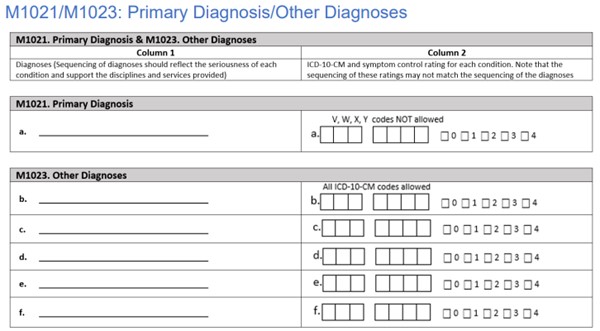
Item Intent
The intent of these items is to accurately report and enter ICD-10 CM codes for the patient’s primary (M1021) and other (M1023) home health diagnoses and document the degree of symptom control for each diagnosis.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
Response-Specific Instructions
Identifying Primary (M1021) and Other (M1023) Diagnoses
- The assessing clinician must determine the primary and other home health diagnoses based on the assessment findings, information in the medical record including but not limited to physician/allowed practitioner orders, medication list and referral information, and input from the physician/allowed practitioner.
- The assessing clinician is expected to complete the patient’s comprehensive assessment and understand the patient’s overall medical condition and care needs before assigning diagnoses.
- The assessing clinician may elicit input from other agency staff that have had direct in-person contact with the patient or have had some other means of gathering information to contribute to the OASIS data collection.
- The primary diagnosis (M1021) and other diagnoses (M1023) may or may not relate to the patient’s most recent hospital stay, but must meet the definitions of primary and other diagnoses presented in this guidance.
- Diagnoses may change during the course of the home health stay due to a change in the patient’s health status or a change in the focus of home health care. At each required OASIS time point, the assessing clinician must assess the patient’s clinical status and determine the primary and other diagnoses based on patient status and treatment plan at the time of the assessment.
- Only current diagnoses should be reported as primary and secondary diagnoses in M1021 and M1023.Diagnoses should be excluded if they are resolved or do not have the potential to impact the skilled services provided by the HHA. An example of a resolved condition is cholecystitis following a cholecystectomy
Reporting ICD-10-CM codes for Primary (M1021) and Other (M1023) Diagnoses
- Adherence to the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10- CM) Official Guidelines for Coding and Reporting when assigning ICD 10 CM diagnosis codes is required under the Health Insurance Portability and Accountability Act (HIPAA). It is expected that each agency will ensure that diagnoses and ICD-10-CM codes reported in OASIS meet these guidelines.
- The assessing clinician can enter the ICD-10-CM codes. Alternatively, a coding specialist in the agency may enter the actual numeric ICD-10-CM codes in Column 2, as long as the assessing clinician has determined the primary and other diagnoses in Column 1.
Reporting the Symptom Control Rating in Column 2
- Assessing degree of symptom control includes but is not limited to review of presenting signs and symptoms, type and number of medications, frequency of treatment readjustments, and frequency of contact with health care providers.
- Inquire about the degree to which each condition limits daily activities.
- Assess the patient to determine if symptoms are controlled by current treatments.
- Clarify which diagnoses/symptoms have been poorly controlled in the recent past.
Coding Instructions
- Column 1, Diagnoses:
- Enter the description of each diagnosis
- List each diagnosis for which the patient is receiving home care
- Diagnoses are listed in the order that best reflects the seriousness of each condition and supports the disciplines and services provided
- Complete Column 1 from top to bottom, leaving any blank entries at the bottom.
- Order other diagnoses (M1023) according to the degree they impact the patient’s health and need for home health care, rather than the degree of symptom control.
For example, if a patient is receiving home health care for Type 2 Diabetes that is “controlled with difficulty” this diagnosis would be listed above a diagnosis of a fungal infection of a toenail that is being treated, even if the fungal infection is “poorly controlled.”
- Column 2, ICD-10 CM codes:
- For each diagnosis in Column 1, enter its ICD-10 CM code at the highest level of specificity
- No surgical or procedure codes allowed in Column 2
- ICD-10-CM sequencing requirements must be followed if multiple coding is indicated for any diagnoses.
- External cause codes (ICD-10-CM codes beginning with V, W, X, or Y) may not be reported in M1021 (Primary Diagnosis) but may be reported in M1023 (Other Diagnoses).
- When a Z-code is reported in Column 2, the code for the underlying condition can often be entered in Column 2, as long as it is an active on-going condition impacting home health care.
- See the ICD-10-CM “Official Guidelines for Coding and Reporting” for complete instructions on code assignment and sequencing related to the use of Z-codes, and use of multiple coding for a single condition (such as manifestation/etiology pairs).
- For wound-related ICD-10 codes, refer to topic “ICD-10-CM Diagnosis Codes”, then click on the Subtopic corresponding to the current year for a searchable tool with wound care-specific ICD-10 Codes (e.g. “Wound Care ICD-10 Codes for 2024”)
M1028: Active Diagnoses – Comorbidities and Co-existing Conditions

Item Intent
This item identifies whether two specific diagnoses are present and active. These diagnoses influence a patient’s functional outcomes or increase a patient’s risk for development or worsening of pressure ulcers/injuries.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
Response-Specific Instructions
- Identify diagnoses: The diseases and conditions in this item require a physician (or nurse practitioner, physician assistant, clinical nurse specialist, or other authorized licensed staff if allowable under state licensure laws) documented diagnosis be present at the time of assessment.
- Clinical record sources for these diagnoses include, but are not limited to transfer documents, physician/allowed practitioner: progress notes, recent history and physical, discharge summary, orders, and consults.
- Do not include diseases or conditions that have been resolved or do not affect the patient’s current functional, cognitive, mood or behavior status; medical treatments; nurse monitoring; or risk of death at the time of assessment.
- Diagnostic information, including past medical and surgical history obtained from family members and close contacts, must also be documented in the clinical record by the physician (or others as listed above) to ensure validity, follow-up, and coordination of care.
- Only diagnoses confirmed and documented by the physician (or others, as listed above) should be considered when coding this item.
- Determine whether diagnoses are active: Once a diagnosis is identified, determine whether the diagnosis is active.
- If information regarding active diagnoses is learned after the end of the assessment timeframe, the OASIS item should not be revised to reflect this new information. The OASIS should reflect what was documented at the time of the assessment. If, however, it comes to light after the OASIS assessment is submitted an error occurred, where a documented active diagnosis was initially present but not indicated on the OASIS, the Home Health Agency should correct the OASIS following the agency’s correction policy and M0090 would not necessarily be changed.
