ABSTRACT
Venous Leg Ulcers (VLU) are relatively common, affecting 1% of the population in the U.S.[1] VLU can be defined as an open skin lesion of the leg or foot that occurs in an area affected by venous hypertension, often caused by chronic venous insufficiency.[2] It is a chronic condition, with recurrence rate within 3 months after wound closure as high as 70%.[1] Thirty-five percent of people with VLU experience four or more episodes.[3][4]
For VLU management including a section for clinicians on patient education, see "Venous ulcers - Treatment and Prevention". For clinical guidelines and quality measures specific to VLU, see "Venous Ulcers - Overview".
Assessment: See Algorithm for Assessment of Venous Ulcers
History: A complete assessment of the patient, performed by a qualified multidisciplinary team, includes identification of risk factors for chronic venous insufficiency (CVI), development of VLU, VLU recurrence and delayed healing. Patient's concerns and psychosocial status should also be assessed.
Physical Examination: Signs of chronic venous disease include active or healed ulcers, varicosities, telangiectasia, varicose veins, edema, etc. VLUs generally develop in the gaiter area, between mid-calf and approximately 1 inch below the malleolus [5]. VLUs can be superficial to deep and generally have irregular margins, wound bed with fibrin and granulation tissue, and moderate to heavy exudate.
Diagnosis: Predominantly clinical, but peripheral arterial disease (PAD) needs to be ruled out with evaluation of ankle brachial index (ABI) ratio, audible handheld Doppler ultrasound with continuous waveform analysis or other noninvasive arterial tests. An ABI <0.9 indicates an ischemic component. Venous disease is objectively documented with duplex ultrasound. Other tests can be ordered when necessary
Differential diagnosis: Arterial ulcers, neuropathic ulcers, pressure ulcers are among the most common differential diagnoses.
Characterization of VLUs: After differential diagnoses are ruled out and etiology is established, expert consensus recommends categorizing VLUs as "simple", "complex" or of "mixed etiology" to determine likely prognosis, so that appropriate timeframes for monitoring, reassessment and specialist referral can be established [6]
Ulcer healability: Classification according to potential to heal with conservative management only is helpful in determining an adequate treatment plan. Ulcers that can be healed with conservative management only are categorized as "healable", ulcers that are likely not going to heal with conservative management only are "non-healable" and if co-existing medical conditions, drugs or circumstances will likely impede wound healing, ulcers are classified as "maintenance". See topic "How to Determine Healability of a Chronic Wound"
Documentation: To be done at least weekly to assess wound healing progress. Proper documentation includes number and position of ulcers on the leg, wound measurements including area, perimeter, and depth, description of wound edge, peri-wound area, wound base quality, amount and type of drainage, and infection, history of debridement. Signs of VLU improvement need to be documented to support medical necessity (as per Medicare requirements). As part of a patient-centered approach, it is recommended that clinicians adopt patient-reported outcome measures to assess patient’s Quality of Life (QOL), pain, and depression. [7]
Treatment: see "Venous ulcers - Treatment and Prevention"
Patient Education: see "Venous ulcers - Treatment and Prevention"
When to refer to specialists:
- Specialized service/clinic that manages VLU (e.g., wound clinic), if initially treated elsewhere: "Complex" VLUs and "mixed etiology" leg ulcers, atypical presentation, pressure ulcer/injury. To facilitate referral and transition of care, use the "Provider Wound Communication Tool"
- Vascular surgeon: Abnormal ankle brachial index ratio, duplex ultrasound results with any indications for vascular surgery, peripheral artery disease, critical limb ischemia
- Emergency department: Acute limb ischemia, sepsis, necrotising fasciitis
- Nutritionist at initial evaluation
- Respective specialists if associated dermatological, metabolic, hematologic, autoimmune, oncologic diseases are suspected
- Plastic surgeon for surgical wound coverage procedures
- Hospice if the patient is certified as terminally ill (prognosis of 6 months or less) by their attending provider (if they have one) and the hospice provider.[8]
- See details in Table "Pressure levels and management of simple, complex and mixed VLU' in topic "Venous Ulcers - Treatment and Prevention"
ICD-10 Coding
First select ICD-10 for underlying pathology:
- Chronic venous hypertension with ulcer (I87.31-, I87.33-)
- Post-phlebitic syndrome with ulcer (I87.01-, I87.03-)
- Post-thrombotic syndrome with ulcer (I87.01-, I87.03-)
- Varicose ulcer (I83.0-, I.83.2-)
Then for VLU severity:
- Non-pressure chronic ulcer of the calf (L.97.2-)
Clinical guidelines and Quality Measures: see "Venous Ulcers - Overview"
|
Algorithm for Assessment of Venous Ulcer | First Visit Checklist | Follow up Visit Checklist
|
INTRODUCTION
Overview
This topic covers the Introduction and Assessment of venous leg ulcers (VLU) including epidemiology, risk factors, etiology, pathophysiology, history, physical examination, diagnosis, differential diagnoses, documentation and ICD-10 coding. For VLU management including a section for clinicians on patient education, see "Venous ulcers - Treatment and Prevention". For clinical guidelines and quality measures specific to VLU, see "Venous Ulcers - Overview". For an overview of surgical interventions for management of chronic venous disease and resulting manifestations such as VLUs, see " Chronic Venous Disease - Surgical Management".
Background
Venous disease is a chronic condition that can be characterized by periods of ulceration (i.e. an open wound) followed by healing and then recurrence.[9] Patients with chronic venous disease (CVD) of the lower extremities may present with many different clinical features, ranging from reticular veins, telangiectasias, varicose veins, edema, skin pigmentation, lipodermatosclerosis, and atrophie blanche, to venous ulceration. [10][11] Venous Leg Ulcers (VLUs) are a relatively common, complex type of wound that have a negative impact on people’s lives and incur high costs for health services.[12]
Definitions
- Venous leg ulcers: VLU can be defined as an open skin lesion of the leg or foot that occurs in an area affected by venous hypertension.[2] VLUs can result in pain, unpleasant odor, reduced mobility, sleep disturbance, reduced psychological well-being and social isolation.[12] In severe cases and when associated with arterial insufficiency, VLUs can lead to limb amputation.[13][14]
- Chronic venous disease: the term chronic venous disease (CVD) has been defined as “(any) morphological and functional abnormalities of the venous system of long duration manifest either by symptoms and/or signs indicating the need for investigation and/or care”. [15][16]
- Chronic venous insufficiency: the term “chronic venous insufficiency” (CVI) is reserved for advanced CVD, which is applied to functional abnormalities of the venous system, producing edema, skin changes, or venous ulcers, corresponding with C3 to C6 of the CEAP classification. [15] See section 'CEAP Classification System' below.
Relevance of VLUs
- Venous ulcers are often recurrent:
- The recurrence rate within 3 months after wound closure is as high as 70%.[1] Thirty-five percent of people with VLU experience four or more episodes during their life times.[3][4]
- Open ulcers can persist from weeks to many years:
- The first-line treatment for VLUs is compression therapy, but despite adequate compression up to 45% of people have unhealed ulcers after 6 months of treatment.[12][17] Since these figures were extracted from randomized controlled trials, the percentage of unhealed ulcers in the real world are probably higher.
- It is estimated that 93% of VLUs will heal in 12 months, and 7% remain unhealed after five years.
