CLINICAL
Overview
Unna Boot, also known as Unna's Boot (UB) or paste boot, is an inelastic bandage that is frequently used in compression therapy to treat venous leg ulcers (VLU). This topic focuses on application of UB. For a review on compression therapy and other types of compression devices, see topic "Compression Therapy". For guidance on selecting compression pressure level, see "How to Select Adequate Compression Therapy Pressure Levels and Products". For examples of different brands, see "Compression Brands Quick Reference".
Background
- Compression therapy is considered the mainstay of VLU treatment. Along with standard care it has the potential to heal 50%-75% of VLUs.[2][3]
- Adequate compression can be achieved by several methods, for instance by using a single component/layer (such as a compression stocking or one type of bandage) or by using multiple components/layers (different types of bandages or stockings and bandages used together).[2][4] Overall, evidence shows that multi-component systems are more effective than single-component systems. High compression is more effective than low compression, but among different types of high compression no clear differences have been observed.[2] See different types of compression therapy devices in section 'Types of Compression Therapy Devices' in topic "Compression Therapy".
- Prior to compression therapy, all patients who are candidates for compression therapy should be assessed for concomitant peripheral artery disease (PAD) with a noninvasive arterial assessment, such as ankle brachial index (ABI), doppler waveform or toe brachial index (TBI).[5] Assessment of arterial blood supply with these tests is a major determinant of the pressure level of compression to be applied.[5] See topic "How to Interpret Audible Handheld Doppler Ultrasound and Waveforms to Rule out PAD".
- If PAD is suspected and noninvasive arterial assessment (e.g. ABI, doppler waveform, TBI) cannot be performed right away, compression with low modified pressure (e.g. tubular dressings) may be applied until arterial assessment is completed. See 'Algorithms' in topic "How to Select Adequate Compression Therapy Pressure Levels and Products".
Definition
- Unna Boot (UB): classified as a non-stretch, inelastic compression bandage, an UB is an impregnated bandage that was originally developed by the German dermatologist Paul Gerson Unna in 1885.[6][7]
- To improve upon the poorly tolerated compression bandages for treatment of VLU of his era, Unna initially developed a single layer, special gauze bandage impregnated with a mixture of 15% zinc oxide in a glycogelatin-based paste, which allows for drying and cooling effects as well as antipruritic effects.[6][7] Following experimentation with various types of bandages, Unna introduced a new skin-matched compression bandage at the Third International Congress of Dermatology in London in 1896.[8] In 1910, Unna's disciple, Heinrich Fischer, introduced the Fischer bandage, which is an UB applied snugly with a short-stretch bandage layered over it.[6] Unna's method gained widespread recognition for its efficacy and ease of use, leading to its adoption and subsequent commercialization by several companies in the early 20th century.[6]
- How it works: the zinc paste bandage (UB) acts as an inelastic, semi-rigid mold around the leg (i.e., low resting pressure). When the patient walks, the mold offers resistance and counteracts calf muscle movement, increasing venous return (i.e., increased working pressure).[9]
- Commercially available UBs:
- Nowadays, commercially available zinc paste bandage (UB) brands include Viscopaste, Gelocast, Primer Unna Boot. Manufacturers also carry kits that include a zinc paste bandage (UB), and an outer layer, such as self-adhering elastic bandage (e.g. Unna-FLEX® Compression Bandage Convenience Pack). In addition, some manufacturers have developed variations of the original UB, with bandages made of other materials impregnated with zinc (e.g., CoFlex® TLC Zinc Lite, Unna-FLEX® Elastic Unna Boot).
- For commercially available kits that include a zinc paste bandage (UB), it is advisable that clinicians check with manufacturers in regards to resulting working pressure, distribution of pressure and stiffness. For more information on types of compression devices, their stiffness and indications, see section 'Types of compression therapy devices' in topic "Compression Therapy". Commercially available kits that include a zinc paste bandage (UB) are typically as a 2 or more layer bandage system [9][10]:
- Inner layer: rolled gauze bandage impregnated with zinc oxide, calamine, glycerin, sorbitol gelatin or magnesium aluminum silicate, applied from the forefoot to just below the knee.
