Last updated on 9/17/24 | First published on 9/25/17 | Literature review current through Jul. 2026
[cite]
Authors:
Jeff Mize RRT, CHT, UHMSADS,
Tiffany Hamm BSN, RN, CWS, ACHRN, UHMSADS,
Steven Orr MD, FACEP/UHM, FAPWCA,
Elaine Horibe Song MD, PhD, MBA,
Topic editors:
Eugene Worth MD, M.Ed., FABA, ABPM/UHM,
more...
Coauthor(s)
Jeff Mize, RRT, CHT, UHMSADS
Disclosures: Nothing to disclose
Tiffany Hamm, BSN, RN, CWS, ACHRN, UHMSADS
Chief Nursing Officer, Wound Reference, IncDisclosures: Nothing to disclose
Steven Orr, MD, FACEP/UHM, FAPWCA
Disclosures: Nothing to disclose
Elaine Horibe Song, MD, PhD, MBACo-Founder and Editor, Wound Reference, Inc;
Professor (Affiliate), Division of Plastic Surgery, Federal University of Sao Paulo;
Volunteer, Association for the Advancement of Wound Care;
Google Scholar Profile
Disclosures: Nothing to disclose
Editors
Eugene Worth, MD, M.Ed., FABA, ABPM/UHM
Disclosures: Nothing to disclose
For full access to this topic and more
premium content, upgrade today. Or get started with a Free Basic account (limited content and tools).
INTRODUCTION
The purpose of this topic is to provide practitioners of Hyperbaric Oxygen Therapy (HBO) an in-depth summary of HBO indications and common HBO treatment protocols. For an introduction to HBO, refer to An Introduction to Hyperbaric Oxygen Therapy
Treatment Protocol Guidelines
The following hyperbaric medicine treatment protocols are based upon the recommendations of the Hyperbaric Oxygen Committee of the Undersea and Hyperbaric Medical Society. Clinical protocols and/or practice guidelines are systematically developed statements that help physicians, other practitioners, case managers and clients make decisions about appropriate health care for specific clinical circumstances.
Protocols allow health providers to offer evidence-based, appropriate, standardized diagnostic treatment and care services to patients undergoing hyperbaric therapy. Evidenced-based medicine offers clinicians a way to achieve improved quality, improved patient satisfaction, and reduced costs. Utilization Review should be initiated when clinical decisions result in deviation from or modification of treatment protocols. This includes any course of treatment at or above the recognized threshold limits.
Medical Necessity
Medicare.gov defines “medically necessary” as “health-care services or supplies needed to prevent, diagnose, or treat an illness, injury, condition, disease, or its symptoms and that meet accepted standards of medicine.”
The following conditions meet coverage indications per the National Coverage Determination (NCD) 20.29.[1] Continued HBO therapy without documented evidence of effectiveness does not meet the Medicare definition of medically necessary treatment. Thorough re-evaluation should be made at least every 30 days for documentation of response to therapy.
HBO INDICATIONS
By Indication
-
Chronic Refractory Osteomyelitis
-
Osteoradionecrosis - Mandibular
-
Soft Tissue Radiation Injury
-
Diabetic Foot Ulcer
-
Compromised Skin Grafts and Flaps, digit/limb replantation
