AIR BREAK SYSTEM
Introduction
During monoplace hyperbaric oxygen therapy, it is necessary to provide an alternative air breathing medium. This may also be necessary to greatly minimize the risk of central nervous system oxygen toxicity in the general hyperbaric patient population
Description
The air breathing system consists of an independent high-pressure air source, capable of providing flow that is sufficient to meet the patient's inspiratory demand. Air breathing systems may be provided by institutional gas outlet (wall outlet) or via portable "H" cylinders utilizing a diameter index safety system (DISS) regulator. Delivery of the air break to the patient may be provided by disposable non-rebreather mask, demand valve and resuscitation mask or trach collar. For purposes of infection control, masks should be single patient use and cleaned or replaced (per patient) as needed.
�
Equipment Set-up
- Confirm medical grade compressed air H cylinder, high-pressure reducing regulator (set at 70 psig) or wall gas source is properly connected to the external chamber door (DISS or flowmeter).
- Connect the Non-rebreather, demand valve with mask or trach collar to internal gas outlet via DISS or christmas tree adapter.
- Confirm gas source pressure is set at 70 psig and test the system prior to initiating compression.
- H cylinders should be turned completely open during treatment.
- Instruct the patient about the rationale for the air break process.
- Confirm the patients understanding of how to use the air break delivery device.
Procedure
All patients treated in the monoplace hyperbaric chamber will have with the capability of administering an "air break" at any point during his/her treatment.
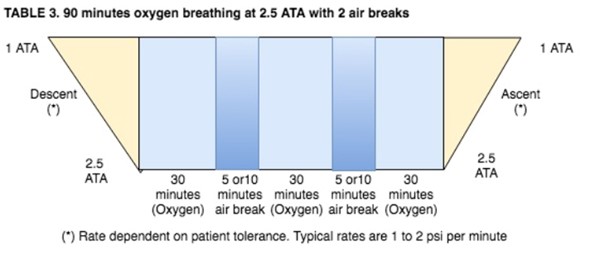
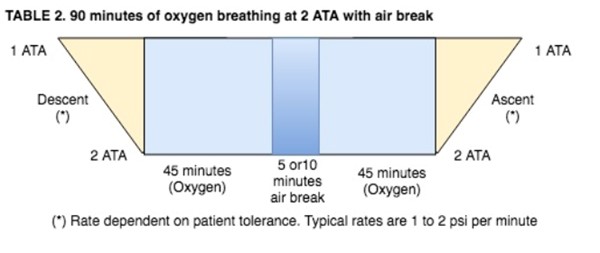
- Patients being treated at pressures above 2.0 ATA breathing 100% oxygen will receive scheduled "air breaks" as follows
- Patients that are known to have increased potential for central nervous system (CNS) oxygen toxicity and every patient being treated at pressures above 2.0 ATA will be given an "air break". Conditions that may increase the potential for CNS oxygen toxicity are:
- Febrile state (oral temperature >100˚F)
- Seizure history
- Associated head injury
- Concurrent administration of medication known to lower seizure thresholds
- This air break should be delivered as follows:
- For any CNS complications that develop during a patient's HBO procedure, refer to: ‘Emergency Procedures: Oxygen Toxicity’
BLOOD GLUCOSE LEVEL AND HBOT
To ensure that all patients who are currently being treated for irregular blood glucose levels do not experience a hypoglycemic event as a result of ongoing hyperbaric oxygen therapy.
Background
Most studies suggest that blood glucose (BG) decreases in diabetics undergoing Hyperbaric Oxygen Therapy (HBOT). This decrease in BG is estimated at 50 mg/dl. The effect of HBOT may also be less on non-insulin dependent diabetes mellitus patients. [1]
The goal is to ensure that all patients who are currently being treated, do not experience a hypoglycemic event as a result of ongoing hyperbaric oxygen therapy.
Policy Elements
The following standards should be utilized for those patients receiving hyperbaric oxygen therapy.
- Diabetic Patients (IDDM and NIDDM): blood glucose measurements by fingerstick are mandatory for all diabetic patients prior to and after hyperbaric oxygen treatment due to the hypoglycemic effect of HBO. It is assumed that this effect is due to the inhibition of the anti-insulin hormones (somatotropic hormone and glucagon) in the HBO environment.
- Recommend to the patient/ caregiver that patients eat one hour prior to their hyperbaric treatment assuring complex carbohydrates have been eaten, e.g., multigrain & vegetables
- Document the time, quantity and food consumed prior to arrival in the hyperbaric suite.
- Document the time and specific glycemic control medication taken prior to arrival in the hyperbaric suite.
o Staff should consider the timing of short and long-acting glycemic control medications when scheduling HBO to avoid peak action time while at depth in the chamber.
o Consider holding insulin until after the treatment.
o If the patient's Blood Glucose Level has been checked while inpatient within 1 hour of the hyperbaric treatment, the HBO staff does not need to repeat the Blood Glucose Level unless insulin was given.
o If more than an hour has passed since Blood Glucose level was checked, the HBO staff should recheck Blood Glucose level before treating the patient.