- Intermediate layer(s): continuous gauze dressing. Cast padding may be applied on top of inner layer for padding of bony prominences or to absorb wound exudate. Some products do not offer this layer, while others provide compression in this layer (please refer to the manufacturer's product insert).
- Outer layer: typically a self-adherent elastic wrap applied with graded compression, tubular dressing (i.e. stockinette) or short-stretch bandage
Relevance
- Application of UB is one of the most common clinic procedures billed to Medicare. A 2019 study showed that it was among the top ten most performed procedures by a large multi-regional health care system in the U.S.[1]
Skills and Education
- A physician/Qualified Healthcare Professional (QHP) order is needed to apply an UB in the U.S. and other countries.
- Clinicians applying an UB should be trained and competent in application of compression therapy bandages including UB.
General Indications and Contraindications
Indications
UB is indicated:
- For ambulatory patients with venous insufficiency and/or VLUs who presents with one of the following [3][11][12]:
- Open wounds
- Leg eczema/dermatitis [11][12]
- Need for frequent dressing changes due to weeping (i.e., large/copious drainage)
- Cutaneous pressure damage from previous use of elastic bandages
- Conditions requiring modified compression (20-30 mmHg), such as mild/moderate PAD. To determine compression level indicated for a patient, see topic "How to Select Adequate Compression Therapy Pressure Levels and Products".
UB should be used with caution and in collaboration with a vascular specialist in the following situations:
Contraindications
Contraindications to UB include:
- Contraindications to compression therapy in general (e.g. severe PAD, unstable congestive heart failure with pulmonary edema, untreated lower limb skin or ulcer infection, untreated acute deep venous thrombosis). See 'Contraindications' in topic "Compression Therapy".
- Patient allergy to any of the ingredients in the UB paste (i.e., zinc oxide, calamine, glycerin, sorbitol gelatin or magnesium aluminum silicate)
While some manufacturers may list Unna boots as contraindicated for patients who are unable to walk or move (non-ambulatory), these patients might still benefit from UB. Even though their muscle pump might not be functional, minimal toe movement or passive ankle mobilization performed by physiotherapists may produce a massaging effect that can help promote venous return.[10] In those cases, it is crucial to monitor closely for potential complications such as pressure injuries due to lack of movement.
Frequency of Change
- If ulcer present, apply UB after every dressing change. For non-infected wound with small to moderate drainage and adequate dressing, may change weekly.
- Medicare allowed frequency of change under the Surgical Dressing Benefit is once every week. See section 'Coding, Coverage and Reimbursement' below.
- If ulcer not present, may change weekly.
- If VLU not present, UB is not covered under the Surgical Dressing Benefit. See section 'Coding, Coverage and Reimbursement' below.
Risks
- Paste-impregnated bandage may cause contact dermatitis requiring discontinuation of UB.[9]
- May contribute to non-adherence to care plan, as some patients find UB bulky and uncomfortable.[9][13]
- Application is largely operator-dependent. Incorrect application may lead to inefficient compression, pressure damage or other complications.[9][14]
HOW TO APPLY AN UNNA BOOT
Assessment and Plan
Application of an UB is part of a comprehensive care plan. Prior to applying, it is important that a comprehensive assessment be performed so that the following questions can be answered:
- Does the patient have a VLU? If so, is it healable?
- For compression therapy recommendations for VLUs based on their potential for functional healing (i.e. healability), see section 'Compression Therapy' in topic "Venous Ulcers - Treatment and Prevention"
- Are there any contraindications to compression therapy/UB?
- See 'General Indications and Contraindications' above
- If using compression therapy, what pressure level is indicated?
- See topic "How to Select Adequate Compression Therapy Pressure Levels and Products".
- What are the risks and benefits for the patient?
