Last updated on 10/9/24 | First published on 10/4/18 | Literature review current through Mar. 2025
[cite]
Authors:
Tiffany Hamm BSN, RN, CWS, ACHRN, UHMSADS,
Jeff Mize RRT, CHT, UHMSADS,
Scott A. Robinson MD,
Steven Orr MD, FACEP/UHM, FAPWCA,
Topic editors:
Eugene Worth MD, M.Ed., FABA, ABPM/UHM,
more...
Coauthor(s)
Jeff Mize, RRT, CHT, UHMSADS
Disclosures: Nothing to disclose
Tiffany Hamm, BSN, RN, CWS, ACHRN, UHMSADS
Chief Nursing Officer, Wound Reference, IncDisclosures: Nothing to disclose
Scott A. Robinson, MD
Disclosures: Nothing to disclose
Steven Orr, MD, FACEP/UHM, FAPWCA
Disclosures: Nothing to disclose
Editors
Eugene Worth, MD, M.Ed., FABA, ABPM/UHM
Disclosures: Nothing to disclose
CLINICAL
Overview
This topic describes the application and importance of transcutaneous oximetry in hyperbaric medicine and includes a practical algorithm based on expert consensus and evidence. For an in-depth summary of hyperbaric oxygen (HBO) therapy indications and common treatment protocols, see "HBO Treatment Indication With Protocol". For an introduction to HBO, refer to "An Introduction to Hyperbaric Oxygen Therapy".
Background
- Definition: Transcutaneous oximetry is a noninvasive method to analyze the partial pressure of oxygen in tissue.[1] In literature, it is frequently abbreviated as TCOM, TcPO2, PtcO2.
- Examples of TCOM brands: Radiometer, Perimed
How the intervention works
- Transcutaneous Oximetry (TCOM) allows the estimation of partial pressure of oxygen on the skin surface by employing noninvasive heated electrodes. TcPO2 values do not represent actual partial pressures of oxygen within the wound bed because the oximetric electrodes are placed over adjacent areas of the wound; the periwound.
- The electrode is heated, usually to 44 or 45 degrees Celsius, dilating the blood vessels and allowing oxygen to diffuse to the electrode. Unlike SPO2 sensors that measure saturation percentage of oxygen in the blood, the TCOM measures the actual number of oxygen molecules in the periwound tissue.[2]
- TCOM is best thought of as a mapping procedure. As such, the more periwound sites that are measured, the better. It is recommended that at least 2 periwound sites be used in clinical decision making. Mean TcPO2 values are better predictors of healing potential than single site values (i.e., the average of TcPO2 values from 2 or more adjacent sites of an area being studied). [3]
General indications and contraindications
Indications
- TCOM serves as a screening tool for peripheral arterial disease
- TCOM obtained while breathing normobaric air can assist in identifying which patients have wounds that will not heal spontaneously due to insufficient blood supply to the wound:
- TcPO2 value of < 40 mmHg is thought to represent sufficient hypoxia to impair wound healing [1][3]
- Patients with critical limb ischemia will almost always have a TcPO2 <30 mm Hg and usually less than 20 mm Hg [1][3]
- Amputation level prediction
- A systematic review and meta-analysis suggest the TCOM predicts healing complications of lower limb amputations. A TcPO2 value of less than 40 mmHg results in a 24% increased risk of healing complication compared to over 40 mmHg and the risk further increases as the TcPO2 value decreases.[4]
- Determining response to surgical revascularization
- As a screening tool to predict benefit from subsequent hyperbaric oxygen therapy [2]
Contraindications
Listed below are limitations of TCOM, rather than contraindications:
- TCOM can not be used on:
- Digits, as the electrodes and electrolyte rings are too wide
- Plantar portions of the feet, due to thickened skin
- Palmar surfaces of the hands, due to thickened skin
- TCOM can not be used in the wound bed due to the seal mechanism of the electrolyte ring needing to be airtight