- Diabetic Outpatients: Blood glucose level must be checked by the hyperbaric staff on ALL diabetic patients prior to initiation of hyperbaric oxygen therapy.
- The following Blood Glucose level guidelines should be used for all diabetic patients.
- Blood Glucose Level: < 120mg/dl: Hold HBO treatment until further direction is given by the hyperbaric physician.
- Blood Glucose level: 120mg/dl – 130mg/dl:
- Patient should be given a complex carbohydrate and 4 ounces of juice to drink pre-treatment and also 4 ounces to drink during treatment.
- For Diabetic patients, blood glucose measurement should be performed after every treatment.
- No patient should be released with a blood glucose of less than 120mg/dl even if asymptomatic. It is possible that the blood glucose will continue to decrease after the patient is removed from the chamber.
- Patients with a blood glucose of less than 120 mg/dl should be fed prior to leaving the facility.
- Glucose gel should always be kept available for use.
CARDIAC MONITORING
To ensure that signs and symptoms of dysrhythmia are recognized and promptly addressed.
For cardiac monitoring, standard monitoring devices may be used outside the chamber. Outside monitors use through-the-hull penetrators to gain patient connection. Only specialized cardiac cables are allowed inside the chamber and must be tested and approved by the HBO Safety Director. [1]
- As ordered, patients will be placed on a cardiac monitor while in the chamber.
- Typically, cardiac monitoring is recommended upon initial treatment for all patients, and for subsequent treatments for patients with heart conditions.
- Patients will be placed on the cardiac monitor during their initial treatment whether or not there is an underlying etiology.
- All patients undergoing cardiac monitoring will have ECG monitoring during hyperbaric treatment:
- Alarm settings will be set to 20 above and 20 below patient heart rate or per physician's order.
- The alarms should NOT be turned off at any time during patient treatment.
- After the patient reaches the prescribed pressure or ectopy is detected at any time, a rhythm strip should be printed and scanned into the electronic medical record or placed in the patient's chart.
- Notify the hyperbaric physician of ectopy or dysrhythmia. Oxygen toxicity is commonly preceded by tachycardia.
FEEDING TUBES
To provide a process for effectively managing patients with feeding tubes in place during hyperbaric oxygen therapy. Patient feeding via the feeding tube will be discontinued during hyperbaric oxygen therapy.
Procedure
- Explain to the patient the need to discontinue tube feeding.
- Clamp and disconnect line from the patient’s feeding tube.
- Open clamp to the feeding tube. Flush with 10-15 ml of water (do not use saline in the stomach) and reclamp. Begin hyperbaric treatment.
- Upon completion of hyperbaric treatment and removal of the patient from the chamber, reconnect the feeding tube. Unclamp the tube and restart the pump.
Note: Nasoduodenal feeding tubes like the Dobhoff are inserted into the stomach and duodenum. There is no risk of barotrauma due to gas expansion during ascent. The gastrostomy tube/ feeding tube is inserted through the abdomen into the stomach.
MANAGEMENT OF DRAINAGE TUBES
Avoidance of gastric distention which could lead to aspiration of gastric contents can be achieved with the continued use of nasogastric tube during HBOT. Bladder distention can be avoided with the use of a foley catheter. It is important to follow hyperbaric procedures for the care and function of drainage tubes to prevent backflow of drainage or air.
Procedure for nasogastric (NG) tube:
- Non-ventilated/alert patients:
- Disconnect NG tube from suction and cap the tube during treatment.
- NG tube should be visible to the chamber operator at all times.
- Ensure the tube is properly secured to the nose.
Procedure for Foley Catheter
Foley catheters require no special attention except to avoid kinking in the tubing and to empty the vented tubing bag before treatment.
- Prior to hyperbaric treatment, unclamp the drain hose on collection bag and empty all contents into measuring device to record output. Report urinary output to the inpatient nurse
- Expel air from the foley bag by rolling it up, re-clamp the exit port and then unroll the bag to allow for gravity drainage during HBOT and expansion of bag on ascent.
- Place the foley bag flat on the gurney between the patient's legs to aid drainage.
- Ensure main foley tube is secured to the patient's leg
- Check to ensure the tubing running from the patient's bladder to the collection bag is patent, unkinked and unclamped. [1]
Procedure for Hemovacs and Jackson Pratt Drains
- Prior to hyperbaric treatment, uncap the drain and empty contents into a measuring device. Report drainage amount to the inpatient nurse as applicable.
- Expel the air from the drain and close the cap. This will allow for the drain to continue functioning during HBOT.
- Ensure the drain is visible to the chamber operator at all times and secured to the patient.
- If the patient reports pain during ascent or descent, pause the chamber pressure, assess and resume gradually once the patient is pain-free. If pain at the drain site persists, notify the provider and plan to ascend patient.
�
EARLY ASCENT DURING HBOT
To ensure that the occurrence of early ascent during hyperbaric oxygen therapy is reviewed and recorded.
The Hyperbaric Medicine Service is aware that early ascent during HBOT may be necessary.