For details on VLU assessment, see topic "Venous ulcers - Introduction and Assessment". For guidance on treatment plan for VLU, see topic "Venous Ulcers - Treatment and Prevention"
Procedure
Training in the application of bandages is crucial for adequate outcomes. This is especially true for inelastic bandages, which should be applied with a higher initial pressure compared with elastic material. Instruction of compression application with the use of interface pressure measurement has been shown to improve technique.[10]
There are several variations of this procedure. Tables 1 to 3 below illustrate steps and rationale of an application methods utilizing zinc paste bandage (UB) covered with an outer layer of an inelastic cotton wool bandage (Rosidal® or Comprilan®), thereby producing a multilayer, multicomponent inelastic bandage.[9][10][15] Review manufacturers' instructions for use and the organization's policies and standards prior to applying.
Table 1. Pre-Application
| Steps | Rationale/ Tips
|
|
1. Apply/re-apply UB early morning, as soon as patient wakes up if possible
|
- If patient sleeps on a bed, legs are probably least swollen in the morning
|
|
2. Ensure adequate supplies and assistance if needed: - Appropriate lighting
- Clean gloves
- Soap and water
- Bandage scissors (with blunt tips)
- Wound dressings for ulcer if present
- Commercially prepared rolled gauze bandage impregnated with paste (e.g., Viscopaste, McKesson Unna Boot)
- Cast padding
- Short-stretch bandage to cover the zinc bandage (alternatively, elastic bandage, gauze wrap, or tubular dressing may be used)
|
- Commercially prepared bandages may come plain (with zinc oxide only, white color) or with calamine and/or other substances.
- Zinc with calamine: usually a non-hardening pink paste. Calamine may help reduce itching, pain and skin irritation (e.g., Gelocast Unna Boot, McKesson Unna Boot with Calamine)
- Cast padding may be used over impregnated bandage to protect bony prominences or absorb exudate
|
3. Remove previous bandage/wound dressing if present. Wash, cleanse or shower leg with water and soap. Dry leg
| - To remove previous bandage, may cut bandage off with bandage scissors with blunt tips by lifting bandage away from the skin to avoid skin damage (and away from the ulcer location, if applicable).
|
|
4. Measure the ankle circumference 10 cm from the bottom of the heel; measure the calf circumference 30 cm from the bottom of the heel
|
- To obtain a baseline edema measurement prior to first time application of an UB, and compare prior to subsequent applications and monitor improvement
|
|
5. If ulcer present, don clean gloves and perform local wound care and apply wound dressing as needed
|
- If wound dressing contains silver (e.g., Acticoat Flex3 or Acticoat Flex7), use an interface (e.g., gauze dressing) between the silver containing dressing and the paste-impregnated bandage, to prevent the paste’s emulsifier from coming in contact with the silver dressing
|
Table 2. Application
| Steps | Rationale/ Tips |
1. Don clean gloves
| - To keep new bandage clean during application
|
2. Position patient: if seated, support foot off the floor. If supine, elevate affected leg. Position the patient's leg and foot at a 90-
degree angle (Figure 1).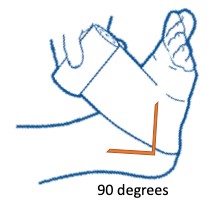 Fig. 1. Position the patient's leg and foot at 90 degree angle
| - Dorsiflexion helps with comfort and functionality when patient walks
|
3. Apply first/inner layer: zinc paste bandage can be applied in a spiral fashion. A 10-m bandage is recommended for one lower leg. It is important that bandage be applied with smooth constant contact avoiding wrinkles or a loose/baggy wrap that would result in noncontact. Spiral fashion: - Begin at the base of the toes. Wrap bandage around the foot, heel and around the leg in a spiral fashion and with an overlap of 50% up until just below the knee. Once applied, the bandage should then be smoothed and molded around the leg (Figure 2)

Fig. 2. Application of paste bandage on right leg, spiral fashion
| - Stiff bandage material is not easy to handle. Most untrained clinicians apply inelastic bandages with too low a pressure. Ensure bandage is applied with smooth constant contact and according to manufacturers instructions, as pressure often falls as a result of the immediate removal of edema.[10]
- When initiating therapy, especially for a patient who has never worn compression before, many clinicians prefer to apply the wrap more loosely and slowly increase pressure with subsequent dressing applications, to increase patient compliance with therapy. Some compression is better than no compression.