Coding Instructions
- Code 1, Peripheral Vascular Disease (PVD) or Peripheral Arterial Disease (PAD), if the patient has an active diagnosis of Peripheral Vascular Disease (PVD) or Peripheral Arterial Disease (PAD).
- Code 2, Diabetes Mellitus (DM), if the patient has an active diagnosis of Diabetes Mellitus (DM).
- Code 3, None of the Above, if the patient does not have any of the active diagnoses listed above.
- Dash is a valid response for this item.
- Dash indicates “no information.” CMS expects dash use to be a rare occurrence.
Coding Tips
The following tips may assist staff in determining whether a disease or condition should be coded as an active diagnosis.
- The physician (nurse practitioner, physician assistant, clinical nurse specialist, or other authorized licensed staff if allowable under state licensure laws) may specifically indicate that a diagnosis is active.
- If there is documentation in the clinical record that a patient has diabetes mellitus, select Response 2, Diabetes Mellitus (DM). If there is only documentation in the clinical record of a complication such as nephropathy or neuropathy and there is no documentation that the patient has diabetes, it should not be assumed the complication is associated with diabetes, and Response 2, Diabetes Mellitus, should not be checked.
- If a diabetic patient has either PAD or PVD both Response 1 and Response 2 should be checked.
- The physician (nurse practitioner, physician assistant, clinical nurse specialist or other authorized licensed staff if allowable under state licensure laws) for example, documents at the time of assessment that the patient has inadequately controlled diabetes and requires adjustment of the medication regimen. This would be sufficient documentation of an active diagnosis and would require no additional confirmation because the physician documented the diagnosis and also confirmed that the medication regimen needed to be modified.
Examples
- Active Diagnosis of Diabetes Mellitus. A patient is prescribed insulin for diabetes mellitus. They require regular blood glucose monitoring to determine whether blood glucose goals are achieved by the current medication regimen. The physician progress note documents diabetes mellitus.
- Coding: M1028, Active Diagnoses, would be coded 2, Diabetes Mellitus.
- Rationale: This would be considered an active diagnosis because the physician progress note documents the diabetes mellitus diagnosis, and because there is ongoing medication management and glucose monitoring.
- None of the Above. During the SOC/ROC assessment, a patient told Nurse J, RN that they have had diabetes for 20 years. Nurse J reviewed the transfer documents from the acute care facility and all clinical records on the patient but was unable to find a documented diagnosis of Diabetes Mellitus by physician, nurse practitioner, physician assistant or authorized licensed staff member in their state. There is no documented diagnosis of PVD or PAD.
- Coding: M1028, Active Diagnoses, would be coded 3, None of the Above.
- Rationale: This would be considered a “none of the above” response because the nurse was unable to find the diagnosis of diabetes at the time of assessment, documented by a physician (or nurse practitioner, physician assistant, clinical nurse specialist, or other authorized licensed staff if allowable under state licensure laws). And, there is no documented diagnosis of PVD or PAD.
SECTION M: SKIN CONDITIONS
This section includes items that assess the presence of pressure ulcers/injuries (PU/PI), stasis ulcers (also known as venous leg ulcers or VLU) and surgical wounds.
Background
Definitions
- Epithelialization or re-epithelialization: regeneration of the epidermis across a wound surface.[1] Translucent cell layer comprised of epithelial cells migrating to the wound bed, from wound edge or epidermal appendages. New epidermis appears pink and dry (Figures 1 to 3).
- Non-epithelialized wound: the absence of regenerated epidermis across a wound surface (Figure 2).
- Newly epithelialized wound: when epithelial tissue has completely covered the wound surface, regardless of how long the wound has been re-epithelialized (Figure 3).
- In the context of a surgical wound: epithelialization is characterized by “epidermal resurfacing” meaning the opening created during the surgery is covered by epithelial cells. If there is no interruption in the healing process, this generally takes within a matter of hours to three days postoperatively.[1]
- Eschar: dead or devitalized tissue that is hard or soft in texture; usually black, brown or tan in color, and may appear scab-like. Necrotic tissue and eschar are usually firmly adherent to the base of the wound and often the sides/edges of the wound (Figures 4 to 6).
- Granulation: pink/red tissue that forms when wound is healing. It contains connective tissue, blood vessels and cells needed for wound repair. Tissue is healthy when bright, beefy red, shiny and granular with a velvety appearance (Figures 7 to 9). It is important to differentiate granulating wounds from clean, but non-granulating wounds (Figures 10 to 12).
- Hypergranulation: granulation tissue overgrows the filled-in wound bed
- Non-removable Dressing/Device: examples of a non-removable dressing/device include a dressing that is not to be removed per physician’s/allowed practitioner’s order (such as those used in negative pressure wound therapy [NPWT], an orthopedic device, or a cast).
- Pressure Ulcer/Injury: localized injury to the skin and/or underlying tissue usually over a bony prominence, as a result of intense and/or prolonged pressure, or pressure in combination with shear and/or friction. The PU/PI can present as intact skin or an open ulcer and may be painful.
- Slough: non-viable yellow, tan, gray, green or brown tissue; usually moist, can be soft, stringy and mucinous in texture. Slough may be adherent to the base of the wound or present in clumps throughout the wound bed (Figures 13 to 15).
- Wound bed: base of the wound. The type and amount of tissue present in the wound bed are crucial early indicators of wound progression. Multiple tissue types may be present, and their relative proportions should be carefully estimated to assess the wound status accurately (Figure 16).