- Despite the relatively low prevalence, VLUs represent a significant financial burden to the healthcare system:
- In the U.S., the overall burden to Medicare and private insurers due to VLU is estimated to be around US$14.9 billion (in 2012 US$, excluding out-of-pocket payments and other indirect costs such as lost productivity).[18] Also, it has been reported that 4.6 million workdays per year are lost secondary to chronic venous insufficiency (CVI), in which VLUs are the most severe complication. [19]
- In the U.K., estimated costs to treat a person with open leg ulcer is around GBP 1700 (US$ 2122) per year at 2012 prices, mostly related to nurses' time.[20]
Epidemiology
Prevalence
- Prevalence of ulcers of venous etiology only the UK is about 2.9 cases per 10,000 people [12][21], whereas mixed arterial/venous leg ulcers have a prevalence of 1.1 per 10,000 people.[2]
- Approximately 1% of the population in the United States, 3% of people over 80 years of age in westernized countries. [1] Prevalence is increasing, coinciding with an aging population. [19] In the U.S., VLUs affect between 500,000 to 2 million people per year. [22]
- More prevalent among women, but this gender discrepancy decreases with age. [23]
- Most common type of leg ulcer (~ 80% of leg ulcers). [24]
Incidence
- The overall incidence rate is 0.76 (95% CI, 0.71, 0.83) for men and 1.42 (1.35, 1.48) per 100 person-years for women. [25]
Risk Factors
- Risk factors for development of VLU:
-
- Presence of chronic venous insufficiency (CVI): risk factors for CVI include older age, obesity, reduced mobility, previous leg injuries, deep venous thrombosis, phlebitis, low physical activity, prolonged standing or sitting, arterial hypertension, deep venous thrombosis, family history of VLU.[23][24][26][27][28]
- Genetic predisposition to early onset of varicose veins: Klippel-Trenaunay syndrome, CADASIL, FOXC2 gene mutation, desmulin dysregulation, and Ehlers-Danlos syndrome [27]
- Risk factors for delayed VLU healing:
-
- Initial VLU location, area and duration are the most important predictors [29]:
-
- VLU location in posterior ankle or back of calf region [7]
- VLU that is smaller than 10 cm2 and has a duration shorter than 12 months at first visit has a 70% change of healing by the 24th week of care, whereas a VLU larger than 10 cm2 and with a duration longer than 12 months has only 22% chance of healing by the 24th week of care [12][30].
- Other risk factors include [7]:
-
- > 50 years, male gender
- History of vascular surgery, trauma, repeat intimal venous damage or varicosities
- Family history of VLU
- BMI > 33 kg/m2 with documented nutritional deficiency
- Multiple pregnancy
-
Risk factors for recurrence [7][19]:
-
- Deep venous disease
- Deep venous thrombosis
Etiology
VLUs are the final stage of chronic venous insufficiency (CVI) and associated venous hypertension (increased ambulatory venous pressure).[12][27]
-
The term chronic venous disease is generally applied to the full spectrum of chronic venous disease (CEAP C0-6), whereas chronic venous insufficiency is reserved for more severe presentations (CEAP C4-6).[31] See section 'CEAP Classification System' below.
- It is not infrequent for leg ulcers to be associated with CVI and arterial vascular disease, in which case, these ulcers are said to be of “mixed etiology.”
Pathophysiology
- The pathophysiology of VLU is complex and healing is delayed in many patients due to a chronic inflammatory condition.[32] Patient risk factors predispose individuals to chronic venous diseases including VLU.
- CVI results in venous hypertension (ambulatory venous pressures of up to 60 to 90 mmHg, as opposed to the normal levels of 20 to 30 mmHg), which can happen due to obstruction to venous flow or venous reflux from dysfunction of venous valves, and/or failure of the "venous pump".[27][33] Reflux is much more prevalent among patients across the different stages of chronic venous disease (CVD), including VLUs. However, obstruction has a higher rate of patients who develop VLU and a much faster disease progression.[27]
- Venous hypertension and hemodynamic abnormalities caused by venous flow obstruction or venous reflux lead to inflammatory alterations with microcirculatory changes described below that can result in venous stasis and VLU (see Figure 1) [33][34]:
- Pooling of venous blood: valve dysfunction or venous obstruction leads to blood accumulation, heightening pressure against vein walls.
- Altered shear stress: increased pressure against vein walls changes the physiological shear stress, crucial for maintaining blood fluidity and preventing blood cell adherence.
- Endothelial damage: the resulting mechanical stress disrupts the endothelium's protective glycocalyx layer, leading to cell activation and increased permeability.
- Imbalance of inflammation, inflammatory modulators, oxidative stress, and proteinase activity: endothelial damage leads to activation of adhesion molecules on endothelial cells, leukocyte activation with attachment and migration into vein wall, microcirculation, and in the interstitial space. Multiple chemokines, cytokines, growth factors, proteases and matrix metalloproteinases are produced to target fibroblasts, vascular smooth muscle cells, and the extracellular matrix.[27][32]
- Skin changes: the increased permeability of endothelial cells allows red blood cells to escape, releasing hemoglobin and ferric iron into the interstitial fluid. This release contributes to increased oxidative stress and inflammation, leading to noticeable skin changes and progression of CVD. Skin changes include [35]:
- Eczema and pigmentation (CEAP stage C4a), which appear to be caused mainly by a hemosiderin deposit occurring in the early stages of CVD
- Chronic fibrosing panniculitis (inflammation of subcutaneous fat) related to CVI
- Lipodermatosclerosis (CEAP stage C4b), which eventually leads to the development of tissue breakdown and VLU.[36]
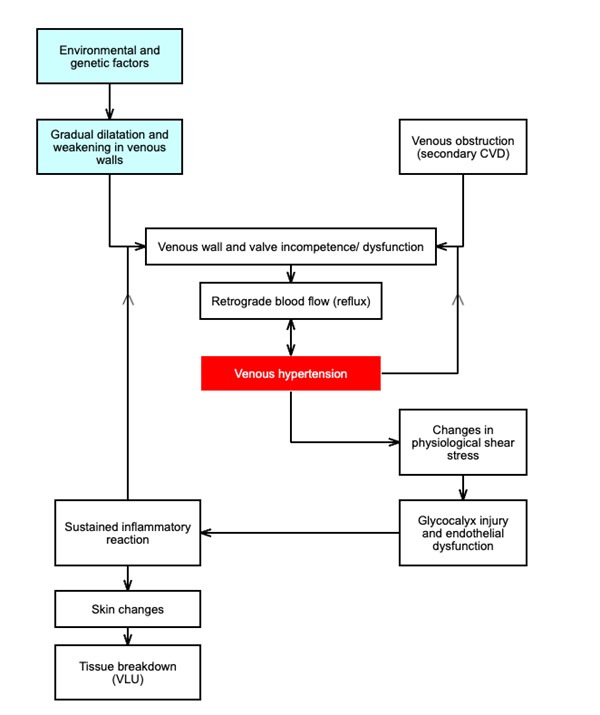
Figure 1. Pathophysiology of venous leg ulcers (adapted from Coelho et al.)[34]
ASSESSMENT
- Primary goals of assessment are:
-
- To identify risk factors for VLU, amputation, delayed healing, recurrence. See details in “Risk Factors”
- To assess patient's and caregiver's concerns
- To screen for significant signs and symptoms to differentiate from other types of lower extremity ulcers, which may require different treatments. See “Differential Diagnoses”
- To categorize VLUs as "simple", "complex" or of mixed etiology (i.e., due to venous disease and peripheral arterial disease) to determine likely prognosis, so that appropriate time frames for monitoring, reassessment and specialist referral can be established [6]
-
- Peripheral arterial disease (PAD) needs to be ruled out with noninvasive arterial tests and venous disease should be documented with duplex ultrasound. See section 'Diagnosis' below
- To determine "healability", that is, the potential of the ulcer to heal with conservative treatment only
-
-
See Algorithm for Assessment of Venous Ulcers below (Algorithm 1)
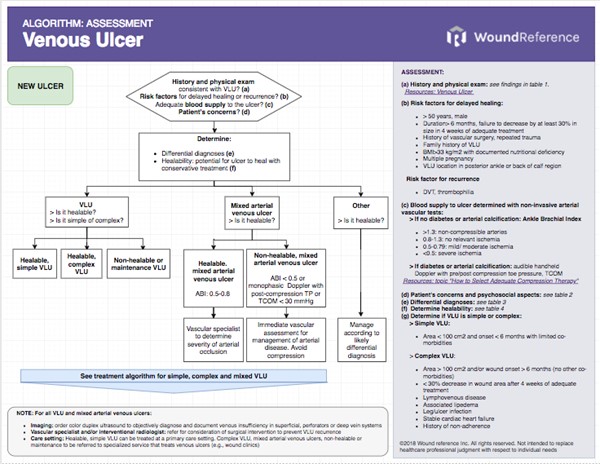
Algorithm 1. Algorithm for Assessment of New and Recurrent Venous Ulcer (click link to enlarge)
History
Qualified professional multidisciplinary team should evaluate and perform a complete assessment of the patient. Patients with VLU frequently present with other co-morbidities that may impede healing. It is important to obtain a comprehensive patient history of the patient’s current condition, recurrence and treatment if any, medical and surgical history including past deep vein thrombosis (DVT), pulmonary embolism or malignancy, medications, and other risk factors related to VLU, CVI or non-healing leg wounds.[2][37][38]
Chief Complaint and History of Present Illness
- Time of symptom onset and duration
- Symptoms experienced by patients with VLU include extremity pain, burning aching, throbbing, cramps, heaviness, itching, tiredness, fatigue, and restless legs.[2][24][37] Venous symptoms are usually exacerbated when the patient is standing and relieved by rest or limb elevation (as opposed to pain of peripheral artery disease, which worsens with walking or that is relieved by rest, or which worsens with limb elevation). Pain is localized to the affected veins, skin changes or ulcer and does not irradiate.
