CLINICAL
Overview
This topic addresses the clinical use, safety and selection of local anesthetics and local anesthesia techniques used to provide anesthesia prior to procedures commonly performed in wound care (e.g. wound debridement, wound biopsy).
Background
Definitions
-
Local anesthesia: refers to a temporary, reversible loss of sensation in a defined area of the body, often induced by the application of local anesthetics.
-
Local anesthetics: local anesthetics are medications that are warranted when a clinical procedure causes pain that could be eliminated by their use.[1]
Relevance
- Use of local anesthesia increases patient comfort and facilitates patient cooperation during procedures.[1]
- In wound management, procedures such as wound debridement, biopsy or abscess drainage often inflict pain and discomfort and thus the use of local anesthetics should be considered. A common misconception is to assume that patients with diabetic peripheral neuropathy or with spinal cord injury would not benefit from the use of local anesthetics prior to such procedures:
- Neuropathic symptoms can be both positive or negative, that is, patients with positive symptoms usually report burning or shooting pain, electrical or sharp sensations, or an exaggerated response to painful stimuli.[2]
- Patients with spinal cord injury may present with autonomic dysreflexia, an abnormal, overreaction of the involuntary (autonomic) nervous system to stimulation, such as pain. This reaction may include change in heart rate, excessive sweating, increase in blood pressure and muscle spasms.[3]
Care Setting
- Topical anesthetic application or subcutaneous infiltration of local anesthetic may be performed in several care settings, including inpatient hospital, outpatient hospital, home health, skilled nursing facilities and others, according to each facility's policies and procedures.[4]
Scope of Practice
Local anesthetic agents infiltration
- For registered nurses (RNs) and licensed practical nurses (LPNs) in the United States, guidance on scope of practice is provided by each state's Board of Nursing. Infiltration of local anesthetic agents (intradermal, subcutaneous, and submucosal) for the purposes of analgesia and/or anesthesia prior to potentially painful procedures falls within the scope of practice of RNs and LPNs in several states. Clinicians should consult their respective Boards.
- For nurse practitioners, physician assistants and physicians practicing in the United States, infiltration of local anesthetic agents falls within respective scopes of practice.[5]
Mechanism of Action of Local Anesthetic Agents
- Mechanism of action: local anesthetics block the conduction of nerve impulses by binding to specific receptors within nerve voltage-gated sodium channels in their inactive state, preventing sodium passage through these channels. Local anesthetic effects end when the substance is diffused away from the nerve membrane.[6][7][8]
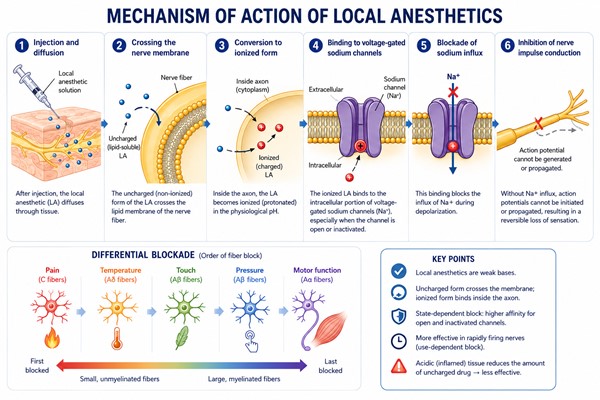
Fig. 1. Mechanism of action of local anesthetics
Types of Local Anesthetic Agents
Tables 1 and 2 list local anesthetics commonly used in the office care setting or facility outside of ambulatory surgical centers and hospital settings.[4] Many local anesthetics fall into two general chemical classes, amino amides and amino esters.
Table 1. Anesthetics for local infiltration
Anesthetic (common brands) | Onset (min) | Duration (min) without epinephrine | Duration (min) with epinephrine
| Maximal recommended dose for adults without epinephrine
| Maximal recommended dose for adults with epinephrine
|
Amides
|
|
|
|
|
|
Articaine
| 2-4
| 30-120
| 60-240
| 5.0 mg/kg or 350 mg
| 7.0 mg/kg or 500 mg
|
Bupivacaine (Marcaine, Sensorcaine)
| 2-10
| 120-240
| 240-480
| 2.5 mg/kg or 175 mg
| 3.0 mg/kg or 225 mg
|
Etidocaine (Duranest)
| 3-5
| 200
| 240-360
| 4.5 mg/kg or 300 mg
| 6.5 mg/kg or 400 mg
|
Lidocaine (Xylocaine)
| <1
| 30-120
| 60-400
| 4.5 mg/kg or 300 mg
| 7.0 mg/kg or 500 mg
|
Mepivacaine (Carbocaine)
| 3-20
| 30-120
| 60-400
| 6.0 mg/kg or 400 mg
| 7.0 mg/kg or 550 mg
|
Prilocaine (Citanest)
| 5-6
| 30-120
| 60-400
| 7.0 mg/kg or 400 mg
| 10.0 mg/kg or 600 mg
|
Esters
|
|
|
|
|
|
Chloroprocaine (Nesacaine)
| 5-6
| 30-60
| N/A
| 11.0 mg/kg or 800 mg
| 14.0 mg/kg or 1000 mg
|
Procaine (Novocaine)
| 5 | 15-90
| 30-180
| 10.0 mg/kg
| 14.0 mg/kg
|
Tetracaine (Pontocaine)
| 7 | 120-240
| 240-480
| 2.0 mg/kg
| 2.0 mg/kg |
Table 2. Anesthetics for topical application
Anesthetic
| Onset (min)
| Duration (min)
| Special considerations
|
Benzocaine
| <5 | 15-45
| Methemoglobinemia possible
|
Cocaine
| 1-5
| 30-60
|
|
Dibucaine
| <5 | 15-45
| For mucous membranes
|
Dyclonine
| 2-10
| <60 | For mucous membranes but not conjunctiva
|
Lidocaine
| <2 | 30-45
|
|
Lidocaine/prilocaine eutectic mixture
| <60 | 60-120 after removal of occlusive dressing | Methemoglobinemia possible |
- Factors that affect local anesthetics:
- Duration: the duration of action of local anesthetics depends on the concentration of local anesthetic and the blood flow to the nerve fiber. Also, the higher the lipid solubility of the local anesthetic, the longer the duration of action and greater potency. Local anesthetics can cause varying degrees of vasodilation, which also affects their duration of action and side effect profile.[6]
- Onset: dispersion of the local anesthetic through the tissue occurs more slowly with if the anesthetic solution has an increased acidity or if the target tissue is infected.