 Fig. 1. Non-epithelialized wound | 
Fig. 2. Epithelialization | 
Fig. 3. Newly epithelialized |

Fig. 4. Eschar: dry, adherent, hard | 
Fig. 5. Eschar: firmly adherent, hard | 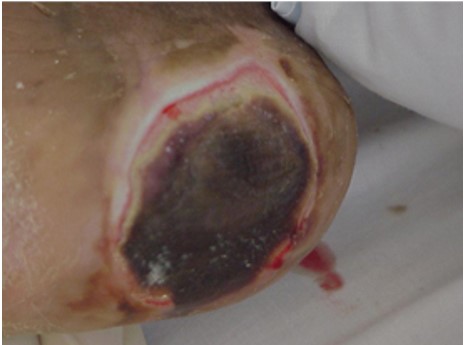
Fig. 6. Eschar: loose, soft, spongy |
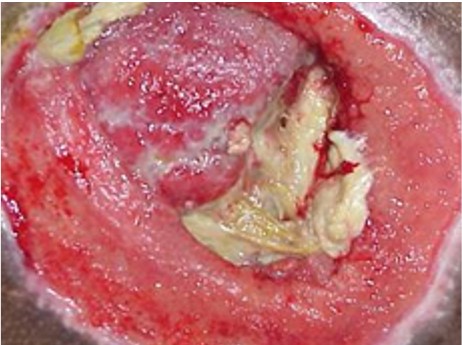
Fig. 7. Granulating: pink, red | 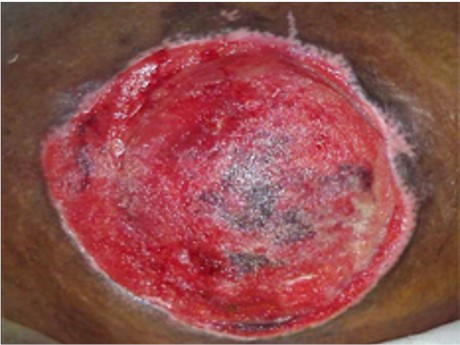
Fig. 8. Granulating: red | 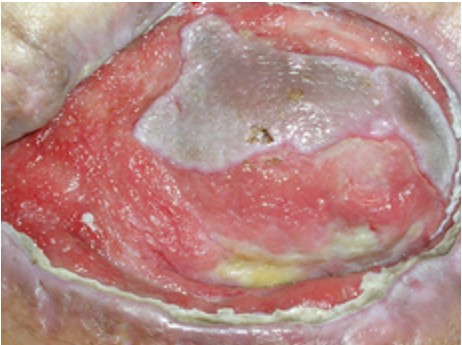
Fig. 9. Granulating: pink |
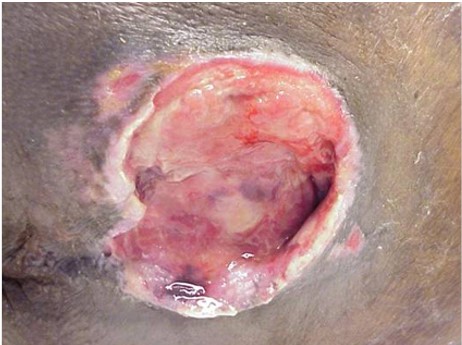
Fig. 10. Clean, but non-granulating wound | 
Fig. 11. Clean, but non-granulating, dusky, pale wound | 
Fig. 12. Clean, but non-granulating friable wound |

Fig. 13. Slough: moist, loose | 
Fig. 14. Slough: moist, adherent | 
Fig. 15. Slough: soft, moist |
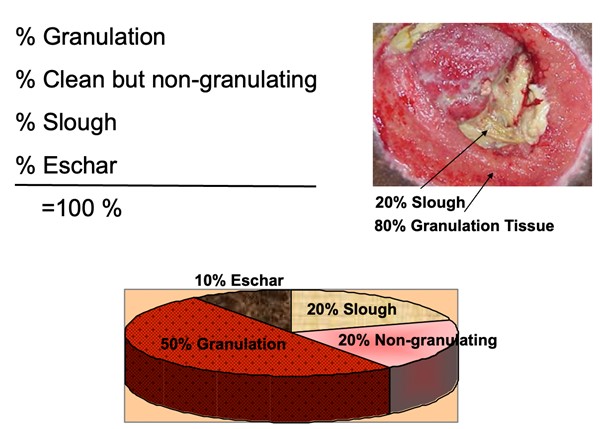
Fig. 16. Estimation of wound bed tissue type proportion
Pressure Ulcers/Injuries
This section summarizes CMS OASIS Instructions related to PU/PI. For an introduction and assessment of PU/PI including epidemiology, risk factors, etiology, pathophysiology, history, physical examination, diagnosis, differential diagnoses, documentation and ICD-10 coding, see "
Pressure Ulcers/Injuries - Introduction and Assessment".
The following CMS OASIS Instructions apply to all OASIS E items related to pressure ulcers/injuries (PU/PI)
[1]:
- The presence of pressure ulcers/injuries and unstageable ulcers/injuries should be determined by physical assessment and observation. Medical records, patient/caregiver report and physician input may be used for historical purposes only to identify the presence of an existing ulcer/injury or the stage of a previously healed pressure ulcer.
- Review the history of each pressure ulcer/injury in the clinical record. If the pressure ulcer/injury was previously classified at a higher numerical stage than what is observed now, as long as it remains stageable, it should continue to be classified at the higher numerical stage until healed.
PU/PI Risk Assessment
PU/PI Classification
- Home health agencies may adopt the National Pressure Injury Advisory Panel (NPIAP) guidelines in their clinical practice and documentation. However, since CMS has adapted the NPIAP guidelines for OASIS purposes, the definitions do not perfectly align with each stage as described by NPIAP. When discrepancies exist between the NPIAP definitions and the OASIS scoring instructions provided in the OASIS Guidance Manual and CMS Q&As, providers should rely on the CMS OASIS instructions (Table XX)
- See topic “Pressure Ulcers/Injuries - Classification/Staging”
Table 5. Pressure Ulcers/Injuries Staging per CMS OASIS Instructions [1] Pressure Ulcers/Injuries staging per CMS OASIS instructions
|
- Stage 1 Pressure Injury: an observable, pressure-related alteration of intact skin whose indicators, as compared with an adjacent or opposite area on the body, may include changes in one or more of the following parameters: skin temperature (warmth or coolness); tissue consistency (firm or boggy); sensation (pain, itching); and /or a defined area of persistent redness in lightly pigmented skin. In darker skin tones, the injury may appear with persistent red, blue or purple hues.
- Stage 2 Pressure Ulcer : stage 2 pressure ulcers are characterized by partial thickness loss of dermis presenting as a shallow open ulcer with a red-pink wound bed, without slough or bruising. May also present as an intact or open/ruptured serum-filled blister.
- Stage 3 Pressure Ulcer : stage 3 pressure ulcers are characterized by full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle is not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining or tunneling.
- Stage 4 Pressure Ulcer : stage 4 pressure ulcers are characterized by full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often includes undermining and tunneling.