- Edema of lower extremities:
-
- History of medical condition resulting in edema of lower extremities, such as heart failure, hypothyroidism, hypoalbuminemia or nephrotic syndrome
- History of lymphatic disease resulting in edema of lower extremities. It is common for chronic venous disease to be associated with chronic lymphatic insufficiency, a condition known as phlebolymphedema. See topic "Lymphedema - Introduction and Assessment".
- Extremity swelling due to chronic venous disease can be present in 25-75% of patients, worsens with prolonged standing and improves with leg elevation and walking. In women, symptoms exacerbate with menses or pregnancy.
- History of complications, such as DVT, embolisms, skin infections, cellulitis, osteomyelitis, and malignant change.[24]
- Assess risk factors for development of VLU. See section ‘Risk factors’ above
- Past treatment history
- Comorbidities: autoimmune disorders, diabetes, immunosuppression and other conditions may delay healing.[39]
Medications
- Medications that delay wound healing (in case patient has an ulcer) include: anticoagulants, antimicrobials (various antibiotic classes), anti-angiogenesis agents (eg, bevacizumab, aflibercept), antineoplastic drugs, anti-rheumatoid drugs (eg, methotrexate, aspirin/nonsteroidal anti-inflammatory drugs [NSAIDs]), colchicine (anti-gout drug), topical hydrogen peroxide, topical iodine, full-strength 0.5% Dakin’s solution (sodium hypochlorite), nicotine, steroids, and vasoconstrictors.[40][41]
Social History
- Injectable drugs: repeated injections of illicit or not illicit drugs into the lower limb veins results in CVI. Increased risk for VLU persists even after prolonged periods free from injecting.[39][42]
Nutrition
- Clinical guidelines recommend nutritional assessment for patients with VLU [2][43][44], despite the relative low number of studies on nutritional supplementation on VLU healing. Poor nutrition may be a risk factor for delayed VLU healing.[45] Patients with VLUs are commonly overweight and also have a relative nutritional deficiency that needs to be addressed.[5][46]
-
- Standardized tools such as the "Nestlé MNA" and "Self-MNA®" by Nestlé can be used
- Medicare Quality Payment Program, Quality Measure:
-
- "Process Measure: Nutritional Screening and Intervention Plan in Patients with Chronic Wounds and Ulcers"
- "Patient Reported Nutritional Assessment and Intervention Plan in Patients with Wounds and Ulcers"
- "Preventative Care and Screening: Body Mass Index (BMI) Screening and Follow-Up"
Patient's and caregivers' concerns
- Patient's and caregiver's concerns and psychosocial aspects should be assessed and taken in consideration when creating a treatment plan:
-
- Evaluate patient's concerns: pain, exudate, odor, ability to carry out daily activities
-
- Medicare Quality Payment Program, Quality Measure: "Pain Assessment and Follow-Up"
- Evaluate psychosocial aspects of the patient, caregiver and family: cognitive, functional, emotional status, understanding of the wound and risk factors, preference for treatment, motivation for adherence to the care plan, financial concerns
- We recommend use of Patient-Reported Outcome Tools to assess aspects above and measure impact of interventions. See 'Patient-reported outcomes (PRO) tools' below.
Physical Examination
VLUs commonly present in between area mid-calf and approximately 1 inch below the malleolus.[5] The recurrence of an ulcer in the same area is highly suggestive of venous ulcer.[24] Physical examination of lower extremities should include [2]:
Inspection
- See Figures 1-9
- Limb shape and size (abnormal shape or large limbs can lead to challenges in compression therapy)
- Presence of active or healed ulcers, varicosities, telangiectasia, varicose veins, edema
- Chronic venous skin changes and dermatitis, such as skin discoloration, inflammation, eczema, hyperpigmentation, malleolar flair, corona phlebectatica (venous starburst of veins radiating distally from the medial malleolus), atrophie blanche (capillaries are virtually absent in areas of fibrotic scars, also known as livedoid vasculopathy), lipodermatosclerosis (severe fibrosing panniculitis of the subcutaneous tissue, area of indurated inflammatory tissue that binds the skin down to the subcutaneous tissue)
- Signs of infection, cellulitis
Palpation
-
- Varicosity, palpable venous cord, tenderness, sensation, induration
- Edema
- Peripheral pulses. See section 'Palpation' in topic "Arterial Ulcers - Introduction and Assessment".
- Percussion (or tap) test: this exam evaluates the functional status of valves in the superficial venous system. The test can be performed with or without a Doppler.
- Test: With the patient standing, place fingers of one hand on the saphenous vein. With fingers of the other hand, tap the saphenous vein about 15-20 cm proximally to the fingers previously placed on the saphenous vein.
- Abnormal test: distally placed fingers feel a pulsatile wave as the saphenous vein is proximally tapped, which indicates that valves between the 2 points are incompetent, and thus allow for the wave to travel distally.
- Normal test: the distally placed fingers should not feel any waves or oscillatory signals
- Trendelenburg test: this test measures how long it takes to refill the distal superficial veins on the dorsum of the foot. The goal is to assess valvular competency of the superficial, perforator and deep veins.
- Test: With the patient supine, raise one leg for 60 seconds, then apply a tourniquet around the proximal thigh. Have the patient stand up and observe any filling of the veins of the dorsum of the foot. Release the tourniquet.
- Abnormal test: if veins are immediately filled, the perforator system is incompetent. If veins are filled after the tourniquet is removed, incompetence of the superficial veins are likely.
- Normal: no filling is observed while the tourniquet is on or immediately after it is removed.
Auscultation
Other assessment
- Evaluation of ankle mobility: bony ankylosis and fibrosis may result in los off ankle function
- Assessment of foot temperature, measurement of the ankle brachial pressure index, testing for peripheral neuropathy, to look for signs of associated diseases such as arterial disease or diabetes mellitus.[5]

Figure 2. Atrophie blanche and livedoid vasculopathy
Ulcer Exam
-
Wound assessment: location, number and size of ulcers, edges, undermining, presence and type of nonviable tissue, signs of infection or biofilm, exudate type and quantity, periwound appearance (e.g., altered perfusion, maceration), edema.[39][47]
- Common VLU characteristics:
-
- Anatomic location: often at the medial distal lower extremity and ankle, at the malleolar area
- Margins: irregular
- Depth: superficial-to-deep
- Wound bed: granulation tissue and fibrin often present, minimal to moderate aching pain at borders and middle of the wound bed
- Exudate: frequent, moderate to heavy.