- Use of additives for local infiltrative anesthesia:
- Sodium bicarbonate (buffering): evidence shows that the addition of sodium bicarbonate to local anesthetic in order to raise the pH (known as buffering) decreases patient pain by 20-40% during drug delivery via subcutaneous or intradermal infiltration compared to plain lidocaine with epinephrine.[4]
- Epinephrine (adrenaline): epinephrine is the most common vasoconstrictor used in conjunction with local anesthetics.[4] Vasoconstrictors play an important role in providing optimal local anesthesia in cutaneous procedures by slowing mobilization of the anesthetic and thereby prolonging its effect, reducing peak blood levels, and providing hemostasis.[4] The most commonly used concentrations of epinephrine for office-based procedures are 1:100,000 and 1:200,000.[4] Patients with chronic wounds often present with multiple comorbidities that may pose a contraindication to the use of epinephrine mixed in anesthetic solutions. See section 'Contraindications' below.
Clinical Pharmacology
Absorption of Local Anesthetics
Local anesthetics are commonly administered by topical application or local infiltration. While the duration of anesthesia depends primarily on the anesthetic agent and its interaction with nerve tissue, systemic absorption determines the risk of local anesthetic systemic toxicity (LAST). [7][8]
Topical Application
- The rate of absorption varies considerably depending on the application site.[7][8]
- Mucous membranes (e.g., oral, nasal, genital) are highly vascular and lack a keratinized barrier, resulting in rapid drug absorption and onset of anesthesia.
- Intact skin, on the other hand, requires topical application of an increased concentration of anesthetics to ensure permeation and analgesia. Effective dermal anesthesia requires formulations specifically designed for transdermal delivery (e.g., EMLA® cream, a eutectic mixture of lidocaine and prilocaine or 4% liposomal lidocaine gel), often applied under an occlusive dressing or film. [9]
- Open wounds or broken skin allow greater and less predictable systemic absorption, increasing the risk of toxicity. Product labeling should always be followed before applying topical anesthetics to open wounds.
- The depth and duration of topical anesthesia depend on:
- Application time
- Dermal blood flow
- Total dose applied
- Use of occlusion over the topical anesthesia.
Local Infiltration
- Following injection, systemic absorption is determined primarily by the vascularity of the injection site. More vascular tissues produce higher plasma drug concentrations and a greater risk of systemic toxicity.[7][8]
- Approximate order of systemic absorption (highest to lowest): Intravascular > Mucosal (tracheal/oral) > Intercostal > Epidural > Peripheral nerve blocks > Subcutaneous infiltration
- For most wound care and dermatologic procedures, subcutaneous infiltration produces relatively slow systemic absorption compared with injections into highly vascular tissues.
Factors Affecting Systemic Absorption
Table 3 summarizes factors that increase or decrease systemic absorption of local anesthetics. [7][8]
Table 3. Factors that Affect Systemic Absorption of Local Anesthetics. [7][8]
| Factor | Increases Systemic Absorption | Decreases Systemic Absorption |
| Site of injection | - Higher vascularity (e.g., intravenous, tracheal, intercostal)
- Application to open wound or broken skin, mucosal surfaces
- Larger treatment area
| - Lower vascularity (e.g., subcutaneous, sciatic)
- Application to intact skin
- Smaller treatment area
|
| Presence of additives | - Absence of vasoconstrictors (like epinephrine)
| - Addition of vasoconstrictors (e.g., epinephrine)
|
| Local anesthetic agent | | - More lipid-soluble, highly tissue-bound agents, which are retained in tissues longer and enter the circulation more slowly.
|
Tissue Distribution of Local Anesthetics
- After systemic absorption (i.e., entering the bloodstream), local anesthetics are rapidly distributed to highly perfused organs, including the brain, heart, liver, kidneys, and lungs. These organs are also the primary targets of LAST.[7][8]
- Drug distribution is influenced by:
- Tissue perfusion: Highly vascular organs receive the drug first.