- Deep Tissue Injury: a purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue
|
M1306: Unhealed Pressure Ulcer/Injury at Stage 2 or Higher

Item Intent
- Identifies the presence or absence of Unhealed Stage 2 or higher or Unstageable pressure ulcers/injuries only.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
- Follow-up
- Discharge from agency
Coding Instructions
- Code 0, No, if the only pressure ulcer/injury is one or more Stage 1 OR healed pressure ulcers/injuries (of any previous stage) AND the patient has no other pressure ulcers/injuries.
- Code 1, Yes, if the patient has an unhealed Stage 2, Stage 3, OR Stage 4 pressure ulcer OR if the patient has an Unstageable ulcer/injury.
- Dash is not a valid response for this item.
Response-Specific Instructions
- Review the history of each pressure ulcer/injury in the clinical record. If the pressure ulcer/injury was previously classified at a higher numerical stage than what is observed now, as long as it remains stageable, it should continue to be classified at the higher numerical stage until healed.
Coding Tips
- If pressure is not the primary cause of the lesion, do not report the wound as a pressure ulcer/injury.
- Stage 1 pressure injuries and Deep Tissue Injury (DTI), although closed (intact skin), would not be considered healed. Unstageable pressure ulcers/injuries, whether covered with a non- removable dressing or eschar or slough, would not be considered healed.
- Stage 2 (partial thickness) pressure ulcers heal through the process of regeneration of the epidermis across a wound surface, known as “re-epithelialization.”
- Stage 3 and 4 (full thickness) pressure ulcers heal through a process of granulation (filling of the wound with connective/scar tissue), contraction (wound margins contract and pull together), and re-epithelialization (covers with epithelial tissue from within wound bed and/or from wound margins). Once the pressure ulcer has fully granulated and the wound surface is completely covered with new epithelial tissue, the wound is considered closed, and will continue to remodel and increase in tensile strength. For the purposes of scoring the OASIS, the wound is considered healed at this point, and should no longer be reported as an unhealed pressure ulcer.
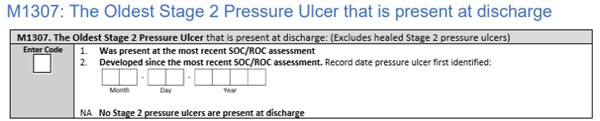
M1307: The Oldest Stage 2 Pressure Ulcer that is present at discharge
Item Intent
The intent of this item is to:
- Identify the oldest Stage 2 pressure ulcer that is present at the time of discharge and is not fully epithelialized (healed),
- Assess the length of time this ulcer remained unhealed while the patient received care from the home health agency, and
- Identify patients who develop Stage 2 pressure ulcers while under the care of the agency.
Item Rationale
- Stage 2 pressure ulcers may worsen without proper interventions.
- These patients are at risk for further complications or skin injury.
Time Points Item(s) Completed
Response-Specific Instructions
- Do not reverse stage pressure ulcers as a way to document healing as it does not accurately characterize what is physiologically occurring as the ulcer heals. For example, over time, even though a Stage 4 pressure ulcer has been healing and contracting such that it is less deep, wide, and long, the tissues that were lost (muscle, fat, dermis) will never be replaced with the same type of tissue. Clinical standards require that this ulcer continue to be documented as a Stage 4 pressure ulcer until it has healed or becomes unstageable.
- Stage 2 (partial thickness) pressure ulcers heal through the process of regeneration of the epidermis across a wound surface called, “re-epithelialization.”
- An ulcer that is suspected of being a Stage 2, but is Unstageable due to non-removable dressing/device at the time of discharge, should not be identified as the “oldest Stage 2 pressure ulcer”.
Coding Instructions
- Dash is not a valid response for this item.
- If a Stage 2 PU/PI is present at discharge:
- If the oldest Stage 2 pressure ulcer that is present at discharge was already present as a Stage 2 pressure ulcer at the first skin assessment completed at the most recent SOC/ROC, code “1, Was present at the most recent SOC/ROC assessment”
- If the oldest Stage 2 pressure ulcer that is present at discharge was NOT a Stage 2 pressure ulcer at the first skin assessment completed at the most recent SOC/ROC, code “2, Developed since the most recent SOC/ROC assessment”.
- Example: If no pressure ulcer existed at the SOC, then a Stage 1 pressure injury developed, which progressed to a Stage 2 by discharge, code “2, Developed since the most recent SOC/ROC assessment”.
- If Code 2 is entered, specify the date the Stage 2 pressure ulcer was first identified. Use two digits to indicate the month (for example, May is 05), single-digit dates should begin with 0, and use four digits to indicate the year (for example, May 4, 2021 would be 05/04/2021).
- If no Stage 2 PU/PI is present at discharge
- If there are no Stage 2 pressure ulcers at the time of discharge, or all previous Stage 2 pressure ulcers have healed, code ”NA, No Stage 2 pressure ulcers are present at discharge”
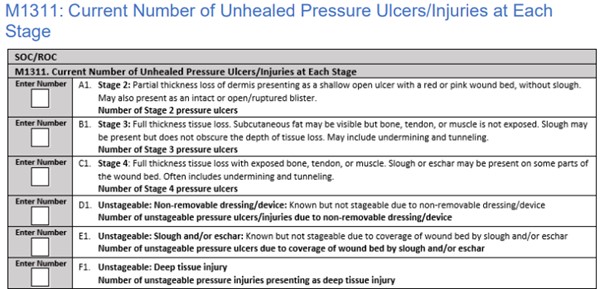
M1311: Current Number of Unhealed Pressure Ulcers/Injuries at Each Stage

Item Intent
- This item identifies the number of pressure ulcers/injuries at each stage (Stage 2, 3, and 4) and designated as Unstageable, that are observed on assessment.
- At discharge, this item also identifies if each pressure ulcer/injury present on the discharge assessment was observed at the same stage at the time of the most recent SOC/ROC.
- Stage 1 pressure injuries and all healed pressure ulcers/injuries are not reported in this item
Item Rationale
- It is important to recognize and evaluate each patient’s risk factors for developing skin ulcers, wounds or lesions, and to identify and evaluate all areas at risk of constant pressure. A complete assessment of skin is essential to an effective pressure ulcer/injury prevention and skin treatment program. It is imperative to determine the etiology of all wounds and lesions, as this will determine and direct the proper treatment and management of the wound.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
- Discharge from agency
Response-Specific Instructions
- If the patient has been in an inpatient setting for some time, it is conceivable that the wound has already started to granulate, thus making it challenging to know the highest numerical stage of the wound. The clinician should make every effort to contact previous providers (including the patient's physician) to determine the highest numerical stage of the pressure ulcer.