- Patients on supplemental oxygen may not have a reliable TCOM examination
Evidence and recommendations
TCOM is helpful in determining HBOT candidacy of patients with non-healing ulcers. The algorithm below (Algorithm 1) maps TCOM values interpretation and recommendations based on an expert consensus and evidence. [3]
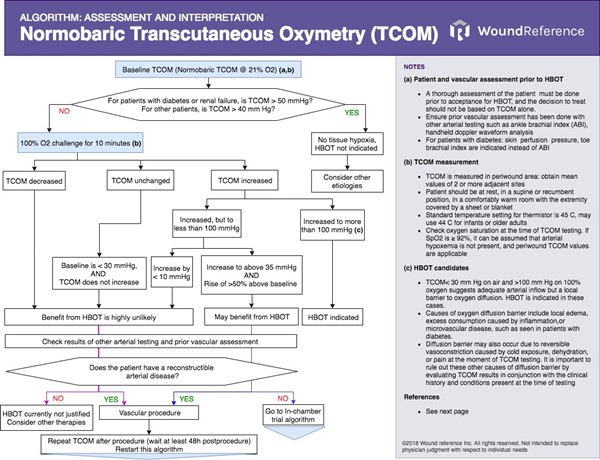
Consensus statements from the same expert panel [3] are also summarized below:
- Tissue hypoxia is defined as TcPO2 <40 mmHg
- In patients without vascular disease, TcPO2 values on the foot increase to a value > 100mmHg when breathing 100% oxygen under normobaric pressures
- Patients with critical limb ischemia breathing air will usually have a TcPO2 <30 mmHg
- Low TcPO2 values breathing normobaric air can be caused by a diffusion barrier (See definition of "diffusion barrier" on Algorithm 1)
- TcPO2 < 40 mmHg while breathing normobaric air is associated with a reduced likelihood of healing after amputation
- If the baseline TcPO2 increases < 10 mmHg while breathing 100% normobaric oxygen, this is at least 68% accurate in predicting failure post-amputation
- An increase in TcPO2 > 40mmHg during normobaric air-breathing after revascularization is usually associated with subsequent healing. This increase may be delayed.
- TcPO2 obtained while breathing normobaric air can assist in identifying which patients will have difficulty healing spontaneously
Practical remarks on TCOM measurement [3]
- TCOM is best thought of as a mapping procedure. As such, the more periwound sites are measured the better. It is recommended that at least 2 periwound sites be used in clinical decision making.
- TCOM measurements should be made with the patient at rest, in a supine or recumbent position, in a comfortably warm room, with the extremity covered by a sheet or blanket. Results of TCOM measurements conducted with legs at an angle to the body cannot be compared to those taken in a supine position.
- Standard temperature setting for thermistor is 45 C, may use 44 C for infants or older adults
- Check oxygen saturation at the time of TCOM testing. If SpO2 is ≥ 92%, it can be assumed that arterial hypoxemia is not present, and periwound TCOM values are applicable
- A normobaric oxygen challenge can determine if a low TCOM value (<40 mmHg) obtained while breathing normobaric air is due to arterial disease or a diffusion barrier
- A normobaric air TcPO2 value <30 mmHg that does not increase after breathing 100% normobaric oxygen for 10 minutes is consistent with severe arterial disease
- TcPO2 < 30 mm Hg on air and >100 mm Hg on 100% oxygen suggests adequate arterial inflow but a local barrier to oxygen diffusion
- Causes of oxygen diffusion barrier include local edema, inflammation, or microvascular disease, such as seen in patients with diabetes.
- Diffusion barrier may also occur due to reversible vasoconstriction caused by cold exposure, dehydration, or pain at the moment of TCOM testing. It is important to rule out these other causes of diffusion barrier by evaluating TCOM results in conjunction with the clinical history and conditions present at the time of testing
- For diabetic foot ulcers, if hyperbaric TcPO2 value exceeds 200 mmHg almost 90% of DFUs will heal regardless of the room air readings when HBOT is used as an adjunct to management. [5]
- TCOM is an excellent tool that has been providing wound healing data since the 1980s. While we have used it to make predictions about wound/ulcer healing, we now have additional technologies that also provide excellent data. We suggest that TcPO2 values be combined with Laser Doppler, fluorescence angiography, and, possibly invasive testing such as magnetic resonance angiography, CT angiography, etc.