- Lipid solubility and protein binding: More lipid-soluble anesthetics (e.g., bupivacaine) are retained longer in tissues and generally have a longer duration of action.
- Muscle mass: Skeletal muscle serves as the largest reservoir for redistribution because of its large tissue volume.
Metabolism of Local Anesthetics
- Local anesthetics are classified as esters or amides, which differ in how they are metabolized.[7][8]
- Ester local anesthetics (e.g., procaine, chloroprocaine, tetracaine, benzocaine):
- Rapidly hydrolyzed by plasma pseudocholinesterase (butyrylcholinesterase).
- Produce water-soluble metabolites that are excreted by the kidneys.
- Procaine and benzocaine are metabolized to para-aminobenzoic acid (PABA), which is associated with a higher incidence of allergic reactions than amide anesthetics.
- Amide local anesthetics (e.g. lidocaine, mepivacaine, prilocaine, bupivacaine, ropivacaine)
- Metabolized primarily by in the liver by hepatic cytochrome P450 enzymes.
- Hepatic impairment, reduced liver blood flow (e.g., cirrhosis, congestive heart failure), or repeated dosing can increase plasma concentrations and the risk of LAST.
Elimination/Excretion
- Following hepatic or plasma metabolism, metabolites are excreted primarily by the kidneys. Only a small fraction of unchanged local anesthetic is eliminated in the urine.[7][8]
Side Effects of Local Anesthetics
Local anesthetics are generally safe when used within recommended doses. Adverse effects may be local (at the site of administration) or systemic if sufficient drug enters the circulation, resulting in LAST. The risk of systemic toxicity increases with larger doses, highly vascular injection sites, intravascular injection, application to mucosal surfaces or large open wounds, and impaired drug metabolism. Recognizing early signs is crucial for immediate intervention. [7][8]
Local Side Effects (Injection/Application Site)
- These reactions typically occur at or near the site of administration [7][8]:
- Common reactions: pain, burning, or stinging upon administration; swelling or erythema; local tissue injury (if excessive concentration or inadvertent intravascular injection occurs).
- Specific observations: tissue blanching is common if epinephrine is present. Prolonged numbness or nerve injury/paresthesia can occur, though rare.
- Hypersensitivity: true allergies (IgE/IgG-mediated) are uncommon. Reactions are more frequently associated with ester-type agents (e.g., procaine, benzocaine) or preservatives in multidose amide preparations (e.g., methylparaben).
Local Anesthetic Systemic Toxicity (LAST)
- LAST is a rare but potentially life-threatening complication caused by excessive plasma concentrations of local anesthetic.[7][8]
- LAST occurs when systemic absorption exceeds metabolism, primarily affecting the Central Nervous System (CNS) and Cardiovascular System (CVS). CNS symptoms typically precede cardiovascular collapse.
- Early Warning Signs (Monitor closely):
- CNS: circumoral (around the mouth) numbness, metallic taste, tinnitus, dizziness, lightheadedness, blurred vision, anxiety, agitation, and tremor.
- CVS: tachycardia, palpitations, and initial hypertension (often due to epinephrine or CNS stimulation).
- Late/Severe Signs (Emergent):
- CNS: confusion, slurred speech, muscle twitching, seizures, loss of consciousness, and respiratory depression or arrest.
- CVS: bradycardia, hypotension, arrhythmias (e.g., wide QRS, ventricular tachycardia/fibrillation), cardiovascular collapse, and cardiac arrest.
Methemoglobinemia
- Prilocaine and benzocaine can rarely cause methemoglobinemia, particularly after topical application to mucosal surfaces or large treatment areas.
- Clinical features include: cyanosis unresponsive to supplemental oxygen, dyspnea, fatigue, headache, low pulse oximetry despite adequate oxygenation.
Clinical Considerations for Practice
- Cumulative risk: repeated topical applications (e.g., spraying lidocaine during debridement) increase the risk of cumulative systemic absorption.
- High-risk patient groups: caution is advised in patients with cardiovascular disease, liver dysfunction (reduced amide metabolism), or those taking medications that decrease hepatic blood flow.
- Emergency management: If LAST is suspected, stop administration immediately. Airway management and oxygenation are the highest priorities. Activate the emergency response system or call EMS.
- For cardiovascular toxicity related to potent agents like bupivacaine, lipid emulsion therapy is the recommended first-line treatment.
- If practicing in a facility where lipid emulsion therapy is available, follow institutional protocols for administration of 20% lipid emulsion.
- Refer to the American Society of Regional Anesthesia and Pain Medicine (ASRA) Local Anesthetic Systemic Toxicity Checklist.[10]
- Topical vs. injected: Topical anesthetics are not risk-free. Large treatment areas, prolonged application, occlusive dressings, and application to mucosa or open wounds can increase systemic absorption.[7][8] See Table 3.
Techniques for Local Anesthesia
This topic focuses on topical application and subcutaneous infiltration of local anesthetics but other techniques are also listed below for comparison purposes:
- Topical application (topical anesthesia): certain anesthetic agents can be applied topically on the skin or on the wound (Table 2). These agents have been developed to replace, augment or reduce the pain of local infiltration, and thus reduce patient apprehension.[1]
- Subcutaneous infiltration (local infiltrative anesthesia): this method induces anesthesia through direct infiltration of anesthetics through the skin or wound (Table 1). Procedures including skin biopsy, wound debridement, excision, wound closure, tissue rearrangement, skin grafting, cauterization, may all be successfully performed under local infiltrative anesthesia.[4]
- Direct infiltration: this technique is better suited for intact, uninfected skin or uninfected wounds. It involves local injection of anesthetics directly through an open wound or through intact skin in the procedure field (e.g. skin that will be biopsied). See Figure 2.