- Any occurrence of early ascent or termination of a treatment before the prescribed actual bottom time is complete, will be reviewed by the hyperbaric physician and Safety Lead.
- The attending clinical staff member and physician shall complete an early ascent form.
- Copies of the form should be provided to the Medical Director and Safety Director. A copy should also be placed in the patient’s chart or scanned into the electronic medical record.
- After completion of the Early Ascent Form (see attachments), the documentation will be entered into the monthly QA.
- Any action required, as a result of the early ascent, will be at the discretion of the hyperbaric physician.
- Early ascent will decrease the total treatment time therefore possibly altering the number of 30-minute increments billed with HCPCS code G0277.
FAMILY VISITATION
To prevent an influx of visitors that might impede safe and effective patient care and maintain patient privacy.
Policy Elements
The hyperbaric staff member(s) present have the ultimate authority to permit/not permit visitors/patient family members at any time in the hyperbaric facility.
- In general, visitors are discouraged from entering the hyperbaric medicine facility, unless they are accompanied by a staff member.
- An inpatient's family members/friends are advised to wait in the patient's hospital room or in one of the hospital waiting areas, while the hyperbaric treatment is underway.
- Outpatient family members/friends who travel daily with the patient should be asked to wait for the patient in designated waiting areas, not in the hyperbaric facility.
- In the event that the patient may benefit by having someone with him/her during their initial treatments (i.e., pediatric patient or confinement anxiety), one family member may sit beside the chamber and communicate with the patient. The visitor must leave the facility whenever other patient care needs arise, as necessary.
- Visitors must stay in the designated areas within the HBO unit as identified by staff.
- Visitors with contagious diseases or known infections will not be allowed to enter the hyperbaric facility.
- Children under the age of 12 are not permitted in the hyperbaric treatment area during patient care or treatment.
- Photographs taken by visitors will be allowed only with the written prior authorization stating approval. [2]
FLUID VOLUME DEFICIT
Patients undergoing HBOT for conditions such as Gas Gangrene and necrotizing soft tissue infections, the patient's fluid and electrolyte status should be monitored and adjusted accordingly to maintain homeostatic conditions, particularly to avoid volume depletion which could lead to peripheral vasoconstriction. [3]
Ensure that the signs and symptoms of fluid volume deficit will be recognized and promptly addressed.
- Assess patient’s potential for fluid imbalance i.e.: dialysis, diuretics, diarrhea, vomiting, fever.
- Assess skin turgor and oral mucous membranes for signs of dehydration.
- Assess for alteration in mentation (confusion, agitation, slowed response)
- Assess fluid and electrolyte balance. Maintain hydration and blood pressure support as indicated by physician order.
- Monitor patients Intake & Output, as directed by physician order.
- Monitor patient’s vital signs. [1]
HEIMLICH VALVE
To avoid over expansion of the lungs and maintain drainage of chest tubes during hyperbaric oxygen therapy for those patients with chest tubes in place. Treating a patient with a chest tube in the hyperbaric environment requires the placement of a Heimlich valve to prevent the progression of the pneumothorax or hemothorax to a tension pneumothorax.
Before Hyperbaric Treatment
- Assess respiratory status of patient. Determine if a large air leak is present requiring suction. If so, notify HBO physician to determine if HBO should be held.
- Clamp off chest tube with hemostats
- Disconnect from underwater seal drainage.
- Connect Heimlich valve to the end of the chest tube. NOTE: be sure the arrow on the valve is pointing AWAY from the patient’s chest. Quickly unclamp chest tube and secure the Heimlich valve with tape to prevent accidental dislodging.
- Connect distal end of Heimlich valve to a drainage container:
- If drainage is present, may use sterile urinary drainage bag or sterile glove.
- If no drainage, may use vented sterile glove.
- Check for negative seal to prevent leakage and/or accidental dislodging.
- Assess respiratory status of patient.
- Compression and decompression rates should be slowed to allow adequate pleural venting. [1]
After Hyperbaric Treatment
- Assess respiratory status of patient.
- Clamp off chest tube with hemostats
- Reconnect distal end of the Heimlich valve or chest tube to underwater seal drainage.
- Unclamp chest tube
- Assess respiratory status of patient.
INTRAVENOUS INFUSION
Goal: To administer IV infusion of fluids and medications as required during hyperbaric oxygen therapy; to minimize the risk of iatrogenic air embolism; to maintain patency of IV lines.
Background
Intravenous infusion capability is typically performed in level 1 hyperbaric centers, which provide emergent HBOT 24/7. These patients may originate from the emergency room or the intensive care unit and may require medications to be administered intravenously during HBOT. It is important that all of the connections are tight and there are no leaks or air of any visible amount in the tubing.