- Check with manufacturers in regards to resulting working pressure, distribution of pressure and stiffness.
- Inelastic bandages (e.g. zinc paste bandages) should be applied with much higher resting pressure, pressing the bandage roll toward the leg as if molding clay.[10]
- To obtain a homogeneous pressure distribution without creating constricting bands or folds, cut the zinc bandage when it does not exactly follow the cone-shaped leg surface during application.
- When wrapping the foot and ankle area, ensure that all skin is covered and there are no gaps, which can force edema to the uncovered area of skin and cause blistering or new wound formation.
- A variation of the spiral technique for the ankle and heel regions includes (Figure 3):
- Wrapping with 50% overlap from the base of the toes
- Then wrapping around the ankle with 1-3 figure eights, and
- Continue spiral wrapping with 50% overlap up until just below the knee
- For proper use of each product, it is important to review manufacturers' instructions, as certain brands suggest application of UB with figure eights at the ankle while others do not.

Fig. 3. Figure of eight around the ankle, spiral fashion - Cast padding may be applied on top of inner layer for padding of bony prominences or to absorb wound exudate.
|
4. Apply outer layer: Apply a 5-m-long short-stretch bandage over the zinc paste bandage with graded compression and 50% overlap. | - This layer prevents soiling of clothes and bedcover. This short-stretch bandage can be washed and reused with each change of the bandage.
|
Table 3. Post-Application
| Steps | Rationale/ Tips |
| 1. If possible have patient in supine position or with legs elevated until UB dries. | - So that UB molds to leg with minimal edema. Pressure level may be highest after application but will likely decrease with usage.
|
| 2. Monitor patient for leg pain, or other signs of circulatory impairment (cyanosis, coolness, numbness). If present, UB is too tight and must be removed immediately. Consult with patient's physician before reapplying the boot | - To reassess for PAD or other condition impairing leg blood supply
|
3. Complete required documentation as listed in section ‘Documentation’ below.
| - Documentation should be thorough and consistent for quality of care and reimbursement
|
4. Educate patient to look for signs/symptoms of circulatory impairment, keep UB dry during shower/bathing, avoid damaging the boot when walking
| - See topic "Patient Education - Shower Instructions for People with Wounds"
|
5. Schedule follow up within one week or as ordered
| - See “How to Assess Effectiveness” below
- When the bandage loosens, it should be replaced to stop the limb from swelling with edema again and to prevent any constriction effects due to the compression material slipping down. In the initial phase, renewal may be necessary once a day.[10]
- After edema has subsided, the bandage is changed every 7 days on average.[10]
|
Documentation
Following the procedure, document the following:
- Patient consent
- Medical diagnosis
- Location of the VLU
- Previous ulcer debridement (required for Medicare reimbursement of dressing supplies and UB)
- Appearance of the wound:
- Pre-debridement dimensions: diameter, depth, area in centimeters
- Undermining or tunneling, wound bed tissue composition by percentage, color, presence of exudates or necrotic tissue, signs of infection, purulent drainage or abscess, visible structures such as bone, tendon, vessels or nerves
- Vascular status, or evidence of reduced circulation
- Photograph of the wound
- Type of dressing applied to the wound
- Type of UB applied to the wound
- Presence/absence of signs/symptoms of circulatory impairment after application
- Date for follow-up assessment
- Other post procedure notes or patient teaching, including follow up instructions
The medical record must include a plan of care containing treatment goals and physician or other qualified provider follow-up.
HOW TO ASSESS EFFECTIVENESS
Signs of effectiveness include:
- Increasing proportion of granulation tissue on wound bed and no signs or symptoms of infection
- Decrease in wound area, depth, exudate, necrotic tissue
- Resolved eczema or dermatitis within 2 weeks;
- Measurable improvement in the ankle and calf measurements within 1 week
CODING AND REIMBURSEMENT
Overall, compression bandages (including UB), wraps and certain gradient compression stockings are covered by Medicare under the conditions below.