- Field block: heavily contaminated, infected wounds, skin abscesses or wounds that require manipulation prior to closure should undergo a field block. In this technique, the anesthetic solution is infiltrated around the border of the surgical field, leaving the operative area undisturbed.[11] As a result, onset of the anesthetic agent is not delayed by the increased acidity of infected tissue. In addition, an advantage of this technique is that there is no tissue distortion in the operative field, allowing for more precise tissue manipulation and reconstruction.[1] See Figure 3.
- Peripheral nerve block: useful when refers larger areas must be anesthetized; in these cases, local infiltration would require large doses of anesthetic.[11] In a nerve block, anesthetic is injected into the extra-neural or paraneural spaces, providing complete anesthesia in the region supplied by that nerve, distal to the site of injection.[11]
- Tumescent anesthesia: tumescent anesthesia is a specialized form of local anesthesia in which large volumes of dilute anesthetic are injected subcutaneously to produce swelling and firmness of the targeted areas.[4] It is used for liposuction and other plastic, cosmetic, and dermatological surgical procedures involving large areas of skin.
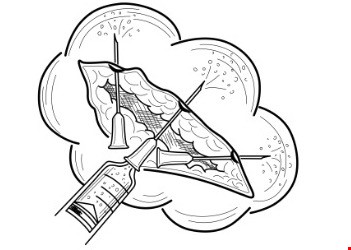
Fig 2. Subcutaneous infiltration of local anesthetic, direct infiltration | 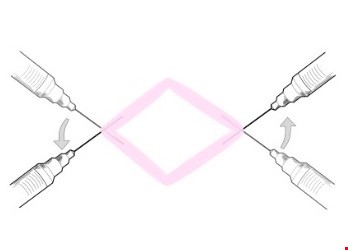 Fig 3. Subcutaneous infiltration of local anesthetic, field block Fig 3. Subcutaneous infiltration of local anesthetic, field block
|
Understanding Relevant Anatomy
The 3 layers of the skin are: epidermis, dermis, and subcutaneous fat layer or subcutis (Figure 4). For details, see section 'Skin Appendages and Nerves' in topic "The Skin".
- Input from free nerve endings (nociceptors) present in the epidermal and dermal layers are perceived as pain. Infiltration of local anesthetic into the subcutaneous layer prevents transmission of pain.
-
Because nerve endings are concentrated in the dermis, intradermal injections are more painful than sub-dermal injections.[12]
- Because of their orientation and concentration in the dermis, there is a lower probability that free nerve endings may be pierced causing pain if the needle is inserted perpendicularly to the skin (i.e. at 90 degrees perpendicular to the skin) as opposed to obliquely (e.g. at 45 degrees from the skin surface).[12]
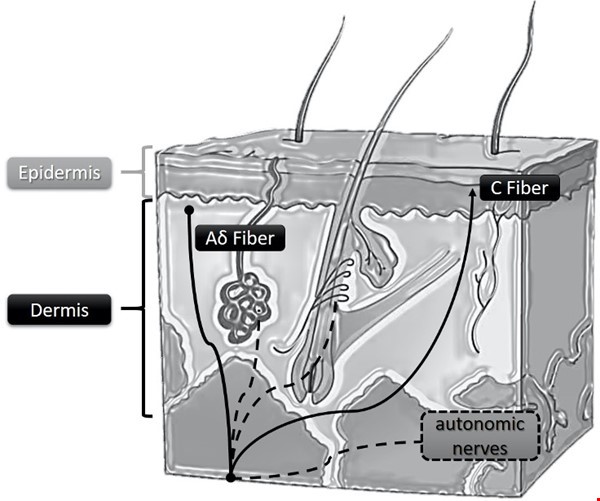
Fig. 4. Schematic of histological cut of the skin showing neural fibers. Aδ fibers: myelinated, respond to nociceptive stimuli such as cold and pressure (provide fast/first pain information). C fibers: unmyelinated, slowest neural impulse conduction, respond to temperature and pain stimuli (nociceptive).
General Indications and Contraindications
Indications
Topical anesthesia
- 2CFor minor skin procedures (e.g. skin biopsy, small excisions, minor debridements), clinical guidelines suggest the use of topical anesthesia prior to the procedure to minimize pain (Grade 2C).[4]
- 2CFor larger procedures (e.g. debridements), clinical guidelines suggest the use of topical anesthetic agents to lessen the pain of injection and reduce the dose of infiltration anesthesia (Grade 2C).[4]
- For pregnant or nursing women, a limited amount of topical lidocaine is safe for use, but there is insufficient evidence to recommend use of other topical anesthetics.[4]
- 1B2CFor children, guidelines recommend topical anesthesia as the first-line method for repair of dermal lacerations (Grade 1B) and other minor procedures (Grade 2C). [4]
Local infiltrative anesthesia
- Infiltrative anesthesia is safe and recommended for potentially painful procedures, such as obtaining a biopsy specimen, wound debridement, excision, wound closure, tissue rearrangement, skin grafting, cauterization, abscess drainage and foreign body removal from the skin.[4]
Contraindications
- Known allergies or sensitivities to a local anesthetic is a contraindication for use of that anesthetic or other agents with the same chemical classification (i.e. amide or ester; see Table 1).