- The general standard of practice for patients starting or resuming care is that patient assessments are completed as close to the actual time of the SOC/ROC as possible.
- For example, if a pressure ulcer/injury that is identified on the SOC date increases in numerical stage within the assessment time frame, the stage of the pressure ulcer/injury at the first skin assessment completed would be reported in M1311X1 at the SOC.
- When the assessing clinician is unable to complete a full skin assessment at the first visit, the assessing clinician may collaborate with a second clinician who completes the first clinical skin assessment within the assessment timeframe, if the HHA policy permits.
- Stage 2 Pressure Ulcers (M1311A1)
- Report in M1311A1 the number of Stage 2 pressure ulcers that are observed on the current day of assessment.
- Examine the area adjacent to or surrounding an intact blister for evidence of tissue damage. If other conditions are ruled out and the tissue adjacent to or surrounding the blister demonstrates signs of tissue damage (e.g., color change, tenderness, bogginess or firmness, warmth or coolness), these characteristics suggest a deep tissue injury (DTI) rather than a Stage 2 pressure ulcer.
- Granulation tissue, slough, and eschar are not present in Stage 2 pressure ulcers
- Stage 3 Pressure Ulcer (M1311B1)
- Report in M1311B1 the number of Stage 3 pressure ulcers that are observed on the current day of assessment.
- A previously closed Stage 3 pressure ulcer that is currently open again should be reported as a Stage 3 pressure ulcer, unless currently presenting at a higher stage or unstageable.
- Stage 4 Pressure Ulcer (M1311C1)
- Report in M1311C1 the number of Stage 4 pressure ulcers that are observed on the current day of assessment
- If any bone, tendon or muscle or joint capsule (Stage 4 structures) is visible, the pressure ulcer should be reported as a Stage 4 pressure ulcer, regardless of the presence or absence of slough and/or eschar in the wound bed.
- A previously closed Stage 4 pressure ulcer that is currently open again should be reported as a Stage 4 pressure ulcer, unless currently unstageable.
- Unstageable Ulcers/Injury: Non-removable dressing/device (M1311D1)
- Report in M1311D1 the number of pressure ulcers/injuries that on the current day of assessment are known but not stageable due to non-removable dressing/device.
- Pressure ulcers/injuries that are known to be present but that are Unstageable due to a non-removable dressing/device, such as a cast that cannot be removed to assess the skin underneath,should be reported in M1311D1, Unstageable.
- “Known” refers to when documentation is available that states a pressure ulcer/injury exists under the non-removable dressing/device. Unstageable pressure ulcers/injuries covered with a non-removable dressing would not be considered healed.
- Unstageable Ulcers: Slough/Eschar (M1311E1)
- Report in M1311E1 the number of pressure ulcers that on the current day of assessment are unstageable due to coverage of wound bed by slough and/or eschar.
- Pressure ulcers that have eschar or slough tissue present such that the anatomic depth of soft tissue damage cannot be visualized in the wound bed, should be classified as unstageable.
- If the wound bed is only partially covered by eschar or slough, and the anatomical depth of tissue damage can be visualized, numerically stage the ulcer, and do not code this as unstageable.
- Pressure ulcers that are covered with slough and/or eschar, and the wound bed cannot be visualized, should be coded as unstageable because the true anatomic depth of soft tissue damage (and therefore stage) cannot be determined. Only when enough slough and/or eschar is removed to expose the anatomic depth of soft tissue damage involved, can the stage of the wound be determined.
- Unstageable pressure ulcers due to eschar or slough would not be considered healed.
- Unstageable: Deep Tissue Injury (DTI) (M1311F1)
- Report in M1311F1 the number of unstageable pressure injuries presenting as deep tissue injury.
- Deep tissue injury may be difficult to detect in individuals with dark skin tones.
- Deep Tissue Injury (DTI), although closed (intact skin), would not be considered healed.
- A pressure ulcer/injury presenting with characteristics of a DTI is reported as a DTI unless full thickness tissue loss is present. For example, a DTI presenting as purple localized discoloration with tenderness caused by pressure, but without full thickness tissue loss would be coded as a DTI, even though the wound is not completely intact.
Determining “Present at the most recent SOC/ROC” to answer M1311 fields ending in 2 (M1311X2, where X is A-F)
For each pressure ulcer/injury observed and reported in items M1311A1-F1 on Discharge, determine whether that pressure ulcer/injury was observed at the same stage at the time of the most recent SOC/ROC, and did not form during this home health quality episode.
- If the patient has a pressure ulcer that was documented at SOC/ROC and at discharge is documented at the same stage, it would be considered as “present at the most recent SOC/ROC”, even if during the episode the original pressure ulcer healed and reopened.
- If the pressure ulcer/injury was unstageable at SOC/ROC, but becomes numerically stageable later, when completing the Discharge assessment, its “Present at the most recent SOC/ROC” stage should be considered the stage at which it first becomes numerically stageable.
- If it subsequently increases in numerical stage, do not report the higher stage ulcer as being “present at the most recent SOC/ROC” when completing the Discharge assessment.
- For instance, a PU/PI was unstageable at SOC/ROC, then it became numerically stageable as a Stage 3, but then progressed to Stage 4 during the same episode of care. When completing the Discharge assessment, its “Present at the most recent SOC/ROC” stage would be Stage 3 and not Stage 4
- Unstageable Ulcers: Slough/Eschar (M1311E2)
- M1311E2: Any numerically stageable pressure ulcer/injury observed at SOC/ROC that is unstageable due to slough and/or eschar at discharge, should be considered new, and not coded as “present at the most recent SOC/ROC” for M1311E2.
- Unstageable Ulcers/Injury: Non-removable dressing/device (M1311D2)
- If an unknown pressure ulcer/injury is discovered upon removal of a non-removable dressing/device, that pressure ulcer/injury should be considered new, and not be coded as “present at the most recent SOC/ROC” for M1311X2.
- If a pressure ulcer/injury that is stageable at SOC is unstageable due to a non-removable dressing/device at discharge, it would be considered “present at the most recent SOC/ROC” if it had NOT:
- increased in numerical stage, or
- become unstageable due to slough/eschar when the non-removable dressing/device was applied. This is because even though the stage of the pressure ulcer/injury is unknown at discharge, there is no documentation or indication that it increased in numerical stage or worsened during the stay.
- Unstageable: Deep Tissue Injury (DTI) (M1311F2)
- A deep tissue injury with intact skin at SOC/ROC, that becomes stageable, is considered “present at the most recent SOC/ROC” at the stage at which it first becomes numerically stageable.