-
- "Wet leg syndrome": occurs when large quantities of exudate exude from lower extremities, increasing risk for skin maceration, infection and wound chronicity.[39] Often seen in phlebolymphedema. See topic "Lymphedema - Introduction and Assessment".
|

Figure 3. Venous ulcer and stasis
dermatitis on right lower leg
|

Figure 4. Superficial venous ulcer
with irregular margins
|
|

Figure 5. Venous ulcers on right and left lower extremities
|

Figure 6. Venous ulcer: indurated margins,
red granulation tissue
|
|

Figure 7. Highly exudative venous ulcer
with fibrin tissue
|

Figure 8. Venous stasis
|
|
![]()
Figure 9. Refractory VLU (<30% decrease in size after 4 weeks of care)
|
![]()
Figure 10. Legs with abnormal shape (inverted champaigne bottle) and venous stasis
|
Ulcer Complications
SOFT TISSUE INFECTION
- Specific findings that may indicate that a venous leg ulcer is infected include [48]:
- Ulcer area of 10cm2 or larger
- Presence of wound bed slough
- Increased wound exudate
- Depression, chronic pulmonary disease and anticoagulant use are predictors of wound infection
- The following mnemonics can help identify superficial and deep infections [49][50][51]:
- Superficial infection: The NERDS mnemonic can help identify soft tissue infection. If any 3 NERDS are present, superficial soft tissue infection is likely and topical antimicrobial treatment is justified. For mixed venous-arterial ulcers with superficial infection, topical antimicrobials alone may not be sufficient and systemic antibiotics may be needed.[52][53] NERDS stands for:
- Nonhealing ulcer
- increased Exudate
- Red-friable tissue
- Debris
- Smell
- Deep and surrounding infections: The STONEES mnemonic can help identify deep and surrounding infections. Systemic antibiotics and topical antimicrobial treatment are justified if 3 or more of the STONEES signs are present. STONEES stands for:
- increased Size,
- elevated Temperature of 3° F over a mirror image of the surrounding wound skin
- Os (latin for bone): probing to bone
- New breakdown or satellite areas of involvement,
- increased Exudate
- Erythema + edema (cellulitis)
- Smell
- Diagnosis is mainly clinical. Tissue biopsy or quantitative, validated swab cultures (e.g. Levine technique), or biofluorescent scans may be used to confirm diagnosis of infection. [48] For details on the wound infection continuum and associated signs and symptoms, see section see section 'Relevance' in topic "Wound Culture - Swabs, Biopsies, Needle Aspiration'. Tissue biopsy or quantitative, validated swab cultures (e.g. Levine technique), or biofluorescent scans may be used to confirm diagnosis of infection. See topics "Wound Culture - Swabs, Biopsies, Needle Aspiration", "How to Collect a Wound Swab (Levine Technique) for Culture" and "How to Perform a Wound Biopsy".
Diagnosis
The diagnosis of VLU is predominantly clinical. Clinical assessment for the assessment of chronic venous disease is very important because diagnostic testing results and symptoms do not always correlate.[54] However, peripheral arterial disease (PAD) needs to be ruled out with noninvasive arterial tests and venous disease should be documented with duplex ultrasound. PAD can be present in up to 25% of VLU patients [3][4] and its presence affects how compression therapy, one of the main interventions to manage VLUs, is implemented. Prior to application of compression therapy, presence of other ulcer etiologies and/or co-morbid conditions that affect how compression is applied should be carefully evaluated. Failure to do so can result in adverse effects and deterioration of the patient's condition. PAD may be ruled out with evaluation of ankle brachial index ratio (ABI); for patients with diabetes or arterial calcification, audible handheld Doppler ultrasound with continuous waveform analysis is preferred. Additional tests can be ordered when necessary, as illustrated in Table 1 below. See section on 'Algorithms' in topic "How to Select Adequate Compression Therapy Pressure Levels and Products". See types and brands of noninvasive arterial testing devices in topic "Assessment and Documentation".
Table 1. Summary of functional/diagnostic tests for patients with venous leg ulcers
| Functional/diagnostic tests for patients with venous leg ulcers by indications |
For all patients with suspected venous leg ulcers [19]: - To assess for adequate blood flow to promote ulcer healing, and to rule out PAD: palpation of lower-extremity arterial pulses and calculated ABI are recommended.[19] Audible handheld Doppler ultrasound with continuous waveform analysis, toe pressure, transcutaneous oxygen pressure (TCOM, TcPO2) are preferable for patients with diabetes or arterial calcification (See Table 2)
- To assess venous reflux and/or obstruction and confirm diagnosis of VLU: comprehensive duplex ultrasound is recommended [19]
For patients with recalcitrant VLUs (i.e., VLUs that fail to show signs of improvement within 4 weeks of adequate standard therapy) [19] - Biopsy (see topic "How to Perform a Wound Biopsy")
- Referral to a subspecialist
- Venous plethysmography for routine initial evaluation of VLU is discouraged unless results of venous duplex ultrasound are inconclusive, or if patient has recurrent or recalcitrant VLU [2].
- Laboratory evaluation for thrombophilia for patients with a history of recurrent or recalcitrant VLU or thrombosis [2]
For patients patients with ulcers that might not be due to venous insufficiency, but rather have an atypical appearance [19] - Biopsy (see topic "How to Perform a Wound Biopsy")
- Referral to a subspecialist
For patients with VLUs with signs of infection: - Wound culture (see topic "How to Collect a Wound Swab (Levine Technique) for Culture")
For patients with anatomical venous anomalies, and patients in whom surgical intervention on the deep venous system is planned.
- X-ray contrast venography, magnetic resonance, or computed tomography venography [19]
|
Noninvasive arterial tests
Noninvasive arterial tests are recommended to rule out peripheral arterial disease and to determine ulcer healing potential.
- Medicare Quality Payment Program, Quality Measure: "Noninvasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential"
- Ankle Brachial index (ABI) ratio for patients with lower extremity ulcer, no diabetes and no arterial calcification (See Table 2). [19]
-
- ABI testing can be completed with a hand-held Doppler machine and sphygmomanometer, or an automated ABI device. See topic "How to Perform An Ankle Brachial Index".
- Medicare will cover ABI and other noninvasive arterial testing if specific criteria are met.[55]
- Audible handheld Doppler ultrasound with continuous waveform analysis, toe pressure, transcutaneous oxygen pressure (TCOM, TcPO2) are preferable for patients with diabetes or arterial calcification (See Table 2)
-
- Clinicians can measure toe pressure by placing a small toe cuff around the great toe and attaching a plethysmography probe at the pulp of great toe tip. The cut-off values of toe pressure and toe brachial index (TBI) are arbitrary and vary in the literature. A toe pressure lower than 30 mmHg or TBI 0.2-0.25 is considered severely ischemic and diagnostic of critical limb ischemia (CLI). Wound healing potential drops as TBI decreases from the normal values.[56] See topic " How to Interpret Audible Handheld Doppler Ultrasound and Waveforms to Rule out PAD".
-
Microcirculation assessment prior to primary therapy in patients can be used when concomitant arterial etiology is suspected, if arterial calcification or diabetes, or for monitoring of advanced wound therapy.[2]
-
- TCOM near VLU: if >= 30mmHg, rules out severe arterial disease and predicts VLU healing.[37]
Table 2. Arterial noninvasive bedside tests and likely interpretation
For compression therapy according to interpretation of arterial noninvasive tests, see algorithms 'Based on ankle brachial index (ABI)' or 'Based on audible handheld Doppler ultrasound or continuous waveform analysis', and section 'Compression Therapy' in topic "Venous Ulcers - Treatment and Prevention". For details on noninvasive arterial tests, see section 'Noninvasive arterial tests' in topic "Arterial Ulcers - Introduction and Assessment".