- Allergy to lidocaine is rare, with a genuine immunologic reaction representing only 1% of all adverse reactions to these medications.[4]
- For multiple wounds or large wounds that require large amounts of local anesthetics such that the total dose needed for adequate effect is expected to reach the maximum allowable anesthetic dose, infiltration of local anesthetics is not recommended.
Addition of epinephrine
-
Patients with chronic wounds often present with multiple comorbidities that may pose a contraindication to the use of epinephrine mixed in anesthetic solutions. Addition of epinephrine is not recommended in the following cases [13]:
- For patients with underlying comorbidities that may be exacerbated by systemic epinephrine effects (e.g., hyperthyroidism, pheochromocytoma, severe hypertension, coronary artery disease)
- Local anesthesia of wounds on limbs if patients have compromised peripheral circulation (e.g. peripheral artery disease)
- Patients taking lurasidone (may cause hypotension), ergot alkaloids (enhanced hypertensive and vasoconstrictive effect)
- For patients taking the medications below, consider avoiding epinephrine or modifying therapy due to potential drug interaction:
-
Beta blockers
- Monoamine oxidase inhibitors
- Phenothiazines
- Tricyclic antidepressants
- 2BFor local anesthesia on the ear, nose, and digits in healthy individuals, clinical guidelines suggest the addition of epinephrine to local infiltration anesthesia to minimize use of anesthetics and decrease bleeding (Grade 2B).[4]
-
Rationale
: although clinicians historically maintained the idea that using vasoconstrictors in areas of skin served by terminal vessels would lead to necrosis, multiple systematic reviews and randomized controlled trials have found the addition of epinephrine to local infiltrative anesthesia at a concentration of 1:100,000 and 1:200,00 to be safe for use in the digits, hands, and feet of healthy individuals.[4] However as stated above, patients with chronic wounds often present with comorbidities that may pose a contraindication to the use of epinephrine in anesthetic solutions (e.g. peripheral artery disease).Therefore as a rule, it is suggested that clinicians do not keep anesthetics with epinephrine within reach when managing patients with nonhealing wounds, to avoid accidental infiltrations of solutions containing epinephrine and potential complications.
Complications and Side Effects
Topical application or local infiltrative anesthesia
- Adverse reaction to the anesthetic or to preservatives (e.g. methylparaben).[14]
- See section 'Side effects of Local Anesthetics' above.
Local infiltrative anesthesia
- Toxicity due to anesthetic overdose (eg, seizure, cardiac arrhythmias) or sympathomimetic effects due to epinephrine.[14]
- Intravascular injection of anesthetic/epinephrine
- Hematoma
- Spread of infection, by passing the needle through an infected area
Selection of Local Anesthesia for Wound Care
Several medications and techniques for local anesthesia are available. Selection of local anesthesia is primarily based on the experience and comfort level of each clinician, but is also influenced by patient factors including contraindications to any of the local anesthetic components, duration of the procedure, need for hemostasis, and others.[4]
Choice of technique for local anesthesia in wound care
- Prior to procedures that may cause pain and are commonly performed in wound management (e.g. wound debridement, biopsies, etc), clinicians might opt to start by applying topical anesthetics, and then provide further anesthesia by infiltrating anesthetics if the patient continues to feel pain or discomfort. Exceptions include:
- Wounds with extensive tunneling, in which application of topical anesthetic may fill up the tunneling. In those cases, removal of the topical anesthetic prior to the procedure may be challenging.
- If muscle, fascia or bone are visible on the wound bed, application of topical anesthetic on those tissues may not be necessary. However, application of topical anesthetic on the wound margin and periwound skin would help prevent/minimize pain, as free nerve endings (nociceptors) are present in the epidermal and dermal layers.
- For patients with spinal cord injury, clinicians might opt for local infiltrative anesthesia prior to a potentially painful procedure (e.g. pressure ulcer/injury debridement) in order to avoid autonomic dysreflexia.
Choice of local anesthetic agent in wound care
-
Choice of topical anesthetics: clinical guidelines recommend use of noncocaine formulations over cocaine formulations as the latter is associated with higher costs and increased potential for side effects.[4]
- For intact skin:
- EMLA:1 to 2 grams of cream is applied per 10-cm2 area of skin. Cover with occlusive dressing or transparent film.[8]
- 4% liposomal lidocaine gel (e.g. Topicaine ): apply a moderately thick layer, approximately 1/8 inch thick, maximum of 5g. Cover with occlusive dressing or transparent film.[8]
- For chronic wounds, 2-5% lidocaine gel, viscous or cream applied topically have been shown to be safe and effective in reducing pain prior to debridement. Onset is typically within 3-5 minutes.[15][16][17]
-
Choice of anesthetic for local infiltration:
- For most patients with chronic wounds, clinicians might opt for buffered 1-2% lidocaine without epinephrine as the local anesthetic of choice for local infiltrative anesthesia.