For patients requiring continuous intravenous infusions during HBOT, a special extension set was developed for the monoplace chamber. It includes a pass-thru and has a back check valve which allows the I.V. fluid to flow in only one direction. Specialized pumps are used to overcome the pressure inside the chamber and should not be used elsewhere in the hospital to prevent injuries. [1]
As a result, the necessary increased line pressures can preclude line occlusion warning capabilities, which may lead to infiltration of the IV site. This is particularly true of older pumps commonly employed in many hyperbaric units e.g. IVAC® 530 and Abbott® Hyperbaric pumps. Clinical Concerns: Infiltration of intravenous lines may have only minimal consequences for the patient such as minor swelling, inflammation, and discomfort. Unfortunately, serious consequences may ensue as a result of the pressure causing effects of fluids confined within soft tissues (compartment syndrome), severe ischemia from vasoconstriction (vasoactive sympathomimetic amines i.e. pressors), or frank necrosis from chemotherapeutic agents.
Additionally, the patient may be put at risk should the dosage of pressor agents fail to reach therapeutic levels when not properly infused. Loss or inappropriate dosing of analgesic or sedative medications may likewise have adverse effects particularly in the mechanically ventilated patient. [4]
Monoplace chambers are limited in the number of IV pass-thru ports. Careful consideration should be given of which drugs and IV solutions are necessary during HBOT. For example, if the patient is receiving separate infusions of total parenteral nutrition (TPN) and insulin, those two infusions could be joined together before infusing the solution through the chamber. [3]
Recommendations
- All IV sites should be thoroughly assessed prior to, every 15 minutes during treatment, and upon completion of hyperbaric treatments. Special attention should be given to the tubing and the respective IV sites after the patient is positioned in the chamber as tubing may become kinked or dislodged. The nurse shall document these assessments.
- During treatment, IV sites should be periodically visualized such that swelling or discoloration may be identified in a timely fashion.
- Intravenous infusions should be stopped should any signs indicative of IV infiltration be identified. The appropriate nurse manager and attending physician should be promptly notified.
- Suspicious or negative findings shall be documented in the patient chart along with necessary corrective interventions.
- Use of arm boards or splints should be considered when the location of intravenous access may result in positional occlusion e.g. antecubital fossa, dorsum of hand.
Safeguards
- Procedure for Chamber Setup/Removal
- Slightly loosen metal nut on outside of chamber door
- Remove metal port. Ensure the small black rubber O-ring remains in place
- Slide the IV back check extension through the IV port on the chamber door from the inside to the outside. Tighten the nut at the outside of the door.
- Ensure patency of IV site.
- Attach IV tubing from IV solution (outside the chamber door). When the solution fills the tubing, then connect the 3-way stop cock (comes in extension set tubing), followed by connecting the back check tubing to the patient’s IV port.
- Be sure backcheck valve is between patient and chamber door
- Tighten down an Interlink cap (or other needleless hub) on open port of stop-cock
- Place IV tubing through appropriate pumping device
- Check to see that all clamps are open; confirm tubing is bubble free
- Check for correctly ordered rate of flow and functioning of equipment before closing chamber door
- When the patient has exited the chamber, remove back check tubing from inner chamber door, replace metal port, and tighten metal nut.
- Procedure for PRN medication administration
- Turn off the pump.
- Close the 3-way valve of the stop cock to the pump.
- Push the medication through the cap/hub, follow with a 10cc saline flush.
- Turn the 3-way stop cock to close off the open port (open access from the pump to the patient).
- Turn on IV pump
MEDICATIONS IN THE HYPERBARIC ENVIRONMENT
Goal: maximize patient safety during HBO therapy.
Policy Compliance
The Hyperbaric Medicine service will adhere to the institutional policies for the preparation, dispensing and procurement of medications. Emergency medications are consistently available. A crash cart will be immediately available to the Hyperbaric Medicine Service.
Policy Elements
A hyperbaric and hyperoxic environment creates numerous considerations for the use of drug therapies within it. Physiologic changes to the body from HBOT may lead to pharmacokinetic changes in drug disposition. In addition, HBO acting as a drug can interact and enhance or lessen the physiologic effect of the drug. Most drugs will not interact unfavorably with oxygen. Unless specific contraindications or precautions have been addressed, it is generally safe to assume a medication can be used. Significant known exceptions and their evidence along with implications of hyperbaric oxygen will be discussed. [3]
Pharmacodynamic interactions result in modification of the pharmacologic effect of the drug after administration. These interactions will increase or decrease the effects of oxygen or the drug. [3]
See "Medications In The Hyperbaric Environment" for information regarding drugs that:
- Are incompatible with HBOT due to enhanced toxicity
- Drugs which decrease tolerance to oxygen toxicity
- Drugs which increase tolerance to oxygen toxicity
- Considerations for commonly used drugs
- Antiarrhythmic agents
- Transdermal systems
- Implantable medication delivery systems
MODIFICATION OF TREATMENT PROTOCOL
To ensure that any modification in treatment protocol is done within the appropriate treatment guidelines.
The Hyperbaric Medicine Service is aware of the potential to modify or change a patient’s treatment protocol (i.e. Diabetic Foot Ulcer being modified to Compromised Flap following surgery).
- The hyperbaric physician and Program Director will review any occurrence of a modification or change in the treatment protocol.
- The attending clinical staff member and physician shall complete a modification in treatment protocol form. see attachments.
- Copies of the form should be provided to the Medical Director, Safety Director, and Program Director. A copy should also be scanned into the patient’s electronic medical record.