- If a DTI that was observed at SOC/ROC does not evolve to be numerically stageable, but is subsequently classified as another type of unstageable pressure ulcer/injury, it would be considered and coded as “present at the most recent SOC/ROC” on the discharge assessment in that unstageable pressure ulcer/injury category (M1311X1=1 and M1311X2=1).
Coding Instructions
- At SOC/ROC, enter a response for the following rows of this item: A1, B1, C1, D1, E1, and F1.
- Example: At SOC, in B1, enter the number of Stage 3 pressure ulcers that are observed at the first skin assessment completed during the SOC assessment timeframe. Enter 0 if no Stage 3 pressure ulcers are observed.
- Dash is not a valid response for this item at the SOC/ROC time points.
- At Discharge, enter a response for each row of this item: A1, A2, B1, B2, C1, C2, D1, D2, E1, E2, F1, and F2, unless directed to skip.
- Example: At Discharge, in A1 enter the number of Stage 2 pressure ulcers that are observed at the discharge assessment. If no Stage 2 pressure ulcers are observed, enter “0” in A1, and skip A2. If at least one Stage 2 pressure ulcer is observed and reported in A1, enter in A2 the number of these Stage 2 pressure ulcers that were observed at the same stage at the most recent SOC/ROC.
- Dash is a valid response for this item at the discharge time point.
- Dash indicates “no information.” CMS expects dash use to be a rare occurrence.
Coding Tips
- Any type of flap procedure performed to surgically replace a pressure ulcer is reported as a surgical wound, until healed. It should not be reported as a pressure ulcer/injury on M1311.
- A pressure ulcer treated with any type of graft is no longer reported as a pressure ulcer/injury, and until healed, should be reported as a surgical wound on M1340.
- A pressure ulcer that has been surgically debrided remains a pressure ulcer and should not be reported as a surgical wound on M1340.
Examples - Identify “Present at the most recent SOC/ROC” to answer M1311 at Discharge
1. Deep Tissue Injury (DTI) with intact skin at a SOC assessment becomes numerically Stageable
- The RN assesses a patient’s skin at the SOC and identifies a DTI with intact skin on the patient’s left heel. This DTI remains unchanged until the RN skin assessment 10 days later, which reveals open skin presenting as a Stage 3 pressure ulcer. The pressure ulcer does not change for the remainder of the episode. At the discharge skin assessment, the ulcer remains a Stage 3. (In this example, there are no other pressure ulcers/injuries at the SOC assessment, during the episode or at discharge).
- Coding: On the discharge assessment:
- M1311B1, Number of Stage 3 pressure ulcers, would be coded “1”.
- M1311B2, Number of these Stage 3 pressure ulcers that were present at the most recent SOC/ROC would be coded “1”.
- M1311F1, Number of unstageable pressure injuries presenting as DTI, would be coded “0”. (Skip M1311F2).
- Rationale: At the discharge assessment, the patient had one Stage 3 pressure ulcer, and zero unstageable pressure injuries presenting as DTI. The Stage 3 pressure ulcer observed on the discharge skin assessment is reported “present at the most recent SOC/ROC” because that is the stage at which the DTI observed at the SOC assessment first became numerically stageable.
2. Deep tissue injury (DTI) with intact skin at SOC, becomes numerically stageable and increases in numerical stage by discharge.
- The RN completes a skin assessment during the SOC visit for a patient and identifies a right hip DTI with intact skin. This DTI is first numerically stageable 10 days later as a Stage 3 pressure ulcer and increases in numerical stage five days after that, to a Stage 4 pressure ulcer. The pressure ulcer remains a Stage 4 at discharge.
- Coding: On the DC discharge assessment:
- M1311C1, Number of Stage 4 pressure ulcers, would be coded “1”.
- M1311C2, Number of these Stage 4 pressure ulcers that were present at the most recent SOC/ROC, would be coded “0”.
- M1311F1, unstageable pressure injuries presenting as DTI, would be coded “0”. (Skip M1311F2).
- Rationale: The DTI with intact skin observed on the SOC skin assessment first became numerically stageable as a Stage 3. Because the Stage 3 pressure ulcer increased in numerical stage to a Stage 4 by the discharge assessment, the Stage 4 pressure ulcer at discharge is considered new, and not coded as present at the most recent SOC/ROC.
3. Deep Tissue Injury (DTI) with intact skin at SOC, becomes numerically stageable, then is
unstageable due to slough and/or eschar at discharge.- The RN assesses a patient’s skin during the assessment timeframe for the SOC and identifies a DTI with intact skin on the patient’s right heel. This DTI first becomes numerically stageable at the third home visit, as a Stage 3 pressure ulcer. At the discharge skin assessment, this pressure ulcer is unstageable due to slough and eschar.
- Coding: On the discharge assessment:
- M1311E1, number of unstageable pressure ulcers due to slough and/or eschar, would be coded “1”.
- M1311E2, number of these unstageable pressure ulcers that were present at the most recent SOC/ROC, would be coded “0”.
- M1311F1, unstageable pressure injuries presenting as DTI, would be coded “0”. (Skip M1311F2).
- Rationale: The DTI with intact skin observed on the SOC skin assessment first became stageable as a Stage 3 pressure ulcer. This ulcer did not remain a Stage 3, however. At the discharge skin assessment the ulcer was unstageable due to slough and eschar. Any pressure ulcer/injury that is unstageable due to slough and/or eschar at discharge, but was previously numerically stageable, is considered new, and not coded as present at the most recent SOC/ROC
M1322: Current Number of Stage 1 Pressure Injuries
Item Intent
- Identifies the presence and number of Stage 1 pressure injuries.
Item Rationale
- Stage 1 pressure injuries may deteriorate to more severe pressure ulcers/injuries without adequate intervention; as such, they are an important risk factor for further tissue damage.
- Development of a Stage 1 pressure injury is one of multiple factors that should lead providers to initiate pressure ulcer/injury prevention interventions.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
Response-Specific Instructions
- Recognize that although Stage 1 pressure injuries are closed (intact skin), they would not be considered healed.
Coding Instructions
- Enter the number of Stage 1 pressure injuries present at the first skin assessment completed at the SOC/ROC.