- Many patients with chronic wounds present with comorbidities (e.g. peripheral artery disease) that may pose a contraindication to the use of epinephrine in anesthetic solutions for local infiltrative anesthesia.
- For patients with true allergy to lidocaine, clinical guidelines suggest use of either ester-type local anesthetics as an alternate form of local infiltration anesthesia.[4]
HOW TO ADMINISTER LOCAL ANESTHESIA FOR WOUND CARE PROCEDURES
Assessment
- Prior to administering local anesthesia for wound care procedures, it is important that a comprehensive patient and wound assessment be performed. See topic "How to Assess a Patient with Chronic Wounds" and "How to Determine Healability of a Chronic Wound".
- Specifically, it is important to investigate whether the patient has any history of allergies or adverse reactions to local anesthesia. Patients with history of severe reactions suggestive of anaphylaxis should not receive any local anesthetics until they undergo an evaluation by an allergy specialist.
Procedure: application of topical anesthetic
Tables 4 below illustrate steps for application of topical anesthetics in wound care. The doses and methods of application may vary for different patients and medications (see Table 1). The step-by-step below refers to the topical application of lidocaine.[15][18]
Table 4. Procedure
|
Steps
|
Rationale/ Tips
|
|
1. Perform hand hygiene, don clean procedure gloves. Remove previous wound dressing
|
|
2. Gently cleanse skin and wound with sterile saline or water to remove debris if any
|
|
|
3. Gently dry with a piece of gauze
|
|
4. Apply a thick layer of the topical anesthetic (if gel or cream), cover the wound to the thickness of a dime - For intact skin:
- EMLA: 1 to 2 grams of cream is applied per 10-cm2 area of skin.
- 4% liposomal lidocaine gel (e.g. Topicaine ): apply a moderately thick layer, approximately 1/8 inch thick, maximum of 5g.
- Cover with occlusive dressing or transparent film.[8]
|
- For wounds with tunneling, avoid applying topical anesthetic through tunneling, as it might be difficult to remove it
- EMLA cream should not be used on mucous membranes, broken skin, infants younger than 1 month of age, or patients with a contraindication to either lidocaine or prilocaine.[8]
|
|
5. Wait for 4 to 15 minutes and test for pain sensation - For intact skin: wait longer and test for pain sensation.
- EMLA: 1 hour under an occlusive dressing.[8]
- 4% liposomal lidocaine gel : 5-10 minutes onset, and about 30-60 minutes duration.
|
|
6. If anesthesia is incomplete, give supplementary local infiltration anesthesia through the partially anesthetized wound edges (usually resulting in only minimal pain).
|
|
Procedure: subcutaneous infiltration of local anesthetic (local infiltrative anesthesia)
Table 5 below illustrates steps for subcutaneous infiltration of local anesthetics in wound care.[4][12][14] Doses and methods of application may vary for different patients and medications (see Table 1).
Table 5. Procedure
|
Steps
|
Rationale/Tips
|
1. Determine patient history of allergies or sensitivities which may contraindicate product use.
|
|
2. Obtain patient’s consent per facility policy
|
|
3. Obtain provider's order (including medication, dosage range and site of injection)
|
|
4. Ensure adequate assistance, supplies, and equipment: - Appropriate lighting
- Assistive equipment/ additional personnel for positioning
- Personal protective equipment (PPE) as indicated: clean gloves, eyewear, mask, cap and gown
- Wound cleansing solution (e.g. normal saline, lactate ringer, hypochlorous acid, surfactants, potable water)
- Syringe (e.g., 1 to 10 mL) and needle (e.g., 25 to 33 gauge) for anesthetic injection
- Injectable local anesthetic (e.g, 1% lidocaine without epinephrine)
- Instruments for the wound care procedure (e.g. debridement, biopsy)
|
Maximum dose of local anesthetics (see Table 1): - Lidocaine without epinephrine, 4.5 mg/kg or 300 mg; lidocaine with epinephrine, 7 mg/kg or 500 mg.
- NOTE: A 1% solution (of any substance) represents 10 mg/mL (1 g/100 mL)
For intact skin: To minimize infiltration pain consider: - Small needle gauge: consider a 30G or 33G needle.
- Small initial syringe size: consider starting with a 1 mL syringe, then transition to a 3 mL syringe.
- Buffering: use 1 mL of 8.4% bicarbonate with each 10 mL of lidocaine with 1:100,000 epinephrine. [19][20]
|
5. Position the patient comfortably and ensure wound is exposed and visible.
| - While positioning, explain the procedure to the patient and let the patient know that they may feel a burning sensation at first, before the area becomes anesthetized
|
| 5a. Apply topical anesthetic on the periwound skin to minimize injection pain (see Table 4 above) |
|
6. Open supplies onto separate surface or tray, in an area independent of patient or clinician movement.
|
- Tools should never be placed on an unstable surface, such as the patient; this could potentially cause injury.
|
7. Examine the neurovascular structures distal to the wound.
| - Document any preexisting nerve deficit distal to the wound before doing anesthetic infiltration.
|
8. Perform hand hygiene, and don clean gloves.
|
|
9. If a topical anesthetic has been used prior to the infiltration, remove it with dry gauze.
| - If needed, change gloves after removal of topical anesthetic
|
10. Cleanse the skin from the wound edges outward, making several outwardly expanding circles. - Cleanse the wound with a non-cytotoxic cleanser such as normal saline, hypochlorous acid, or potable water (do not use antiseptics). Pat dry with sterile gauze
| - Do not apply antiseptics for surgical skin preparation (i.e. 2-4% chlorhexidine, povidone-iodine, alcohol) directly into the wound because many are toxic to tissues and may interfere with wound healing.[21] Of note, more diluted versions of antiseptics have been designed for wound cleansing.[22]
- Consider anesthetizing wounds before cleansing and irrigating if cleansing is expected to be overly painful
|
11. Local infiltration anesthesia - For open wounds:
- Insert the needle directly into the exposed subcutaneous layer of the wound bed/ wound edge (i.e., do not insert the needle through the skin) and advance the needle to the margin of the wound.