- The physician ordering the modification or change in treatment protocol may dictate a note regarding the change in protocol.
- After completion of the modification of the treatment protocol form, the documentation will be entered into the monthly QA.
- Any action required, as a result of the modification or change in the current treatment protocol, will be at the discretion of the medical director.
�
PAIN ASSESSMENT
Provide optimal pain assessment and management.
Policy Elements
Pain can be extraordinarily complex to control and is often inadequately managed, leaving more than 100 million adults in the United States living with pain. Early appropriate interventions of acute pain, however, can prevent chronic pain, a serious disease that involves changes to the nervous system that can lead to a greater perception of pain severity. [5]
Pain Assessment
- Pain is recognized as the 6th vital sign
- Pain is "whatever the experiencing person says it is, existing whenever and wherever the person says it does" (McCaffery 1968). Self-report is the preferred indicator of pain.
- All patients should be assessed for pain at the time of consultation and reinforced during each subsequent visit.
- Many options are available for rating pain level. (numeric 0-10, Wong-Baker faces). Ensure these are patient appropriate.
- Assessment findings will be documented in the electronic medical record.
Pain Management
- Pain relief is the alleviation of pain or the reduction in pain to a level of comfort that is acceptable to the patient and is demonstrated by a decrease in the patient's pain scale rating and an improvement in physical, cognitive and behavioral and/or psychosocial functioning
- Pain management requires a multi-faceted approach using pharmacological interventions (opioid and non-opioid) and nonpharmacological approaches together to provide comfort.
- An individual's experience of pain will manifest itself in emotional and behavioral responses particular to his or her culture, personal history and unique perceptions. [6]
Pain Education
- All patients should be educated on pain management at the time of consultation and reinforced during each subsequent visit
- Patients and families should be provided with written information about pain management.
- Patients and families should be taught to use a pain rating scale that is age, condition, and language appropriate for reporting pain intensity with the goal of pain prevention.
- Patients should be taught about pharmacologic and non-pharmacologic interventions and the potential side effects.
Procedure
- All patients should be assessed for pain
- All clinicians are responsible for pain assessment
- An individualized pain management plan which includes the patient's goal for pain management, patient preferences for treatment, age, type of pain, and cultural beliefs and practices.
- Notify the hyperbaric/ wound physician of a new occurrence of pain, unrelieved pain or increase in pain.
PATIENT EDUCATION
Education of the patient and his/her family improves patient health outcomes by helping to promote a healthy behavior and involving the patient int care and care decisions. The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) includes education as one of its own standards for hospital accreditation. [1]
The JCAHO's goals that substantiate education of the patient in the wound and hyperbaric environment encompass but are not restricted to:
- Formulating patient education program goals
- Allocating resources for patient education
- Determining and prioritizing specific patient educational goals
- Providing education to meet the identified patient needs
Activities involved in addressing the above goals include, but not restricted to:
- promoting interactive communication between patients and providers
- improving the patient's understanding of his/her health status, options for treatment, and anticipated risks and benefits of treatment
- enhancing patient participation in continuing care
The hyperbaric and wound education program should:
- Include safety as the key component in the safe delivery of HBOT
- encourage patients' involvement in their care and educational process
- ensure that the educational plan encourages an ongoing interaction between patients and staff
- involve the entire staff of the wound and hyperbaric facility including physicians, nurses, technicians, respiratory therapists, and part-time patient care staff.
- help the patient understand and accept the reasons he or she needs the intervention
- communicate with patients in a way that fosters the patient's learning
- provide instruction on a level understandable to the patient by speaking in simpler language, repeating instructions, and demonstrating key points while avoiding too many directives.
- provide easy-to-read written patient education materials with oral instruction. [1]
The basic principles of education are in accordance with patient rights.
- All patients have the right to access care, respect, confidentiality, and dignity
- All patients have the right to be involved in all aspects of their care-planning including decision making.
Patient education benefits:
- helps to maximize the benefit of hyperbaric therapy and improves cost-effectiveness and patient care.
- increases patient satisfaction, improves quality of life and ensures continuity of care by reducing the incidence of complications with illness, promoting adherence to treatment plans, and decreasing patient anxiety. [1]
Patient preparation for HBOT. The patient should be educated about:
- the purpose and indication for the treatment
- the risks, hazards and benefits involved with HBOT as discussed by the physician or qualified health professional (QHP) prior to consenting the patient
- the risk factors which include but are not limited to fire, barotrauma, pneumothorax and oxygen toxicity of the central nervous system, pulmonary and ophthalmic function.
- ear equalization techniques
- safe and effective use of medications including potential drug/food and drug/drug interactions.
- safe and effective use of appropriate medical equipment or supplies
- safety policies and procedure of the hyperbaric unit
- expectations of the treatment such as temperature changes, in-chamber noise, middle ear equalization, confinement anxiety and fire hazards.
- nutritional interventions and requirements for wound healing
- the daily routine and tour of the hyperbaric unit [1]
PATIENT HYPERBARIC TREATMENT
All patients will be treated upon:
- Consultation and approval by the hyperbaric physician or QHP.