- Dash is not a valid response for this item
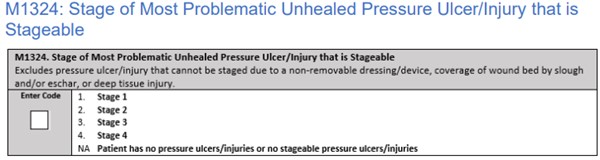
M1324: Stage of Most Problematic Unhealed Pressure Ulcer/Injury that is Stageable
Item Intent
- Identifies the stage of the most problematic unhealed stageable pressure ulcer/injury.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
- Discharge from agency
Coding Instructions
- Enter the response that most accurately describes the stage of the most problematic unhealed stageable pressure ulcer/injury.
- Step 1: Determine which pressure ulcer(s)/injur(ies) are stageable or unstageable. Definitions of pressure ulcer/injury stages are in guidance for M1311, Current Number of Unhealed Pressure Ulcers/Injuries. A pressure ulcer/injury is considered unstageable if:
- It is covered with a non-removable dressing/device, such as a cast, that cannot be removed.
- The wound bed is obscured by some degree of necrotic tissue AND no bone, muscle, tendon, or joint capsule (Stage 4 structures) are visible.
- Note that if a Stage 4 structure is visible, the pressure ulcer is reportable as a Stage 4 even if slough or eschar is present.
- It presents as a deep tissue injury
- Step 2: Determine which stageable pressure ulcer/injury is the most problematic.
- “Most problematic” may be the largest, the most advanced stage, the most difficult to access for treatment, the most difficult to relieve pressure, etc., depending on the specific situation.
- If the patient has only one stageable pressure ulcer, then that ulcer is the most problematic.
- Enter “NA” if the patient has NO pressure ulcers or only has pressure ulcers that are unstageable at the time of the assessment.
- Stage 1 pressure injuries, although closed (intact skin), would not be considered healed.
- Dash is not a valid response for this item.
Coding Tips
- Pressure ulcers/injuries that have healed are not considered for this item.
- Do not reverse stage pressure ulcers as a way to document healing as it does not accurately characterize what is physiologically occurring as the ulcer heals. For example, over time, even though a Stage 4 pressure ulcer has been healing and contracting such that it is less deep, wide, and long, the tissues that were lost (muscle, fat, dermis) will never be replaced with the same type of tissue. Unless it becomes unstageable, clinical standards require that a Stage 4 pressure ulcer continue to be documented as a Stage 4 pressure ulcer until it has healed.
- If a pressure ulcer is Stage 4 at SOC and is granulating at the next assessment, the ulcer remains a Stage 4 ulcer.
Stasis Ulcer (Venous Leg Ulcer)
This section summarizes CMS OASIS Instructions related to stasis ulcer (also known as venous leg ulcer or VLU). For an introduction and assessment of stasis ulcer including epidemiology, risk factors, etiology, pathophysiology, history, physical examination, diagnosis, differential diagnoses, documentation and ICD-10 coding, see "Venous ulcers - Introduction and Assessment".
If not sure the wound fits the definition of a stasis ulcer, the clinician should contact the physician for clarification.
M1330: Does this patient have a Stasis Ulcer?

Item Intent
- Identifies patients with ulcers caused by inadequate venous circulation in the area affected (usually lower legs).
- This lesion is often associated with stasis dermatitis.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
- Discharge from agency
Response-Specific Instructions
- Physical assessment and observation are the preferred approach to determine the presence of stasis ulcers. Patient/caregiver report, medical records including physician/allowed practitioner orders and input may be used.
- It is important to differentiate stasis ulcers from other types of skin lesions, and only report stasis ulcers in this item.
- Stasis ulcers DO NOT include arterial lesions or arterial ulcers.
- Once a stasis ulcer has completely epithelialized, it is considered healed and should not be reported as a current stasis ulcer.
- Unobservable stasis ulcers are reported stasis ulcer(s) that cannot be observed because of a dressing or device, such as a cast or Unna boot that cannot be removed. Information may be obtained from the physician or patient/caregiver regarding the presence of a stasis ulcer underneath the cast or dressing.
Coding Instructions
- Code 1, Yes, if patient has BOTH observable and unobservable stasis ulcers.
- Code 2, Yes, if the patient has observable stasis ulcers ONLY.
- Code 3, Yes, if the patient has unobservable stasis ulcers ONLY.
- Dash is not a valid response for this item
M1332: Current Number of Stasis Ulcer(s) that are Observable

Item Intent
- Identifies the number of visible (observable) stasis ulcers.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
Response-Specific Instructions
- Physical assessment and observation are the preferred approach to determine the presence of stasis ulcers. Patient/caregiver report, medical records including physician/allowed practitioner orders and input may be used.
- All stasis ulcers except those that are covered by a non-removable dressing/device, such as a cast or Unna boot, are considered observable.
- Dash is not a valid response for this item
M1334: Status of Most Problematic Stasis Ulcer that is Observable

Item Intent
- Identifies the degree of healing present in the most problematic, observable stasis ulcer.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
- Discharge from agency
Response-Specific Instructions
- Physical assessment and observation are the preferred approach to determine the presence of stasis ulcers. Patient/caregiver report, medical records, including physician/allowed practitioner orders and input may be used.
- Determine which stasis ulcers are observable. Include all stasis ulcers that are not covered with a nonremovable dressing/device, such as a cast or Unna boot.
- If the patient has only one observable stasis ulcer, that ulcer is the most problematic.
- “Most problematic” is determined by the clinician’s professional evaluation of the individual’s overall wound status, and may be based on factors including, but not limited to:
- Healing status, such as an ulcer that is infected or resistant to treatment
- Size (may be the largest ulcer)
- Location (may be difficult to access for treatment)
- Once a stasis ulcer has completely epithelialized and is without signs/symptoms of infection, it is considered healed and should not be reported as a current stasis ulcer.
Coding Instructions
- Code 1, Fully Granulating, when the stasis ulcer wound bed:
- is filled with granulation tissue to the level of the surrounding skin or new epithelium;
- has no dead space;
- has no avascular tissue;
- has no signs or symptoms of infection; and,
- has open wound edges.
- Code 2, Early/Partial Granulation, when:
- ≥ 25% of the wound bed is covered with granulation tissue;
- there is minimal avascular tissue (that is, <25% of the wound bed is covered with avascular tissue);
- may have dead space;
- has no signs or symptoms of infection; and,
- has open wound edges.
- Code 3, Not Healing, when:
- ≥25% of the wound bed is avascular tissue – AND/OR
- signs/symptoms of infection are present – AND/OR
- the wound bed is clean but non-granulating – AND/OR
- the wound edges are closed/hyperkeratotic – AND/OR
- there is persistent failure to improve despite appropriate comprehensive wound management.