- Aspirate to rule out intravascular placement and then slowly inject the anesthetic while withdrawing the needle.
- Redirect the already injected needle into unanesthetized skin to maximize the area anesthetized with a single needlestick.
- Continue to anesthetize, covering the entire wound circumference.
- For grossly contaminated or infected wounds:
- Consider injecting instead percutaneously through the intact, uninfected (or otherwise disinfected) skin around the wound (field block, see section above 'Techniques for Local Anesthesia')
- For intact skin [20][19]:
- Insert a smaller needle (e.g, 27-gauge for hand injection and 30-gauge for face injection) at 90 degrees perpendicular to the skin.
- Inject slowly. Advance the needle only within anesthetized tissue.
| To minimize infiltration pain: - For open wounds: to minimize pain in open wounds, consider starting from the center of the wound bed and working outwards, leaving wound edge and intact skin as the last areas to infiltrate.
- For intact skin: to decrease the pain of local anesthetic injection, consider buffering the anesthetic (if lidocaine), slow rate of infiltration (e.g. 30-60 seconds), vibration of the skin, use of a warm solution, or cold air skin cooling.[4]
- Consider inserting the needle at 90 degrees perpendicular to the skin instead of a 45-degree angle.[12]
- Inject the local anesthetic slowly before advancing the needle. Maintain a small wheal (approximately 5 mm) of anesthetized tissue ahead of the needle tip, so the needle advances only through tissue that is already numb after the initial skin puncture. Slow injection allows the anesthetic time to diffuse and take effect, improving patient comfort throughout the procedure. [19][20]
|
12. Allow several minutes for the anesthetic to take effect. You may gently massage the overlying skin with your fingertip to facilitate spread of the anesthetic in the tissues. | - Onset of lidocaine: < 1 minute; see Table 1
|
| 13. Once anesthetized, initiate the procedure |
- Test sensation of the infiltrated area prior to initiating the procedure
|
Videos: How to Administer Local Anesthesia for Wound Care Procedures
Video 1. Use of topical anesthetic prior to conservative sharp wound debridement. By Scott Robinson, MD
Video 2. Use of local infiltrative anesthesia prior to wound biopsy. By Scott Robinson, MD
Documentation
Documentation should include:
- History of any allergies or adverse reactions to local anesthetic(s)
- Previously existing nerve damage distal to the anesthetized area
- Type and dose of local anesthetic(s) used
- Techniques used for local anesthesia
- Document procedure and patient tolerance
- Patient confirmation that the area was anesthetized prior to initiating the intervention
- Any adverse reactions or complications from local anesthesia
TROUBLESHOOTING
Pain upon infiltration
Strategies to reduce injection pain include [20]:
- Optimization of injection technique:
- Use the smallest appropriate needle (typically 30–33 gauge).
- Use small-volume syringes (1–3 mL) to improve injection control.
- Buffer lidocaine with sodium bicarbonate (typically 1 part 8.4% sodium bicarbonate to 10 parts 1% lidocaine) to reduce the burning sensation.
- Inject slowly ("blow slow before you go"), maintaining a small wheal of anesthetized tissue ahead of the advancing needle.
- Insert the needle perpendicular (90°) to the skin for the initial puncture when appropriate.
- Prefer subcutaneous infiltration rather than intradermal injection when clinically feasible, as it is generally less painful.
- Aspirate before injection when appropriate to avoid inadvertent intravascular administration.
- Patient comfort measures:
- Warm the anesthetic solution to room or body temperature before injection.
- Apply vibration, cold (ice), or other counter-stimulation techniques near the injection site.
- Use verbal reassurance and distraction ("talkesthesia") or music to reduce pain perception and anxiety.
Side effects of local anesthetics
See section 'Side Effects of Local Anesthetics' above.
Hypersensitivity/ Allergic Reactions
True allergic reactions to local anesthetics are rare (<1%), particularly with amide anesthetics (e.g., lidocaine, bupivacaine). Ester anesthetics (e.g., procaine, benzocaine) are more likely to cause hypersensitivity because they are metabolized to para-aminobenzoic acid (PABA). Reactions may also result from preservatives (e.g., methylparaben) or other additives rather than the anesthetic itself. Identifying an allergic reaction typically involves a thorough patient history, assessment of clinical symptoms, and, if necessary, allergy testing.[9]
- Symptoms range from mild to life-threatening and may include:
- Localized urticaria, pruritus, or erythematous rash
- Angioedema
- Wheezing or bronchospasm
- Hypotension
- Anaphylaxis (rare)
- Management:
- Stop administration of the local anesthetic immediately.