See all indications below in "Evidence-based indications accepted by the UHMS, approved by Medicare" and "Evidence-based indications accepted by the UHMS, NOT approved by Medicare"
By Treatment Protocol
Table 1: 90 minutes of oxygen breathing at 2 ATA without air break
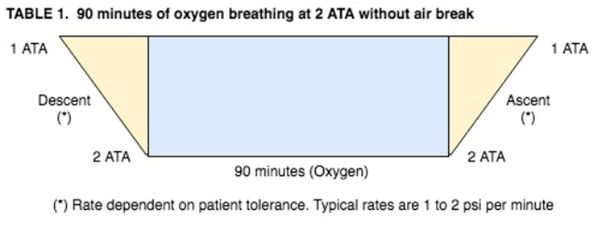
Table 1 based on Kindwall and Whelan [2] and National Baromedical Services [3]
Indications:
|
Topics
|
Sample Physician Order
|
HBO request requirements checklist
and sample EMR documentation |
|
Acute Exceptional Blood Loss Anemia
|
|
-
|
|
Acute Peripheral Ischemia, Crush Injury and Compartment Syndrome
|
/
|
- |
|
Chronic Refractory Osteomyelitis
|
|
|
|
Compromised Skin Grafts & Flaps, digit/limb replantation
|
|
|
|
Diabetic Foot Ulcer
|
|
|
|
Soft Tissue Radiation Injury
|
|
|
|
Pyogenic and Invasive Fungal Intracranial Abscesses
|
|
- |
Table 2: 90 minutes of oxygen breathing at 2 ATA with air break
(patients with high seizure risk)
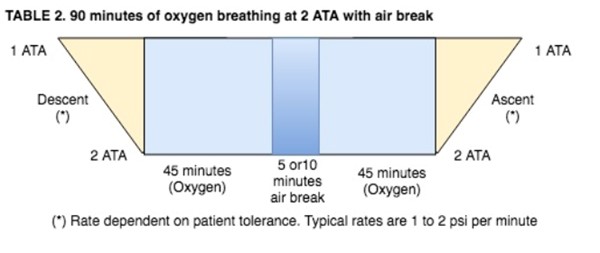
Table 2 based on Kindwall and Whelan [2] and National Baromedical Services [3]
Indications:
|
Topics
|
Sample Physician Order
|
HBO request requirements checklist and sample EMR documentation |
|
Acute Exceptional Blood Loss Anemia
|
|
- |
|
Acute Peripheral Ischemia / Crush Injury (with no associated ischemia-reperfusion component)
|
/
|
- |
|
Chronic Refractory Osteomyelitis
|
|
|
|
Compromised Skin Flaps & Grafts, digit/limb replantation
|
|
|
|
Diabetic Foot Ulcer - Hyperbaric Oxygen Therapy
|
|
|
|
Soft Tissue Radionecrosis
|
|
|
|
Pyogenic and Invasive Fungal Intracranial Abscesses
|
|
-
|
Table 3: 90 minutes oxygen breathing at 2.5 ATA with 2 air breaks
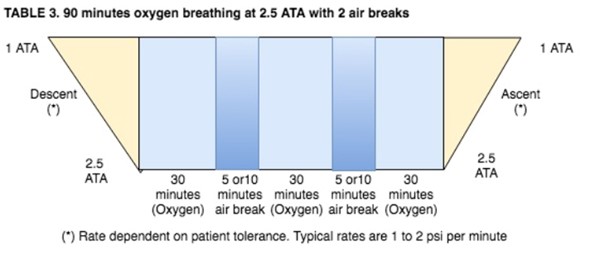
Table 3 based on Kindwall and Whelan [2] and National Baromedical Services [3]
Indications:
|
Topics
|
Sample Physician Order
|
HBO request requirements checklist and sample EMR documentation |
|
Acute Peripheral Ischemia / Crush Injury (involving ischemia- reperfusion component)
|
/
|
- |
|
Acute Retinal Artery Insufficiency (including central and partial retinal occlusion, arterial branch occlusion and central retinal vein occlusion)
|
|
- |
|
Chronic Refractory Osteomyelitis
|
|
|
|
Compromised Skin Flaps & Grafts (includes limb/digit replantation)
|
|
|
|
Osteoradionecrosis - Mandibular
|
|
|
|
Late Radiation Tissue Injury – Prophylaxis (complications of radiation therapy) not covered by Medicare
|
|
-
|
|
Necrotizing Soft Tissue Infections and Fournier's Gangrene
|
|
- |
|
Pyogenic and Invasive Fungal Intracranial Abscesses
|
|
-
|
|
Idiopathic Sudden Sensorineural Hearing Loss
|
|
-
|
Table 4a: 90 minutes oxygen breathing at 3 ATA with 2 air breaks
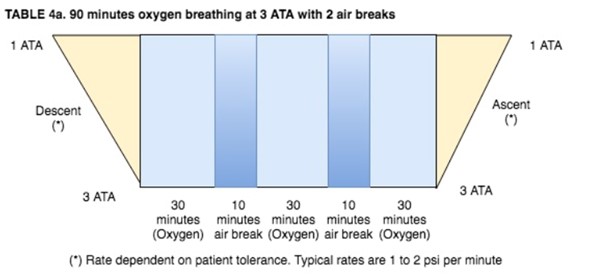
Table 4a based on Kindwall and Whelan [2] and National Baromedical Services [3]
Indications:
|
Topics
|
Sample Physician Order
|
HBO request requirements checklist and sample EMR documentation |
|
Acute Carbon Monoxide Poisoning
|
|
-
|
|
Clostridial Myonecrosis (Gas Gangrene)
|
|
-
|
Table 4b: Weaver Protocols for Carbon Monoxide Poisoning
Table 4b based on Weaver et al [4]
Table V
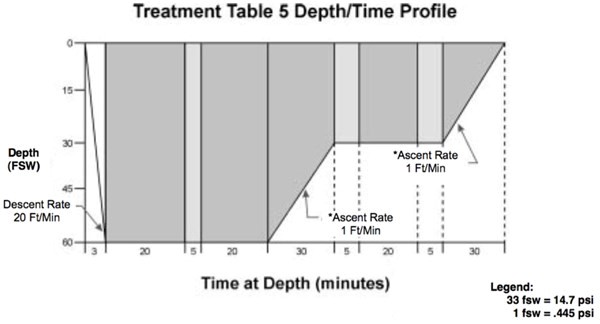
Adapted from the U.S. Navy Diving Manual [5]
- Descent Rate – 20 ft/min.