HBO Pre-Treatment Checklist
- Ensure patient ground bracelet is in place and grounding procedure has been performed.
- Confirm patient is dressed in 100% cotton gown or scrubs provided by the hyperbaric unit
- Complete the HBO pre-treatment safety checklist (timeout) with the patient prior to initiating treatment.
- Check that the patient has no prohibited items, which might be carried, inadvertently or otherwise, into the chamber.
- Re-enforce ear equalization procedure.
- A nursing assessment, including vital signs and auscultating lung sounds, should be undertaken and recorded on all patients prior to each treatment. If the patient temperature is 100° F or greater, institute Policy on Hyperbaric Oxygen-Induced Seizure Prophylaxis
- Check blood glucose level if applicable
- Assessments such as ECG, ear exam, LOC, and wound evaluation as indicated/ordered.
- Provide water using a plastic water bottle.
- Encourage the patient to void prior to treatment. Provide urinal as necessary/requested.
- Connect ECG leads when in-chamber monitoring planned and ensure rhythm is visible on the monitor before closing the chamber door.
- Confirm operation or air-breathing system ensuring the non-rebreather tubing is firmly connected at the internal chamber bulkhead
- All patients being treated at pressures greater than 2.0 ATA, and all those patients considered at increased risk for oxygen-induced seizures will undergo scheduled air breaks.
Notes: Patients will be placed on the cardiac monitor during their initial treatment. EKG monitoring is recommended for every treatment in patients at high risk for CNS oxygen toxicity, and should be considered at pressures greater than 2.5 ATA.
Alarms are set to 20 +/- patient heart rate (an abrupt 20 +/- change in heart rate may be indicative of developing CNS oxygen toxicity.)
- During chamber operations with an occupant in the chamber, a CHT, CHRN, ACHRN or hyperbaric trained physician shall be physically present and shall maintain visual or audible contact with the control panel or the chamber’s occupants.
- The hyperbaric physician will provide direct supervision during the entire treatment and document in the daily progress note.
- Diabetic Patients (IDDM and NIDDM): Finger stick blood glucose checks are mandatory for all diabetic patients prior to and after hyperbaric oxygen treatment.
HBO Post-Treatment Checklist
- Visualize tympanic membranes on first time patients and in any case of patient equalization difficulty. If any barotrauma noted, notify hyperbaric physician
- Recheck patient’s blood glucose level to ensure normal levels before leaving the facility.
- Assist patient with transfer from the hyperbaric cart as needed
- Complete patient charting
- Remove patient linens from cart and discard in the proper linen receptacle
- Disinfect the chamber mattress, pillows, internal chamber acrylic
- Apply clean linens to the HBO cart and pillow
PATIENT ORIENTATION TO HYPERBARIC MEDICINE
Purpose:
To prepare the patient, family and/or significant other(s) physically and emotionally for HBO treatments.
To clearly define safety measures and outline all effects of HBO
To familiarize patients with techniques of air clearance (middle-ear-equalization of pressure)
- Assess the patient’s readiness for hyperbaric oxygen treatments.
- Ask the patient if he/she knows what hyperbaric oxygen therapy entails.
- Prior to the procedure, verify and document that the hyperbaric physician and hyperbaric staff member have discussed the risks and expectations of hyperbaric oxygen treatments with the patient and/or significant other. Risks and side effects, and complications may include:
- ear, sinus, pulmonary, or dental barotrauma
- oxygen seizures
- numbness and tingling in the fingers and toes
- visual changes (including increased cataract growth especially in diabetic and systemic steroids dependent patients, or myopia)
- diabetic hypoglycemia
- fire
- Ascertain what physician has communicated with the pateint regarding HBO
- Provide patient and/or significant other Patient Information Brochure. Document patient and/or significant other understanding of the procedure, and questions answered.
- Familiarize the patient with the purpose, effects and the procedures of HBO, anticipated beneficial effects, and safety precautions relating to his/her treatments.
- Explain the benefit of HBO to the patient's specific condition
- Answer patient’s questions regarding treatments.
- Discuss the risks and side effects
- Emphasize safety precautions to be taken.
- Restricted items include but are not limited to:
- Petroleum or alcohol based substances. No makeup, oils or hairspray allowed in the chamber
- No battery operated equipment
- Only 100% cotton gowns provided by the hyperbaric department will be worn during treatment. No personal garments or unnecessary items will be permitted.
- No objects such as paper are allowed in the chamber (fuel source)
- Familiarize patient to the HBO chamber unite and personnel
- Allow the patient and family to tour the unit. Demonstrate communication capability and diversion activities
- Discuss visiting requirements and restrictions
- Hyperbaric physician to obtain informed consent for hyperbaric treatment signed, dated and timed.
- Instruct patient on what specific medications to take and not to take while having HBO treatment as an outpatient. Coordinate care with in-house staff when inpatient.