- Assess the patient's airway, breathing, and circulation.
- Treat mild reactions with appropriate symptomatic therapy (e.g., antihistamines).
- If anaphylaxis is suspected, administer intramuscular epinephrine promptly, activate emergency medical services, and provide supportive care according to current anaphylaxis guidelines.
- Document the suspected reaction and refer the patient for allergy evaluation before future procedures if the diagnosis is uncertain.
- Prevention:
- Obtain a history of previous reactions to local anesthetics, preservatives, or sulfites before the procedure.
- Distinguish documented allergy from prior vasovagal episodes or toxic reactions.
- Consider preservative-free formulations or referral for allergy testing when a true local anesthetic allergy is suspected but future procedures requiring local anesthesia are anticipated.
Local Anesthetic Systemic Toxicity (LAST)
LAST is a rare but potentially life-threatening complication caused by excessive systemic absorption or inadvertent intravascular injection of local anesthetics. Risk increases with larger doses, highly vascular injection sites, and application to mucosal surfaces or large open wounds. Early recognition and prompt intervention are critical.
- Symptoms:
- Circumoral numbness, tinnitus, metallic taste, and dizziness are classic early neurologic manifestations of LAST.
- Early recognition allows intervention before progression to seizures or cardiovascular collapse.
- Management:
- Stop local anesthetic administration immediately.
- Assess airway, breathing, and circulation.
- Administer supplemental oxygen and provide supportive care.
- Activate the emergency response system or call EMS.
- Monitor for seizures and cardiovascular instability.
- If practicing in a facility where lipid emulsion therapy is available, follow institutional protocols for administration of 20% lipid emulsion.
- Refer to the American Society of Regional Anesthesia and Pain Medicine (ASRA) Local Anesthetic Systemic Toxicity Checklist. [10]
- Prevention:
- Use the lowest effective dose.
- Calculate the maximum recommended dose before injection.
- Aspirate before injection whenever appropriate.
- Inject incrementally and slowly.
- Consider adding epinephrine, when appropriate, to reduce systemic absorption.
- Exercise extra caution when treating large wounds, highly vascular tissues, or mucosal surfaces.
CASE STUDIES
Box 1. provides sample case studies for wound care clinicians.
Box 1. Local anesthetics case studies for wound care clinicians. [8]
Case 1. Optimizing Local Anesthesia for Sharp DebridementA 68-year-old woman with chronic venous insufficiency presents with a 4 × 5 cm painful venous leg ulcer on the medial lower leg. The wound contains adherent fibrin and nonviable tissue requiring sharp debridement. She rates her pain as 8/10 and reports that previous injections of lidocaine were "more painful than the procedure itself." Her medical history includes hypertension and well-controlled type 2 diabetes. She has no known drug allergies. Clinical Question 1: Which strategy is most likely to reduce discomfort during local anesthetic infiltration? - Use buffered lidocaine, inject slowly, and maintain a small wheal of anesthetized tissue ahead of the advancing needle.
- Rationale: Slow infiltration, buffered lidocaine, and the "blow slow before you go" technique significantly reduce injection pain. Using a small-gauge needle (30–33 G), warming the anesthetic, and advancing the needle only through previously anesthetized tissue further improve patient comfort.
Clinical Question 2: Which additional measures may further reduce injection pain? - Several nonpharmacologic interventions - including warming the anesthetic, vibration, cold, music, and verbal distraction ("talkesthesia") - have been shown to reduce pain perception during local anesthetic administration.
Case 2. Recognizing Local Anesthetic Systemic Toxicity (LAST)A 72-year-old man undergoes extensive sharp debridement of a large circumferential venous leg ulcer. Because of significant procedural pain, multiple infiltrations of lidocaine are administered around the wound. Approximately 2 minutes after the final injection, the patient reports ringing in the ears, a metallic taste, numbness around the mouth and increasing dizziness. His blood pressure is 148/86 mmHg, heart rate is 102 beats/min, and he remains awake and oriented. Clinical Question 1: What is the most likely diagnosis? - Early local anesthetic systemic toxicity (LAST). Circumoral numbness, tinnitus, metallic taste, and dizziness are classic early neurologic manifestations of LAST. Early recognition allows intervention before progression to seizures or cardiovascular collapse.
Clinical Question 2: What is the most appropriate immediate action? - Stop administering the local anesthetic, assess airway, breathing, and circulation, and activate emergency response.
- Rationale: Early neurologic symptoms are often the first warning signs of LAST. Stop injecting immediately if the patient develops circumoral numbness, tinnitus, metallic taste, dizziness, agitation, or confusion. Prompt recognition and intervention can prevent progression to seizures and cardiovascular collapse. Immediately discontinue local anesthetic administration, assess airway, breathing, and circulation, administer supplemental oxygen and provide supportive care, and activate the emergency response system or call EMS.
Clinical Question 3: How can LAST be prevented? - Prevention Strategies to reduce the risk of LAST:
- Use the lowest effective dose.
- Calculate the maximum recommended dose before injection.
- Aspirate before injection whenever appropriate.
- Inject incrementally and slowly.
- Consider adding epinephrine, when appropriate, to reduce systemic absorption.
- Exercise extra caution when treating large wounds, highly vascular tissues, or mucosal surfaces.
|