Documentation requirements
Adequate documentation is essential for high-quality patient care and to demonstrate the reasonableness and medical necessity of the study(ies). Documentation must support the criteria as described in the Coverage Indications, Limitations, and/or Medical Necessity section of the Local Coverage Determination. Healthcare professionals should check coverage determinations of their specific insurers. See 'Coding, Coverage and Reimbursement' below. In general [6]:
- There should be a permanent record of the studies performed and the interpretation.
- Any known significant patient reaction or complications should be recorded. Comparison with prior relevant studies needs to be addressed in the documentation along with both normal and abnormal findings.
- Variations from normal should be documented along with measurements.
- The report should address or answer any specific clinical questions. If there are factors that prevent answering the clinical questions, this should be explained in the documentation
- If the provider of the study is other than the ordering/referring physician/non-physician practitioner, that provider must maintain a copy of the test results and interpretation, along with copies of the ordering/referring physician/non-physician practitioner’s order for the studies. This order is required to provide adequate diagnostic information to the performing provider.
- The physician/non-physician practitioner must state the clinical indication/medical necessity for the study in his/her order for the test.
- The provider is responsible for ensuring the medical necessity of procedures and maintaining the medical record, which must be available to Medicare upon request.
- Results of all testing must be shared with the referring physician.
- Non-invasive vascular studies are medically reasonable and medically necessary only if the outcomes will be utilized in the clinical management of the patient.
CODING, COVERAGE, REIMBURSEMENT
Coding
TCOM measurement is billed using CPT codes 93922 and 93923
- 93922: Limited bilateral noninvasive physiologic studies of upper or lower extremity arteries, (eg, for lower extremity: ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries plus bidirectional, Doppler waveform recording and analysis at 1-2 levels, or ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries plus volume plethysmography at 1-2 levels, or ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries with, transcutaneous oxygen tension measurement at 1-2 levels)
- 93923: Complete bilateral noninvasive physiologic studies of upper or lower extremity arteries, 3 or more levels (eg, for lower extremity: ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries plus segmental blood pressure measurements with bidirectional Doppler waveform recording and analysis, at 3 or more levels, or ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries plus segmental volume plethysmography at 3 or more levels, or ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries plus segmental transcutaneous oxygen tension measurements at 3 or more levels), or single level study with provocative functional maneuvers (eg, measurements with postural provocative tests, or measurements with reactive hyperemia)
- ABI must be performed prior to transcutaneous oximetry and is required to be documented in the patient's record in order to bill for TCOM.
AMA Guidelines:
- When only 1 arm or leg is available for study, report 93922 with modifier 52 for a unilateral study when recording 1-2 levels. Report 93922 when recording 1-2 levels bilaterally. Report 93923 with modifier 52 when recording 3 or more levels unilaterally or a unilateral single level study with provocative functional maneuvers. Report 93923 when recording 3 or more levels bilaterally or a bilateral single level study with provocative functional maneuver such as leg elevation or oxygen challenge.
- Report 93922 only once in the upper extremity(s) and/or once in the lower extremity(s). When both the upper and lower extremities are evaluated in the same setting, 93922 may be reported twice by adding modifier 59 to the second procedure
Coverage and Reimbursement
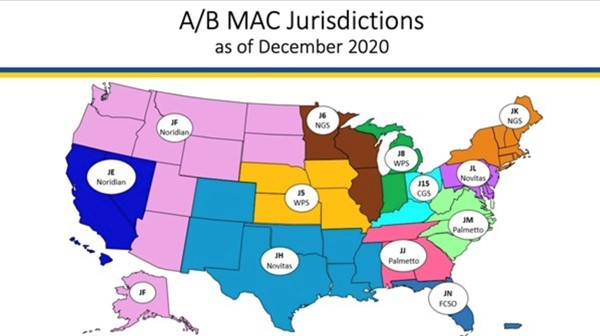
- Medicare coverage of provider and facility fees related to TCOM measurement is managed by Medicare Administrative Contractors (MAC), under Medicare Part A or Part B. Each jurisdiction may have its own specific local coverage determination and policies.