- Screen present medications
- Notify the hyperbaric physician if medications being taken are potentially contraindicated during HBO i.e., steroids, Diamox, insulin, nicotine, hallucinogens, Vitamin C, stimulants, morphine, and digitalis. see Medications in the hyperbaric environment
- Coordinate with the nurse taking care of the patient regarding the administration of certain drugs (e.g. insulin) and the hyperbaric treatment schedule.
- Reinforce the NO-SMOKING rule
- Demonstrate auto-inflationary techniques to equalize ear pressure and encourage return demonstration
- Teach patient Valsalva maneuver (Toynbee maneuver) prior to treatment and test for effectiveness.
- If air breaks are given, have patient practice using mask prior to the first treatment in a monoplace chamber.
- Offer emotional support using relaxation techniques and a systematic patient approach to treatment. [2]
PEDIATRIC PATIENTS
Children are treated with Hyperbaric therapy for various acute and chronic indications, predominately in adult-based hyperbaric practices and facilities. The care of children in an adult care setting requires close communication between pediatric and hyperbaric specialty teams to understand the unique logistical and care needs of children required to meet the standards of pediatric care. [1]
Risks and Benefits
- There are unique pediatric-age associated complications with HBO that are roughly based on patient age groups, most commonly seen in premature and young infants. In this population, most complications focus around the development of retinopathy of prematurity (ROP), the development of bronchopulmonary dysplasia (BPD) or chronic lung disease (CLD), and premature closure of the ductus arteriosus. It has been suggested that HBO eligibility is based on the predicted maturity of the antioxidant defense system, therefore not being recommended for neonates younger than 34.5 weeks postmenstrual age and weighing less than 1.2kg. [3]
Prior to initiation of therapy, the potential risks must be weighed against the potential benefits. In general, the complications seen in older children and adolescents are similar to those in the adult population.
- Approved indications by the Undersea and Hyperbaric Medical Society (UHMS) for the use of HBO in the pediatric population are no different from those of the adult population. [3]
- Pediatric patients may be treated for elective, urgent or emergent indications.
- Treatment logistics
- An infant or toddler can be tended in the monoplace chamber unless they are ventilator-dependent. The staff member must be medically cleared to enter the chamber. Soft restraints should be used for the ventilator-dependent patient following institutional guidelines
- For pediatric patients, it is important for the staff members to remain at the chamber side during the treatment to provide reassurance and establish trust with the patient. Parents of young children should be allowed to stay close to the patient or in sight to help the child complete the therapy. [1]
- Orientation and Anxiety
- The orientation to the chamber depends on the patient's age and his or her physiological and psychological levels of maturity.
- In non-emergent situations, allowing the child to walk through the facility and observe the staff and operations with a parent can make the environment less stressful.
- Staff consistency will aid in reducing the child and parent's stress.
- Distraction during the treatment may make the environment less intimidating. [1]
- Oxygen Administration and Oxygen Doses
- Standard adult regimes of oxygen partial pressures and durations can safely be used in the care of pediatric patients. Consequently, the indications for alteration of oxygen dosage and institutions of air breaks are the same for infants and children as they are for adults. [3] [4]
- Barotrauma Prevention
- In children, as in adults, reducing the incidence of otic barotrauma is dependent on patient education and screening for Eustachian tube dysfunction.
- Middle ear barotrauma may take longer to resolve in children.
- Children may be taught the same ear-clearing techniques taught to adults. (Toynbee maneuver) Children may also drink from a plastic bottle or sippy cup to equalize ears.
- Infants may suck on a pacifier or drink from a bottle to equalize ears. The inside tender would need to burp the infant before ascent to allow any gas that has accumulated in the stomach to be expelled.
- Myringotomy tubes may be placed as needed. [1]
- Sedation and Restraint:
- Physical restraint is often required in the practice of pediatric medicine to prevent the removal of needed medical devices, such as I.V. lines, Nasogastric tubes or endotracheal tubes. Sedation may make restraining the patient more tolerable. Sedatives may not be required for all patients, and if needed, should be short-term. [1]
- Hypothermia:
- The ratio of body surface to mass increases with decreasing age, resulting in a greater relative heat loss for infants. Core temperature is a biological priority and calories will be diverted to preserve it. Evaporative cooling on ascent further increases the risk of hypothermia.
- Physical assessment of the skin (piloerection, shivering, mottling) identifies the problem when it is already present.
- The use of 100% cotton blankets or sheets can decrease the evaporative loss by preventing skin exposure to air currents. Wrapping the child's head in 100% cotton linen, reducing the chamber air flow or ventilation and redirecting the chamber air vents can help to avoid hypothermia. [1]
PREVENTION AND MANAGEMENT OF CENTRAL NERVOUS SYSTEM OXYGEN TOXICITY
Central Nervous System Effects
Grand mal convulsions caused by central nervous system (CNS) oxygen toxicity can occur in patients breathing oxygen at pressures of 2.0 ATA (atmosphere absolute) or greater. Convulsions may occur abruptly or may be preceded by other signs of central nervous system irritability. [3]
Early estimates of the seizure rate during therapeutic oxygen exposures at 2-3 ATA reported a convulsion incidence of about one per 10,000 therapies or 0.01%.