Coverage under the Medicare Part B Surgical Dressing Benefit
If UB is used at a Medicare beneficiary's residence and not applied by a physician who bills Medicare for UB application, UB is covered under the Medicare Part B Surgical Dressing Benefit.[16] Medicare coverage for compression devices, including UB, is managed by Medicare Administrative Contractors (MAC). Coverage is explained by the following articles:
- Local Coverage Determination (LCD) Surgical Dressings (L33831) [16], and
- Local Coverage Article: Surgical Dressings - Policy Article (A54563) [17]
Zinc Paste Impregnated Bandage (Unna boot)
- HCPCS: A6456 - Zinc paste impregnated bandage, non-elastic, knitted/woven, width greater than or equal to three inches and less than five inches, per yard
- Coverage requirements: VLU that meet the statutory requirements for a qualifying wound (surgically created/modified, or debrided).
- Frequency of replacement allowed by Medicare: 1 time/week
- Non-covered conditions: Non-qualifying wounds (see coverage requirements above)
- Modifier: A6456 billed without A1-A9 modifiers will be rejected as missing information.
BILLING REMINDERS:
- When multi-layer compression bandage systems are used for the treatment of a venous stasis ulcer, each component is billed using a specific code for the component - e.g., moderate or high compression bandages (A6451, A6452), conforming bandages (A6443, A6444), self-adherent bandages (A6454), padding bandages (A6441), zinc paste impregnated bandage (A6456)
- Medicare billable unit for bandages used in multilayer systems are "per yard".
- When billing Medicare, check number of yards per bandage as described by manufacturer and indicate number of units (i.e., yards) to be used during the period for which supplies are being requested. As per Medicare Policy: "For all dressings, if a single dressing is divided into multiple portion/pieces, the code and quantity billed must represent the originally manufactured size and quantity".
Coverage as part of a physician/QHP professional service
If a physician applies surgical dressings as part of a professional service that is billed to Medicare, the surgical dressings are considered incident to the professional services of the health care practitioner and are not separately payable. Claims for these dressings must not be submitted. Claims for the professional service, which includes the dressings, must be submitted to the local carrier or intermediary. If dressing changes are sent home with the beneficiary, claims for these dressings may be submitted (see above). In this situation, use the place of service corresponding to the beneficiary's residence; Place of Service "Office" (POS=11) must not be used.[17]
Strapping: Unna Boot (CPT code 29580)
- CPT: 29580 Strapping: Unna Boot
- Coverage requirements: check with your specific MAC. In general, UB application is covered for VLUs, and may be covered for treatment of ligamentous injuries (sprains and strains) of the ankle.[18] See topic "Medicare Coverage Determinations for Wound Care"
- Modifier: Bilateral UBs should be billed with a modifier -50 (bilateral procedure).[18]
Billing reminders:
- Debridement and UB: All supply items related to the Unna boot are inclusive in the reimbursement for CPT code 29580. When both a debridement is performed and an Unna boot is applied, only the debridement may be reimbursed. If only an Unna boot is applied and the wound is not debrided, then only the Unna boot application may be eligible for reimbursement. The National Correct Coding Initiative (NCCI) Policy Manual for Medicare Services Chapter 4, section G states that debridement codes (11042 -11047, 97597) should not be reported with codes 29580, 29581 for the same anatomic area.[19][20] For information on coding/coverage for debridement, see section 'Coding and Reimbursement' in topic "How to Perform Conservative Sharp Wound Debridement".
Application of multi-layer compression system
- CPT: 29581 - Application of multi-layer compression system, leg (below knee), including ankle and foot
- When a zinc paste impregnated bandage (UB, HCPCS A6456) is one of the layers of a multi-layer compression system, use CPT 29581
- Modifier: Bilateral UBs should be billed with a modifier -50 (bilateral procedure).[18]