ABI: ankle brachial pressure, AP: ankle systolic pressure, TP: toe systolic pressure, TcPO2 or TCOM: transcutaneous oxygen pressure, TBI: toe brachial index, SPP: skin perfusion pressure.( * ) ABI, toe pressure, TBI values are frequently falsely elevated in patients with diabetes. Patients with diabetes should have TP measurements [57][58]. If arterial calcification precludes reliable ABI or TP measurements, or if ABI is non-compressible (>1.3), ischemia should be documented by TcPO2, SPP, or Doppler continuous waveform analysis [57][59]. (**) Biphasic waveform may be normal in older individuals or when there is no clear transition from triphasic signal along the vascular tree .
| Interpretation |
ABI (no diabetes) [57]
|
ABI (with diabetes)* [60]
|
Ankle Pressure (mmHg) [57]
|
TcPO2 or TCOM (mmHg) [58]
|
Toe Pressure (mmHg) [57]
|
Doppler waveform [60][61][62]
|
TBI (diabetes) [60][61][62]
|
Skin Perfusion Pressure (mmHg) [60][63]
|
| Non-compressible arteries |
>1.3 |
>1.3 |
|
|
|
|
|
|
| No relevant ischemia |
0.8-1.3 |
0.9-1.3 |
>100 |
>40 |
>=60 |
triphasic or
biphasic **
|
>=0.70 |
>40 |
| Mild/ Moderate ischemia |
0.4-0.79 |
0.5 -0.89 |
50-100 |
30-40 |
30-59 |
biphasic or
biphasic/monophasic
|
0.25-0.69 |
30-40 |
| Severe ischemia |
<0.4 |
<0.5 |
<50 |
<30 |
<30 |
monophasic |
<0.25 |
<30 |
Functional/Diagnostics tests for chronic venous disease
- 1BFor all patients with chronic venous disease of the lower extremities, guidelines recommend a comprehensive venous duplex ultrasound (DUS) as the diagnostic test of choice to evaluate for venous reflux. [2][5][10][38]
-
-
Rationale: For a leg ulcer to be classified as a VLU, objective documented evidence of venous disease is needed.[2] The correct method/type of ultrasound should be ordered to decrease chances of inconclusive results. Evaluation for both obstructive and reflux patterns of venous disease with comprehensive color flow venous duplex ultrasound including B-mode gray-scale imaging, pulsed Doppler sampling, and color flow analysis, in supine and standing positions is considered first-line.[2][5][10]
-
- Common findings in limbs with VLU are venous reflux (superficial and/or deep) and outward flow in perforators.[64][10]
- Referral to vascular surgeon is recommended in cases with significant superficial junctional venous reflux (saphenofemoral or saphenopopliteal junction reflux >500 ms) [38][10] or superficial reflux directed to the ulcer bed [2], deep vein incompetence/obstruction [2][38], or perforator incompetence (outward flow of >500 ms duration, with a diameter of >3.5mm located beneath or associated with the ulcer bed) [2][38][10] or past history of venous surgery [38] For details on DUS diagnostic findings refer to Table 3 below. For a review on relevant anatomy of the venous system see section 'Vascular System of the Lower Extremities' in topic "Applied Anatomy and Physiology in Wound Care".
-
Venous plethysmography for routine initial evaluation of VLU is discouraged unless results of venous duplex ultrasound are inconclusive, or if patient has recurrent or recalcitrant VLU [2].
-
-
Rationale: Plethysmography can identify hemodynamic obstruction patterns. If venous refill time measured with below-knee tourniquet and photoplethysmography is greater than 20 mmHg after vein surgery, there is good chance of VLU healing and non-recurrence [37].
-
Laboratory evaluation for thrombophilia for patients with a history of recurrent or recalcitrant VLU or thrombosis: these patients have a higher prevalence of thrombophilia, which is associated with recurrent and recalcitrant ulcers [2]. Laboratory evaluation includes [2]:
-
- Inherited hypercoagulable factors (anti- thrombin deficiency, protein C and protein S deficiencies)
- Factor V Leiden (resulting in activated protein C resistance)
- Prothrombin G20210A
- Plasminogen activator inhibitor type 1 mutations
- Hyperhomocysteinemia,
- Antiphospholipid antibodies (anticardiolipin and lupus anticoagulant),
- Cryoglobulins and cryoagglutinins
- Factor VIII related antigen, von Willerbrand factor (VWF), D-dimer and factor V Leiden: if indicative of hypercoagulation tendency, pose a risk factor for post-thrombotic syndrome.[37]
- Routine wound culture is not advised. Instead, guidelines suggest wound culture only when VLU shows clinical signs of infection. See topic "How to Collect a Wound Swab (Levine Technique) for Culture".
- Wound biopsy is indicated in VLUs that fail standard therapy after 4 weeks of treatment or for differentiation from other possible non-venous causes for leg ulcer.[2][5] See topic "How to Perform a Wound Biopsy"
Table 3. Summary of clinical practice guidelines on duplex ultrasound (DUS) diagnostic findings for assessing venous reflux in patients with chronic venous disease of the lower extremities [10] Abbreviations: GSV: great saphenous vein, SSV: small saphenous vein, AAGSV: anterior accessory great saphenous vein, and PAGSV: posterior accessory great saphenous vein. For a review on relevant anatomy of the venous system see section 'Vascular System of the Lower Extremities' in topic "Applied Anatomy and Physiology in Wound Care".
| DUS diagnostic criteria and good practice recommendations |
DUS criteria for reflux and pathologic perforating veins - Reflux Criteria:
- Superficial truncal veins (GSV, SSV, AAGSV, PAGSV) tibial, deep femoral, and perforating veins: Reflux is defined as a minimum value >500 ms of reversed flow.
- Common femoral, femoral, and popliteal veins: Reflux is diagnosed with a minimum value of >1 second of reversed flow. No minimum vein diameter is required for diagnosis.
- Axial Reflux Definitions:
- GSV: Retrograde flow from the groin to the upper calf.
- SSV: Retrograde flow from the knee to the ankle.
- AAGSV and PAGSV: Retrograde flow measured between two points at least five cm apart.
- Pathologic perforating veins:
- Outward flow duration of >500 ms and a diameter of >3.5 mm on DUS.
Good Practice Recommendations for DUS Evaluation: - The SVS recommends that DUS be performed in an Intersocietal Accreditation Commission or American College of Radiology accredited vascular laboratory by a credentialed ultrasonographer, preferably with the patient in a standing position. A sitting or reverse Trendelenburg position can be used if the patient cannot stand.
- The study should be interpreted by a physician trained in venous DUS interpretation.
Consensus for Patient Evaluation: - CEAP Class C2 and beyond (see Table 5): mandatory evaluation of the deep venous system for obstruction or valvular incompetence
|
Differential Diagnosis
For differential diagnosis, observing the progression of leg edema throughout the day is crucial. For instance, in venous diseases of the lower limbs, leg edema worsens in positions influenced by gravity and lessens when the limb is elevated. Symptoms are key indicators: intense pain may suggest arterial diseases, while a sense of heaviness or fatigue in the legs often points to venous disease.[65] For a comparison of clinical findings observed during physical examination of common types of lower leg ulcers, refer to section 'Physical Examination' in topic "How to Assess a Patient with Chronic Wounds" and to the 'Algorithm for Assessment of Patients with Chronic Wounds' in topic "How to Assess a Patient with Chronic Wounds". Table 4 below shows a list of differential diagnosis for VLU.[65][66]
Table 4. Differential diagnosis of venous leg ulcers
| Common differential diagnosis | Comments |
| Arterial ulcers | - Typically painful, and punched out or stellate in appearance. The surrounding skin is red and taut. Some arterial ulcers are pale; others may have a black or yellow eschar.
- See topic "Arterial Ulcer - Introduction and Assessment"
|
| Mixed arterial venous ulcers | - Ulcers due to CVI and arterial vascular disease, showing mixed characteristics of VLUs and arterial ulcers.
- See section 'Characterization of VLUs' below.
|
| Lymphedema | - Lymphedema is defined as progressive swelling (edema) of a specific body part due to insufficiency of the lymphatic system. Chronic skin ulcers can occasionally be caused by lymphedema alone. However, they are frequently of mixed origin. Lymphedema of lower extremities is frequently associated with chronic venous insufficiency (CVI) in a condition known as phlebolymphedema.[67]
- For patients with suspected lymphedema, duplex ultrasonography is the initial test to rule out venous disease.
- See topic "Lymphedema - Introduction and Assessment"
|
| Neuropathic ulcers | - Usually occurs on feet in patients with diabetes, neurologic disorders, or Hansen disease.