- Ascent Rate – Not to exceed 1 ft/min. Do not compensate for slower ascent rates. Compensate for faster rates by halting the ascent.
- Time on oxygen begins on arrival at 60 feet.
- If oxygen breathing must be interrupted because of CNS Oxygen Toxicity, allow 15 minutes after the reaction has entirely subsided and resume schedule at point of interruption
- Treatment Table may be extended two oxygen-breathing periods at the 30-foot stop. No air break required between oxygen-breathing periods or prior to ascent.
- Tender breathes 100% O2 during ascent from the 30-foot stop to the surface. If the tender had a previous hyperbaric exposure in the previous 12 hours, an additional 20 minutes of oxygen breathing is required prior to ascent.
Note: In a hyperbaric monoplace chamber operating on psi measurements, decompress at a rate of: 1 psi/2 min
- 30 fsw = 13.3 psi (1.9 ATA)
- 60 fsw = 26.7 psi (2.8 ATA)
Table VI
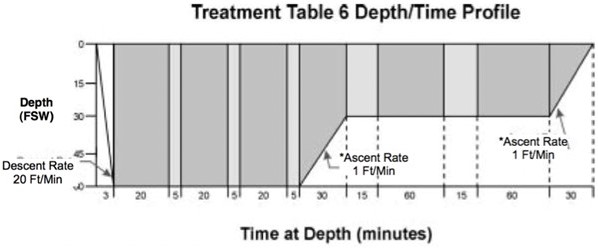
Adapted from the U.S. Navy Diving Manual [5]
- Descent Rate – 20 ft/min.
- Ascent Rate – Not to exceed 1 ft/min. Do not compensate for slower ascent rates. Compensate for faster rates by halting the ascent.
- Time on oxygen begins on arrival at 60 feet.
- If oxygen breathing must be interrupted because of CNS Oxygen Toxicity, allow 15 minutes after the reaction has entirely subsided and resume schedule at point of interruption
- Table 6 can be lengthened up to 2 additional 25-minute periods at 60 feet (20 minutes on oxygen and 5 minutes on air), or up to 2 additional 75-minute periods at 30 feet (15 minutes on air and 60 minutes on oxygen), or both.
- Tender breathes 100% O2 during the last 30 minutes at 30 fsw and during ascent to the surface for an unmodified table or where there has been only a single extension at 30 or 60 feet. If there has been more than one extension, the O2 breathing at 30 feet is increased to 60 minutes. If the tender had a hyperbaric exposure within the past 12 hours, an additional 60-minute O2 period is taken at 30 feet.