- MACs agree that in general, noninvasive studies of the arterial system (including TCOM) are to be utilized if significant signs and/or symptoms of possible limb ischemia are present. Other specific coverage details and requirements vary among MACs and thus, it is recommended that healthcare professionals check their MAC's coverage determinations or directly with their MAC.
- In the U.S., most MACs require that TCOM measurements be performed by personnel possessing the following credentials obtained from the National Board of Diving and Hyperbaric Medicine Technology (NBDHMT): Certified Hyperbaric Technologist (CHT), or Certified Hyperbaric Registered Nurse (CHRN)
- The figure and table below illustrate MAC jurisdictions and respective coverage determinations (if listed on the Medicare Coverage Database).
- Algorithms can be used to support your care plan and to justify medical necessity with the patient's insurance company.
Instructions
- Find your state, and respective MAC (in the white bubble)
- On the table below, find your MAC on the left column. The right column indicates if the MAC follows its own Local Coverage Determination (LCD)
- To go to the LCD, click on the reference number (in blue brackets in the right column) and go to its reference page. On the reference page, click on the green button "View Source".
- See details on requirements, medical necessity and documentation on specific Medicare Local Coverage Determinations.
Medicare Administrative Contractor
| Relevant coverage determinations and articles
|
| Noridian Healthcare Solutions, LLC (Noridian) | L34219 Noninvasive Peripheral Arterial Studies [7] Retired
|
| National Government Services, Inc. (NGS) | L33627 Non-Invasive Vascular Studies [8] A52859 Non-Invasive Vascular Studies – Supplemental Instructions Article- Retired
|
| Wisconsin Physicians Service Insurance Corporation (WPS) | L35761 Non-Invasive Peripheral Arterial Vascular Studies [6]
|
| Novitas | not found |
| CGS Administrators, LLC (CGS) | L34045 Non-Invasive Vascular Studies [9] A56697 Billing and Coding Non-Invasive Vascular Studies [10]
|
| Palmetto | not found |
| First Coast Service Options, Inc. (FCSO) | L33696 Noninvasive Physiologic Studies of Upper or Lower Extremity Arteries [11] |
QUALITY MEASURES
The Medicare Quality Payment Program currently does not have specific measures for TCOM measurement. Below is a measure that is directly related to TCOM measurements in the outpatient setting, issued by the qualified clinical data registry (QCDR) US Wound Registry.
| Setting | CMS Program | Developed by | Measure ID | Title | Description |
Outpatient
| Quality Payment Program
| US Wound Registry
| USWR 23
| Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential
| Percentage of patients aged 18 years or older with a non healing lower extremity wounds or ulcers that underwent a non-invasive arterial assessment once in a 12 month period, stratified by ABI, perfusion pressure, or oximetry
|
CATEGORY A CONTINUING EDUCATION CREDIT
This topic has been reviewed and approved by the National Board of Diving and Hyperbaric Medical Technology (NBDHMT) for one (1) Category A Credit. 'Meeting the Category A requirement related directly to any combination of hyperbaric operations, related technical aspects and chamber safety.'
To claim the credit:
- 1. Read the topic
- 2. Answer the examination and course critique questions.
- 3. Receive the certificate by e-mail. A passing score of 70% is required (please allow up to 8 business days for processing)
For more information on Category A continuing education credits see blog post " Hyperbaric Certification and Continuing Education for Technicians & Nurses".
Official reprint from WoundReference® woundreference.com ©2025 Wound Reference, Inc. All Rights Reserved
Use of WoundReference is subject to the
Subscription and License Agreement.
NOTE: This is a controlled document. This document is not a substitute for proper training, experience, and exercising of professional judgment. While every effort has been made to ensure the accuracy of the contents, neither the authors nor the Wound Reference, Inc. give any guarantee as to the accuracy of the information contained in them nor accept any liability, with respect to loss, damage, injury or expense arising from any such errors or omissions in the contents of the work.