- See topic "Diabetic Foot Ulcer - Introduction and Assessment"
|
| Pressure ulcer/injury | - Pressure ulcer/injury: usually located over bony prominences; risk factors include impaired mobility, altered mental status
- See topic "Pressure Ulcers/Injuries - Introduction and Assessment"
|
| Other differential diagnosis | Comments |
| Drug-induced ulcers | - Hydroxyurea: used for treatment of myeloproliferative diseases, hydroxyurea may cause hyperpigmentation and ulcerations, which can mimic CVD.[68]
- Minocycline: used for treatment of rosacea or acne, minocycline can lead to cutaneous hyperpigmentation.[69]
- Xylazine-Induced skin ulcers
|
| Genetic | - Lipedema: more prevalent in women, lipedema evolves with symmetrical fatty deposit accumulations from the lateral parts to the medial aspects of the skin but there will be no fatty deposit accumulations below the ankle.[70]
- See lipedema cases in topic "Case: Circumferential Negative Pressure Wound Therapy"
|
Hematologic
| - Sickle cell disease
- Thalassemia
- Polycythemia vera (and hydroxyurea therapy)
|
Infectious
| - Orf is a DNA virus belonging to the parapoxvirus family which is transmitted to humans by zoonotic routes through contact with infected animals and may cause ulcers that mimic VLUs.[71]
- Cutaneous disseminated sporotrichosis has been described as a differential diagnosis for VLU.[72]
|
| Inflammatory | - Pyoderma gangrenosum. See topic "Pyoderma Gangrenosum - Introduction and Assessment"
- Necrobiosis lipoidica
- Polyarteritis nodosa
- Schamberg disease: most common type of pigmented purpuric dermatoses (PPDs). Presents as an idiopathic, benign, chronic, cutaneous eruptions characterized by petechiae, purpura, and increased skin pigmentation (brown, red, or yellow patchy) distributed primarily on the lower extremities. Tourniquet test is positive in about half the patients indicating capillary fragility, but no hematologic abnormalities have been described. The histopathologic picture is characterized by inflammation of the capillaries in the upper dermis, diapedesis of red cells, and the deposition of hemosiderin. Prognosis for complete recovery is excellent.[73]
|
| Malignant | - Basal cell carcinoma
- Squamous cell carcinoma
- Marjolin's ulcer
|
| Metabolic | - Calciphylaxis: a rare but life-threatening calcific vasculopathy affecting the microvessels in the dermis and subcutaneous tissue, characterized by painful cutaneous ischemic lesions. Calciphylaxis is more commonly associated with end-stage renal disease (ESRD) requiring dialysis. However, it can also occur in other diseases with normal renal function, including autoimmune disease, polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, and skin changes (POEMS) syndrome, cancer, and coronavirus disease 2019.[74]
|
Characterization of VLUs
After differential diagnoses are ruled out and etiology is established, expert consensus recommends categorizing VLUs as "simple", "complex" or of mixed etiology to determine likely prognosis, so that appropriate time frames for monitoring, reassessment and specialist referral can be established [6]:
- Simple VLU:
-
- Area < 100 cm2 and onset < 6 months with limited co-morbidities
- Complex VLU:
-
- Area > 100 cm2 and/or wound onset > 6 months (no other co-morbidities)
- < 30% decrease in wound area after 4 weeks of adequate treatment
- Lymphovenous disease
- Associated lipedema
- Leg/ulcer infection
- Stable cardiac heart failure
- History of non-adherence
- Mixed arterial venous ulcer:
-
- ABI > 1.3: Non-compressible arteries
- ABI 0.5-0.8: Mixed arterial ulcer with mild/moderate ischemia
- ABI <0.5: Mixed arterial ulcer with severe ischemia
CEAP Classification System
- Clinical guidelines recommend documenting the level of venous insufficiency with a standardized score such as the CEAP (Clinical-Etiology-Anatomy-Pathophysiology) classification system (Table 5). The clinical or basic CEAP classification can be used for clinical practice, and the full CEAP classification system should be used for clinical research.[37][10]
- Relevant chronic venous disease classification systems such as CEAP criteria can guide the assessment of CVD.[5] Developed by an international consensus, CEAP classifies lower extremity venous disease based upon clinical signs, etiology, anatomic location, and pathophysiologic abnormality. It is an internationally accepted standard for describing patients with chronic venous disorders and it has been used for reporting clinical research findings in scientific journals.[75]
- In 2020, the CEAP classification was updated.[75] These changes include adding Corona phlebectatica as the C4c clinical subclass, introducing the modifier "r" for recurrent varicose veins and recurrent venous ulcers, and replacing numeric descriptions of the venous segments by their common abbreviations.[75]
- CEAP limitations include the fact that it was designed as a descriptive classification and does not attempt to measure disease severity or outcomes of therapy.[75]
Table 5. The 2020 revision of CEAP: Abbreviations and Descriptions of Clinical, Etiologic, Anatomic and Pathophysiologic Classification of Chronic Venous Disease [75]
| Clinical | Etiologic | Anatomic | Pathophysiologic |
- C0 No visible or palpable signs of venous disease
- C1 Telangiectasias or reticular veins
- C2 Varicose veins
- C2r Recurrent varicose veins
- C3 Edema
- C4 Changes in skin and subcutaneous tissue secondary to chronic venous disease
- C4a Pigmentation or eczema
- C4b Lipodermatosclerosis or atrophie blanche
- C4c Corona phlebectatica
- C5 Healed ulcer
- C6 Active venous ulcer
- C6r Recurrent active venous ulcer
| - Ep Primary
- Es Secondary
- Esi Secondary – intravenous
- Ese Secondary – extravenous
- Ec Congenital
- En No cause identified
| - As Superficial
- Tel Telangiectasia
- Ret Reticular veins
- GSVa Great saphenous vein above knee
- GSVb Great saphenous vein below knee
- SSV Small saphenous vein
- AASV Anterior accessory saphenous vein
- NSV Nonsaphenous vein
- Ad Deep
- IVC Inferior vena cava
- CIV Common iliac vein
- IIV Internal iliac vein
- EIV External iliac vein
- PELV Pelvic veins
- CFV Common femoral vein
- DFV Deep femoral vein
- FV Femoral vein
- POPV Popliteal vein
- TIBV Crural (tibial) vein
- PRV Peroneal vein
- ATV Anterior tibial vein
- PTV Posterior tibial vein
- MUSV Muscular veins
- GAV Gastrocnemius vein
- SOV Soleal vein
- Ap Perforator
- TPV Thigh perforator vein
- CPV Calf perforator vein
- An No venous anatomic location identified
| Pr RefluxPo ObstructionPr,o Reflux and obstructionPn No pathophysiology identified |
Note: Each Clinical class is subcharacterized by a subscript indicating the presence (symptomatic, s) or absence (asymptomatic, a) of symptoms attributable to venous disease.
Examples of application of the CEAP classification:
- A patient presents with swelling of the leg. On physical examination, the examiner observes varicose veins, and a recurrent active venous ulcer. The duplex scanning report shows great saphenous vein reflux and popliteal and anterior tibial reflux. Signs of postthrombotic obstruction are negative.
- CEAP classification: C2,3,6 Ep As,Ad Pr.
- C3: Presence of edema due to swelling of the leg.
- C2: Presence of varicose veins.
- C6: Presence of a recurrent active venous ulcer.
- E: Etiology is primary (Ep), as postthrombotic signs are negative.
- A: Anatomic involvement includes the superficial (As) saphenous vein and deep (Ad) popliteal and anterior tibial veins.
- P: Pathophysiology is reflux (Pr), as indicated by the duplex scanning report.
- A patient comes in with swelling and tightness of the leg. On physical examination, the examiner observes varicose veins, edema, lipodermatosclerosis, and healed ulceration. The duplex scanning report shows great saphenous vein reflux and popliteal and anterior tibial reflux. Signs of postthrombotic obstruction are negative.