Note: In a hyperbaric monoplace chamber operating on psi measurements, decompress at a rate of: 1 psi/2 min
- 30 fsw = 13.3 psi (1.9 ATA)
- 60 fsw = 26.7 psi (2.8 ATA)
By Threshold Level
For a separate view of the table below, along with the treatment tables, see HBO Threshold Levels
|
Indications
|
Threshold Levels
|
| |
Lower Limit
|
Upper Limit / Utilization Review
|
|
Elective - Chronic
|
|
|
|
Chronic Refractory Osteomyelitis
|
20*
|
30-40‡
|
|
Diabetic Foot Ulcer
|
14
|
40
|
|
Pyogenic and Invasive Fungal Intracranial Abscesses
|
5
|
20‡
|
|
Late Radiation Tissue Injury Prophylaxis
|
20*
|
30‡
|
|
Mandibular Osteoradionecrosis
|
30*
|
60‡
|
|
Preparation of Wounds for Grafting
|
10
|
30‡
|
|
Problem Wound Support
|
14
|
30‡
|
|
Soft Tissue Radiation Injury
|
20*
|
60‡
|
|
Emergent – Acute
|
|
|
|
Acute Carbon Monoxide Poisoning
|
|
5‡
|
|
Acute Exceptional Blood Loss Anemia
|
Until satisfactory hematocrit or pt. stable, asymptomatic,
or transfusion becomes possible
|
|
Acute Peripheral Ischemia, Crush Injury and Compartment Syndrome
|
3*
|
14‡
|
|
Acute Retinal Artery Insufficiency
|
|
**‡
|
|
Acute Thermal Burns
|
5*
|
30‡
|
|
Arterial Gas Embolism
|
|
10‡
|
|
Clostridial Myonecrosis (Gas Gangrene)
|
5*
|
10‡
|
|
Compromised Skin Grafts and Flaps (Includes limb/digit replantation)
|
6*
|
20‡
|
|
Decompression Illness
|
|
10‡
|
|
Necrotizing Soft Tissue Infections and Fournier's Gangrene
|
5*
|
30‡
|
| Idiopathic Sudden Sensorineural Hearing loss |
1 |
20 |
* If the patient receives less than the indicated lower treatment threshold, a case audit is to be undertaken. For these disorders, too few treatments may be unlikely to have sufficient therapeutic effect and potentially waste resources. Reasons for early termination of HBO therapy may include: death; misdiagnosis; non-compliance; deterioration, or failure to perceive improvement.
** For patients treated more than three days after clinical plateau.
‡ Recommendations of the Undersea and Hyperbaric Medical Society, Hyperbaric Oxygen therapy Indications 13th Edition, 2014.
HYPERBARIC CPT CODES
- 99183 Physician or other qualified health care professional attendance and supervision of hyperbaric oxygen therapy, per session (PROFESSIONAL CHARGE)
- G0277 Hyperbaric oxygen under pressure, full body chamber, per 30 minute intervaL (FACILITY CHARGE)
TREATMENT
Evidence-based indications accepted by the UHMS, approved by Medicare
Elective – Chronic Indications
-
Chronic Refractory Osteomyelitis
-
Diabetic Foot Ulcer - Hyperbaric Oxygen Therapy
-
Osteoradionecrosis - Mandibular
-
Soft Tissue Radiation Injury
Emergent/Urgent – Acute Indications
-
Acute Carbon Monoxide Poisoning
-
Acute Traumatic Peripheral Ischemias
- Crush Injury
-
Acute peripheral arterial insufficiency
-
Arterial Gas Embolism
-
Clostridial Myonecrosis (Gas Gangrene)
-
Compromised Skin Grafts and Flaps, digit/limb replantation
-
Decompression Illness
-
Necrotizing Soft Tissue Infections and Fournier's Gangrene
Evidence-based indications accepted by the UHMS, NOT approved by Medicare
Elective – Chronic Indications
-
Pyogenic and Invasive Fungal Intracranial Abscesses
- Avascular Necrosis (Aseptic Osteonecrosis)
- Problem Wound Support
-
Late Radiation Tissue Prophylaxis
Emergent/Urgent – Acute Indications
-
Acute Exceptional Blood Loss Anemia
-
Acute Retinal Artery Insufficiency
- Acute Thermal Burns
-
Idiopathic Sudden Sensorineural Hearing Loss
Official reprint from WoundReference® woundreference.com ©2026 Wound Reference, Inc. All Rights Reserved
NOTE: This is a controlled document. This document is not a substitute for proper training, experience, and exercising of professional judgment. While every effort has been made to ensure the accuracy of the contents, neither the authors nor the Wound Reference, Inc. give any guarantee as to the accuracy of the information contained in them nor accept any liability, with respect to loss, damage, injury or expense arising from any such errors or omissions in the contents of the work.