- Dash is not a valid response for this item
Surgical wounds
This section summarizes CMS OASIS Instructions related to surgical wounds. For an introduction and assessment of surgical wounds complications including epidemiology, risk factors, etiology, pathophysiology, history, physical examination, diagnosis, differential diagnoses, documentation and ICD-10 coding, see topic "Surgical Wound Complications". For a background on ostomy, watch video "Ostomy Care Basics".
M1340: Does this patient have a Surgical Wound?

Item Intent
- Identifies the presence of a wound resulting from a surgical procedure.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
- Discharge from agency
Response-Specific Instructions
- Physical assessment and observation are the preferred approach to determine the presence of surgical wounds. Patient/caregiver report, medical records, including physician/allowed practitioner orders and input may be used.
- The agency may use any skin assessment conducted during the assessment timeframe to code M1340.
- For the purpose of this OASIS item, a surgical site closed primarily (with sutures, staples, or a chemical bonding agent) is generally described in documentation as a surgical wound until re-epithelialization has been present for approximately 30 days, unless it dehisces or presents signs of infection. After 30 days, it is generally described as a scar and should not be included in this item.
- Old surgical wounds that have resulted in scar or keloid formation are not considered current surgical wounds and should not be included in this item.
- An incision line is considered a surgical wound. The staple or suture sites are not considered surgical wounds.
Coding Instructions
- Code 1, Yes, patient has at least one observable surgical wound, if the patient has at least one observable surgical wound
- If the patient has both an observable surgical wound, and a known but not observable surgical wound, Code 1, Yes.
- Code 2, Surgical wound known but not observable if the only surgical wound is not observable.A surgical wound is considered not observable when it is covered by a dressing/device, such as a cast, which is not to be removed per physician order.
- Dash is not a valid response for this item.
Coding Tips
- If a pressure ulcer is surgically closed with a flap or graft it is no longer reported as a pressure ulcer. It should be reported as a surgical wound until healed. If the flap or graft fails, it should continue to be considered a surgical wound until healed.
- A bowel ostomy is excluded as a surgical wound, unless a "take-down" procedure of a previous bowel ostomy is performed, in which case the surgical take-down produces a surgical wound. A bowel ostomy being allowed to close on its own is excluded as a surgical wound.
- All other ostomies are excluded from consideration under this item and should not be counted as surgical wounds.
- There are many types of "ostomies," all of which involve a surgically formed opening from outside the body to an internal organ or cavity. Examples include cystostomy, urostomy, thoracostomy, tracheostomy, gastrostomy, etc.
- Other examples of surgical wounds include, but are not limited to:
- Orthopedic pin sites,
- Central line sites (centrally inserted venous catheters),
- Wounds with drains,
- Medi-port sites and other implanted infusion devices, or
- Venous access devices
- A PICC line (peripherally inserted venous catheter), either tunneled or non-tunneled, is NOT a surgical wound, when it is peripherally inserted.
- Cataract surgery of the eye, surgery to the mucosal membranes, or a gynecological surgical procedure via a vaginal approach do NOT create a surgical wound for the purpose of this item
M1342: Status of Most Problematic Surgical Wound that is Observable

Item Intent
- Identifies the degree of healing present in the most problematic, observable surgical wound.
Time Points Item(s) Completed
- Start of Care
- Resumption of Care
- Discharge from agency
Response-Specific Instructions
- Physical assessment and observation are the preferred approach to determine the presence of surgical wounds. Patient/caregiver report, medical records, including physician/allowed practitioner orders and input may be used.
- Determine which surgical wounds (as defined in M1340 guidance) are observable.
- Identify the most problematic observable surgical wound.
- If the patient has only one observable surgical wound, that wound is the most problematic.
- “Most problematic” is determined by the clinician’s professional evaluation of the individual’s overall wound status, and may be based on factors including, but not limited to:
- Healing status, such as a surgical wound that is infected or resistant to treatment
- Size (may be the largest surgical wound)
- Location (may be difficult to access for treatment)
- Surgical Wound Assessment
- The clinician must first assess if the wound is healing entirely by primary intention (well-approximated with no dehiscence), or if there is a portion healing by secondary intention, (due to dehiscence, interruption of the incision, or intentional secondary healing). For surgical wounds healing by primary intention, observe if the incision line has re-epithelialized.
- Surgical wounds healing by primary intention (approximated incisions) do not granulate; therefore, the only appropriate responses are Response 0 – “Newly epithelialized” or Response 3 – “Not healing”
- A surgical incision is not automatically coded Response 3 – “Not healing” solely due to the presence of staples.
- For a surgical wound healing by primary intention, if there is not full re-epithelialization, such as in the case of a scab adhering to underlying tissue, the correct response is Response 3 – “Not healing” Surgical wounds with incisional separation heal by secondary intention.
- Surgical incisions healing by secondary intention do granulate; therefore, in addition to meeting the definition for 0 – Newly epithelialized or 3 – Not healing, these secondary intention wounds may also fit the definitions for Response 1 – “Fully granulating” or Response 2 – “Early, partial granulation” if appropriate.
- If complete epidermal resurfacing of a surgical wound has occurred, the correct response is Response 0 - "Newly epithelialized" until approximately 30 days have passed without complication, at which time it is no longer a reportable surgical wound.
Coding Instructions
- Code 0, Newly epithelialized, when:
- the wound bed is completely covered with new epithelium; no exudate; no avascular tissue (eschar and/or slough); no signs or symptoms of infection.
- the incision site of an implanted venous access device or infusion device is healed and without signs and symptoms of infection.
- Code 1, Fully granulating, when:
- the wound bed is filled with granulation tissue to the level of the surrounding skin and
- has no dead space,
- has no avascular tissue;
- has no signs or symptoms of infection;
- has open wound edges.
- Code 2, Early/partial granulation, when:
- ≥25% of the wound bed is covered with granulation tissue;
- < 25% of the wound bed is covered with avascular tissue,
- may have dead space; and
- wound bed has no signs or symptoms of infection;
- wound has open edges.
- Code 3, Not healing, when:
- The wound bed has ≥25% avascular tissue – AND/OR
- signs/symptoms of infection – AND/OR
- the wound bed is clean but non-granulating – AND/OR
- wound edges are closed/hyperkeratotic – AND/OR
- persistent failure to improve despite appropriate comprehensive wound management.
- Dash is not a valid response for this item.