- CEAP Classification: C2,3,4b,5, S, Ep, As,d, Pr
Venous Clinical Severity Score (VCSS)
- Clinical guidelines recommend the use of the revised Venous Clinical Severity Score (VCSS) for patients with chronic venous disorders for grading of clinical severity and for assessment of post treatment outcome.[10][11][16]
- Rationale: The Venous Clinical Severity Score (VCSS) complements the CEAP classification’s descriptive nature and static categorical classification scheme by providing a dynamic measure of venous disease severity, reflecting changes over time and treatment response. The VCSS includes 9 parameters of venous disease with a symptom severity scale from 0 to 3 (0–1=mild; 2=moderate; and 3=severe). The scored parameters include pain, varicose veins, edema, skin pigmentation, inflammation, induration, ulcers (number, size, and duration), and compression therapy.[10][11][16]
Ulcer healability
This step involves assessing whether the ulcer can be healed with conservative management only (healable) or not (non-healable), or if co-existing medical conditions, drugs or circumstances will likely impede wound healing (maintenance). Ulcer healability classification helps in determining an adequate treatment plan.[49] A summary is provided below; for more details see topic "How to Determine Healability of a Chronic Wound". After determining ulcer healability, see "Venous ulcers - Treatment and Prevention"
Table 6: Determining ulcer healability
( * ) As determined by comprehensive patient assessment. Maintenance wounds have healing potential but patient or health system barriers compromise healing (**) For persons without diabetes, inadequate blood supply is objectively confirmed by ankle-brachial index (ABI) < 0.5, monophasic doppler waveform, skin perfusion pressure < 30mmHg, transcutaneous oxygen < 30mmHg, absolute systolic ankle pressure < 50 mmHg OR toe pressure < 30mmHg. For persons with diabetes, perform any other testing listed above besides ABI as ABI can be falsely elevated
| Can underlying cause be treated? |
How is blood supply to the wound? |
Co-existing medical conditions/drugs... |
Then wound prognosis is...
|
| Yes |
Adequate |
Are not an obstacle for healing |
Healable
|
| No (*) |
Adequate |
May or may not prevent healing |
Maintenance
|
| No |
Usually inadequate (**) |
May inhibit healing |
Non-healable |
Modified from Sibbald RG et al. 2011[49].
- If patient has any of the conditions below, consider a non-healing program. VLU will likely not heal with conservative treatment only:
-
- Co-morbidities that impede healing:
-
- Ulcer is malignant tumor,
- Major organ failure
- Blood supply to the VLU is inadequate as determined by non-invasive vascular arterial tests (ABI, Doppler, TCOM, other exams)
- If patient has any of the conditions that impede wound healing below, consider a maintenance-healing program until element impeding healing is mitigated:
-
- Co-morbidities:
-
- Uncontrolled diabetes
- Immunosuppression
- Obesity: BMI > 40
- Inadequate nutrition (abnormal serum protein, unintended weight loss)
- Cognitive, emotional, psychological dysfunction
- Calf muscle pump disfunction (arthritic conditions, paralysis, etc)
- Drugs and interventions :
-
- Steroids
- Chemotherapy/ radiation
- Immunosuppressants
- Lifestyle:
-
- Regular smoking
- Impaired mobility
- Financial or resource constraints
Experimental Diagnostics
- Ulcer exudate biomarkers measurement with Multiplex ELISA: a single center study found the biomarkers granulocyte macrophage-colony stimulating factor (GM-CSF) and matrix metalloprotease-13 (MMP-13) to be accurate predictive biomarkers of VLU healing. Results suggested that VLUs with GM-CSF values greater than 29.5 pg/mL or with MMP-13 values greater than 962.2 pg/mL in their exudate will not decrease in size (that is, the the VLU is nonhealing), and thus treatment plan should be reassessed.[76] While results are promising, further validation and development of a point-of-care test are needed before use in clinical practice.
-
Documentation
- Documentation of VLU is important to assess healing progress, as they determine whether a treatment plan should be continued or not. VLU progress should be recorded weekly or sooner if significant change.
- All wound care services provided need to be documented in a way that supports the Medical Necessity requirements, and facilitate evaluation and subsequent care of VLUs. Many VLUs are refractory to healing or have complicated healing cycles either because of the nature of the wound itself or because of complicating metabolic and/or physiological factors.
- Documentation should include number and position of ulcers on the leg. Wound measurements should be made for each VLU, including area, perimeter, and depth, description of wound edge, peri-wound area, wound base quality, amount and type of drainage, and infection, history of debridement. [2]
-
-
Wound measurement methods include manually measuring length and width (the longest length with the greatest width at right angles), manual tracing, digital photography, and software programs that calculate wound dimensions from a photograph of the lesion. Wound tracings that calculate the area via digital software are slightly better than linear measurement [5].
Documenting signs of VLU improvement to support medical necessity (Medicare):
- Reimbursement for wound care services on a continuing basis for a particular wound in a patient requires documentation in the patient's record that the wound is improving in response to the wound care being provided.
- It is not medically reasonable or necessary to continue a given type of wound care if evidence of wound improvement cannot be shown.
- Medicare expects that with appropriate care, wound volume or surface dimension should decrease by at least 10 percent per month or wounds will demonstrate margin advancement of no less than 1 mm/week.
- Medicare expects the wound-care treatment plan to be modified in the event that appropriate healing is not achieved.
- Such evidence must be documented with each date of service provided.
- Evidence of improvement includes measurable changes (decreases) of some of the following:
-
- Drainage
- Inflammation
- Swelling
- Pain
- Wound dimensions (diameter, depth)
- Necrotic tissue/slough
Documentation tools:
- Tools that facilitate standardized assessment should be used:
-
- Wound Reference Wound Prep & Dress Tool creates notes to help support medical necessity that can be copied and pasted to electronic medical records
-
Validated wound assessment tools such as Bates-Jensen Tool.[47]
- The CEAP classification system and the VCSS scoring system may be used to describe chronic venous disorders in a standardized fashion. See section 'CEAP Classification System' above.
-
Patient reported outcome (PRO) Tools: as part of a patient-centered approach, it is recommended that clinicians adopt PRO tools to assess patient’s Quality of Life (QOL), pain, and depression [7] PROM provide a comprehensive picture of patient’s health [77], which can be used to optimize plan of care.