Purpose:
The hyperbaric staff will be skilled in reducing the potential for and management of oxygen toxicity for the patient receiving hyperbaric oxygen treatment.
The hyperbaric physician will be notified immediately if a patient experiences signs or symptoms of oxygen toxicity during HBOT.
Preventing seizure:
- Review past medical history including medication list
- Prescreen for
- recent doses of PCN or Phenergan, steroids
- Prior or current seizure history
- Pre-treatment temperature:
- For temperature greater than 100 degrees F, institute CNS oxygen toxicity prophylaxis procedures. May also use:
- Tylenol P.O. or rectal prior to treatment.
- Ice compresses to axilla and groin area during treatment
- Correct metabolic acidosis if indicated.
- Blood sugar levels to be checked on all diabetic patients within 1 hour prior to each treatment. see blood glucose and HBOT
Observe Patient Closely for pre-monitory signs and symptoms of CNS Oxygen Toxicity such as:
- V vision-visual changes, blurred vision, visual hallucinations
- E Ears- Auditory hallucinations, ringing in the ears
- N Nausea- May inlcude emesis
- T Twitching- Restlessness, numbness, focal twitching (note time, duration and site)
- I irritability- Change in personality
- D Dizziness- Vertigo
- C Convulsions- Seizure acitivity
- C Change in mentatio - Change in affect
- or of a non-descriptive complaint like, “I just don’t feel right” [2]
Course of Action:
- Immediately direct patient to place their air mask to their face and begin 21% oxygen breathing (air break)
- If symptoms are quickly relieved, they may represent oxygen toxicity.
- Within 1-2 minutes of the patient breathing air, ask the patient if the complaint has resolved, improved, remained the same or worsened.
- If the patient complaint has resolved or improved, the patient should complete the entire 10-minute air break. The decision to continue or abort the treatment will rest with the hyperbaric physician. It is important that the staff maintain direct visual observation of the patient throughout the ascent.
- If the patient complaint is unresolved, then have the patient continue the air break while ascending the patient to surface. At surface, the patient should be evaluated for additional etiologies such as hypoglycemia.
- To prevent future occurrences, the treatment pressure may be decreased, with additional air breaks as indicated.
- Example:
For prescribed treatment pressures @ 2.0 ATA
45 minutes 100% O2 – 10 minutes air (21% O2) – 45 minutes 100% O2
- Example:
For prescribed treatment pressures @ 2.0 ATA
30 minutes 100% O2 – 5-10 minutes air (21% O2) – 30 minutes 100% O2 – 5-10 minutes air (21% O2)- 30 minutes 100% O2 [4] [3]
In-Chamber Seizure:
- DO NOT decompress patient while actively seizing due to the expanding gas which could rupture the lung and produce a possibly fatal arterial-gas embolism.
- If the patient begins to seize during decompression, quickly turn the set pressure knob to match the chamber pressure. This will cause the chamber to stop decompression and protect the lung.
- Hold at stable pressure until normal breathing patterns have been established
- Note the time the seizure activity began and the seizure length.
- Notify the hyperbaric physician
- Pull the privacy curtain
- Once normal breathing patterns are visualized, the patient may be decompressed at a rate of 1-2 psi/min
- Remove the patient from the chamber
- Assess vital signs, LOC, blood sugar if applicable, physician evaluation
- Recover the patient with chamber cart side rails up.
- Reassure patient explaining the incident and providing reassurance
- Physician to consider adding additional air breaks or lowering the oxygen treatment pressure
Oxygen-induced seizures are usually self-limited and do not require a pharmacologic agent to terminate the seizure activity. The occurrence of an oxygen-induced seizure is not a contraindication to future HBO therapy. Administration of diazepam (Valium) before each treatment can also be used to suppress seizures. [3]
THE USE OF RESTRAINTS
Due to the unique nature of the monoplace hyperbaric chamber, which lacks a direct “hands-on” capability, restraints are occasionally used to prevent the patient who is exhibiting decreasing levels of consciousness, or agitation, from self-injury and equipment damage during the procedure. A restraint policy is also required to maintain compliance with hospital policy. [4]
Purpose:
To prevent injury while providing a safe environment for patients requiring restain during HBO treatment.
Patients with an altered level of consciousness may require the use of restraints to prevent injury. [2]
- Restraints are to be used at the discretion of the hyperbaric staff, or by physician order.
- Remove any Velcro and tape over metal on the restraint
- Patient will be under constant observation by a hyperbaric staff member.
Note: Adherence to the hospital’s “Restraint Policy” is mandatory. but can be modified to accommodate hyperbaric treatments, as noted above.
Official reprint from WoundReference® woundreference.com ©2026 Wound Reference, Inc. All Rights Reserved
NOTE: This is a controlled document. This document is not a substitute for proper training, experience, and exercising of professional judgment. While every effort has been made to ensure the accuracy of the contents, neither the authors nor the Wound Reference, Inc. give any guarantee as to the accuracy of the information contained in them nor accept any liability, with respect to loss, damage, injury or expense arising from any such errors or omissions in the contents of the work.