-
-
QOL tools validated for VLU patients: the Nottingham Health Profile (NHP) and Venous Leg Ulcer Quality of Life (VLU-QoL) questionnaire seem to be the most suitable PROM for use by clinicians.[77] Others include VEINES - QoL/Sym tool, the Medical Outcomes Survey 12 item Short-Form (SF-12) the Short-Form Health Survey, 36 items (SF-36).[7]
-
- Medicare Quality Payment Program, Improvement Activity "Promote Use of Patient-Reported Outcome Tools" suggests use of Wound-Quality of Life (QoL) and patient-reported Wound Outcome.[78]
-
Pain measurement tools validated for VLU patients: include the Medical Outcomes Survey 12-item Short- Form (SF-12), the Visual Analogue Scale, and the McGill Pain Questionnaire, a subscale of the Nottingham Health Profile. [7]
-
Depression measurement / assessment tools validated for VLU patients: include the Hospital Anxiety and Depression Scale (HADS), the Euroqol 5 dimensions (EQ-5D), and the Nottingham Health Profile. [7]
CODING
ICD-10
- Identify and document first any documented underlying condition (ICD-10-CM documentation)
-
-
Chronic venous hypertension with ulcer (I87.31-, I87.33-)
- Post-phlebitic syndrome with ulcer (I87.01-, I87.03-)
- Post-thrombotic syndrome with ulcer (I87.01-, I87.03-)
-
Varicose ulcer (I83.0-, I.83.2-)
- Specify laterality
-
- Right, left or unspecified
- Specify ulcer severity: Select code for non-pressure chronic ulcer of the calf [79]
-
- Limited to breakdown of skin
- With fat layer exposed
- With necrosis of muscle
- With necrosis of bone
- Unspecified severity
APPENDIX
ICD-10 Coding
- Red arrows indicate non-billable code, Green arrows are billable codes
|
Coding Chronic venous hypertension (Back to text)
 I83 Varicose veins of lower extremities I83 Varicose veins of lower extremities
I83.0 Varicose veins of lower extremities with ulcer
I83.00 Varicose veins of unspecified lower extremity with ulcer
 I83.001 …… of thigh I83.001 …… of thigh
I83.002 …… of calf
I83.003 …… of ankle
I83.004 …… of heel and midfoot
I83.005 …… other part of foot
I83.008 …… other part of lower leg
I83.009 …… of unspecified site
I83.01 Varicose veins of right lower extremity with ulcer
I83.011 …… of thigh
I83.012 …… of calf
I83.013 …… of ankle
I83.014 …… of heel and midfoot
I83.015 …… other part of foot
I83.018 …… other part of lower leg
I83.019 …… of unspecified site
I83.02 Varicose veins of left lower extremity with ulcer
I83.021 …… of thigh
I83.022 …… of calf
I83.023 …… of ankle
I83.024 …… of heel and midfoot
I83.025 …… other part of foot
I83.028 …… other part of lower leg
I83.029 …… of unspecified site
I83.2 Varicose veins of lower extremities with both ulcer and inflammation
I83.20 Varicose veins of unspecified lower extremity with both ulcer and inflammation
I83.201 Varicose veins of unspecified lower extremity with both ulcer of thigh and inflammation
I83.202 Varicose veins of unspecified lower extremity with both ulcer of calf and inflammation
I83.203 Varicose veins of unspecified lower extremity with both ulcer of ankle and inflammation
I83.204 Varicose veins of unspecified lower extremity with both ulcer of heel and midfoot and inflammation
I83.205 Varicose veins of unspecified lower extremity with both ulcer other part of foot and inflammation
I83.208 Varicose veins of unspecified lower extremity with both ulcer of other part of lower extremity and inflammation
I83.209 Varicose veins of unspecified lower extremity with both ulcer of unspecified site and inflammation
I83.21 Varicose veins of right lower extremity with both ulcer and inflammation
I83.211 Varicose veins of right lower extremity with both ulcer of thigh and inflammation
I83.212 Varicose veins of right lower extremity with both ulcer of calf and inflammation
I83.213 Varicose veins of right lower extremity with both ulcer of ankle and inflammation
I83.214 Varicose veins of right lower extremity with both ulcer of heel and midfoot and inflammation
I83.215 Varicose veins of right lower extremity with both ulcer other part of foot and inflammation
I83.218 Varicose veins of right lower extremity with both ulcer of other part of lower extremity and inflammation
I83.219 Varicose veins of right lower extremity with both ulcer of unspecified site and inflammation
I83.22 Varicose veins of left lower extremity with both ulcer and inflammation
I83.221 Varicose veins of left lower extremity with both ulcer of thigh and inflammation
I83.222 Varicose veins of left lower extremity with both ulcer of calf and inflammation
I83.223 Varicose veins of left lower extremity with both ulcer of ankle and inflammation
I83.224 Varicose veins of left lower extremity with both ulcer of heel and midfoot and inflammation
I83.225 Varicose veins of left lower extremity with both ulcer other part of foot and inflammation
I83.228 Varicose veins of left lower extremity with both ulcer of other part of lower extremity and inflammation
I83.229 Varicose veins of left lower extremity with both ulcer of unspecified site and inflammation
|
|
ICD-10 – post phlebitic (Back to text)
- Red arrows indicate non-billable code, Green arrows are billable codes
I87.01 Postthrombotic syndrome with ulcer
I87.011 …… of right lower extremity
I87.012 …… of left lower extremity
I87.013 …… of bilateral lower extremity
I87.019 …… of unspecified lower extremity
I87.03 Postthrombotic syndrome with ulcer and inflammation
I87.031 …… of right lower extremity
I87.032 …… of left lower extremity
I87.033 …… of bilateral lower extremity
I87.039 …… of unspecified lower extremity
|
|
ICD-10 – varicose ulcer (Back to text)
- Red arrows indicate non-billable code, Green arrows are billable codes
I83 Varicose veins of lower extremities
I83.0 Varicose veins of lower extremities with ulcer
I83.00 Varicose veins of unspecified lower extremity with ulcer
I83.001 …… of thigh
I83.002 …… of calf
I83.003 …… of ankle
I83.004 …… of heel and midfoot
I83.005 …… other part of foot
I83.008 …… other part of lower leg
I83.009 …… of unspecified site
I83.01 Varicose veins of right lower extremity with ulcer
I83.011 …… of thigh
I83.012 …… of calf
I83.013 …… of ankle
I83.014 …… of heel and midfoot
I83.015 …… other part of foot
I83.018 …… other part of lower leg
I83.019 …… of unspecified site
I83.02 Varicose veins of left lower extremity with ulcer
I83.021 …… of thigh
I83.022 …… of calf
I83.023 …… of ankle
I83.024 …… of heel and midfoot
I83.025 …… other part of foot
I83.028 …… other part of lower leg
I83.029 …… of unspecified site
I83.2 Varicose veins of lower extremities with both ulcer and inflammation
I83.20 Varicose veins of unspecified lower extremity with both ulcer and inflammation
I83.201 Varicose veins of unspecified lower extremity with both ulcer of thigh and inflammation
I83.202 Varicose veins of unspecified lower extremity with both ulcer of calf and inflammation
I83.203 Varicose veins of unspecified lower extremity with both ulcer of ankle and inflammation
I83.204 Varicose veins of unspecified lower extremity with both ulcer of heel and midfoot and inflammation
I83.205 Varicose veins of unspecified lower extremity with both ulcer other part of foot and inflammation
I83.208 Varicose veins of unspecified lower extremity with both ulcer of other part of lower extremity and inflammation
I83.209 Varicose veins of unspecified lower extremity with both ulcer of unspecified site and inflammation
I83.21 Varicose veins of right lower extremity with both ulcer and inflammation
I83.211 Varicose veins of right lower extremity with both ulcer of thigh and inflammation
I83.212 Varicose veins of right lower extremity with both ulcer of calf and inflammation
I83.213 Varicose veins of right lower extremity with both ulcer of ankle and inflammation
I83.214 Varicose veins of right lower extremity with both ulcer of heel and midfoot and inflammation
I83.215 Varicose veins of right lower extremity with both ulcer other part of foot and inflammation
I83.218 Varicose veins of right lower extremity with both ulcer of other part of lower extremity and inflammation
I83.219 Varicose veins of right lower extremity with both ulcer of unspecified site and inflammation
I83.22 Varicose veins of left lower extremity with both ulcer and inflammation
I83.221 Varicose veins of left lower extremity with both ulcer of thigh and inflammation
I83.222 Varicose veins of left lower extremity with both ulcer of calf and inflammation
I83.223 Varicose veins of left lower extremity with both ulcer of ankle and inflammation
I83.224 Varicose veins of left lower extremity with both ulcer of heel and midfoot and inflammation
I83.225 Varicose veins of left lower extremity with both ulcer other part of foot and inflammation
I83.228 Varicose veins of left lower extremity with both ulcer of other part of lower extremity and inflammation
I83.229 Varicose veins of left lower extremity with both ulcer of unspecified site and inflammation
|
|
ICD-10 – nonpressure ulcer (Back to text)
- Red arrows indicate non-billable code, Green arrows are billable codes
L97.2 Non-pressure chronic ulcer of calf
L97.20 Non-pressure chronic ulcer of unspecified calf
L97.201 …… limited to breakdown of skin
L97.202 …… with fat layer exposed
L97.203 …… with necrosis of muscle
L97.204 …… with necrosis of bone
L97.209 …… with unspecified severity
L97.21 Non-pressure chronic ulcer of right calf
L97.211 …… limited to breakdown of skin
L97.212 …… with fat layer exposed
L97.213 …… with necrosis of muscle
L97.214 …… with necrosis of bone
L97.219 …… with unspecified severity
L97.22 Non-pressure chronic ulcer of left calf
L97.221 …… limited to breakdown of skin
L97.222 …… with fat layer exposed
L97.223 …… with necrosis of muscle
L97.224 …… with necrosis of bone
L97.229 …… with unspecified severity
|
REVISION UPDATES
| Date |
Description |
| 1/2/24 | Updated and expanded sections 'Pathophysiology', 'Diagnosis' and 'Differential Diagnosis' |
| 6/19/19 |
Updated section 'Assessment', updated references, added new photos, added information on Medicare coverage for noninvasive arterial testing |
| 10/24/19 | Added section 'Experimental Diagnostics', updated references |