CLINICAL
Background
Definition:
Stomas or ostomies are surgically created openings connecting a hollow organ to the skin. It derives from the greek “stoma”, or “mouth”. There are various types of stomas, including gastrostomies, jejunostomies, tracheostomies, nephrostomies, urostomies, ileostomies and colostomies. These are created for various purposes. The most common types of diverting ostomies are ileostomies, colostomies, and ileal conduits (often referred to as urostomies).[1][2] Definitions for these common types are described below [3][4]:
- Colostomy: A surgically created opening from the colon to the abdominal wall to allow the elimination of feces. A colostomy can be either temporary or permanent.
- Ileostomy: A surgically created opening from the ileal portion of the small intestine (ileum) to the abdominal wall to allow elimination of small bowel effluent. The ileum is the third and final portion of the small intestine; it is located distally to the duodenum and jejunum and is followed by the cecum (Figure 1).
- Urostomy: A surgically created opening to divert the flow of urine by transplanting the ureters into an isolated segment of the ileum, bringing one end through the abdominal wall to create a stoma. Urine flows from the kidney to the ureters, then through the ileal conduit, exiting through the stoma

Fig. 1. Small and large intestine
Relevance:
- Prevalence: Despite the lack of solid statistics, it is estimated that 450,000 to over 800,000 individuals live with some type of stoma in the United States alone. [1][2]
- Incidence: In addition, other sources quote that approximately 100,000 to 150,000 people undergo operations that result in a colostomy or ileostomy every year.[1][2]
- Complications: Ostomy surgery continues to have high rates of surgical complications, with an unadjusted morbidity rate of 42.9% and mortality rates that have been described to be as high as 10.7%, depending on the population studied.[1][2] These complications undeniably represent a serious public health issue, considering the large population of ostomates, the large numbers of stomas that continue to be created each year, the impact the presence of a stoma creates on an individual, the potential long-term morbidity, and how proper care can make a significant difference in quality of life.
Care coordination
- The various types of stomas are created by surgeons, and depending on the type of stoma, also by gastroenterologists, urologists and interventional radiologists.
- During surgery, the creation of a stoma can be the last step of a potentially extensive operation. If well planned and placed, it can function well and be well tolerated by the patient. On the other hand, if it is not expertly placed, or if there is lack of ideal body contour (i.e. excessively thick abdominal wall, skin folds in the area of the stoma site), it can lead to complications and significant impairment in the patient's quality of life.
- Specialists such as Certified Wound, Ostomy, and/or Continence nurses (WOCN) or Enterostomal Therapy (ET) nurses are essential for preoperative and post-operative education of patients undergoing ostomy surgery.[1][2][3][5]
- In addition, coordination of care across healthcare settings for clinicians caring for an ostomate, or person living with a stoma, is essential to facilitate adaptation after stoma creation.[1][2]
General Indications and Contraindications
Indications:
Stomas are created for a variety of reasons. One of the most common reasons is to divert the fecal stream, preventing it from passing through a healing distal bowel anastomosis, allow decompression of the area and decreasing risk of anastomotic dehiscence. Indications include:
- Creation of a loop ileostomy in patients who undergo a low anterior tumor resection (removal of rectal cancers, especially if low tumors).
- Creation of an end-colostomy (Hartmann's procedure) in patients undergoing emergency surgery for perforated sigmoid colon diverticulitis and are unable to have bowel preparation before surgery.
- In addition to rectal cancer and diverticular disease, other common indications for stoma creation include fecal incontinence, refractory or recurrent anorectal infections (such as in patients with refractory anorectal fistulas), inflammatory bowel disease (Crohn’s disease and ulcerative colitis), severe radiation proctitis, and sacral/buttock pressure injuries.
- For urinary diversions, the most common reason is removal of the bladder due to cancer.
Contraindications
There are relatively few absolute contraindications to the creation of stomas. For instance, patients who cannot undergo general anesthesia due to hemodynamic instability are not candidates for colostomy or ileostomy.[6]
Relative contraindications include [7]:
- Carcinomatosis precluding mobilization of bowel
- Severe morbid obesity, such that intestinal mesentery or distal bowel limb/loop cannot reach the skin surface
- Very poor nutritional status
- Irradiated bowel with severe enteritis, due to severe inflammation, adhesions and increased risk of bowel injury
- Poor blood supply, which would increase the risk of stomal necrosis
Types of Stomas
Stomas have been traditionally created in association with an open operation. More recently, many of these operations have been performed laparoscopically or in a robotic-assisted fashion.
Although this topic focuses on colostomies and ileostomies, a general overview of other types of stoma is also provided below:
Gastrostomy
Gastrostomies are typically created with the goal of creating an access for enteral nutrition in patients who lose the ability to eat. A tube is placed through the stomach connecting it to the outer abdominal wall via a specially made device. This is usually achieved endoscopically, but also by laparoscopy, open surgery, or by fluoroscopy.
Common indications include:
- Stroke patients who are at risk of aspiration. For instance, patients with oropharyngeal dysphagia (difficulty swallowing due to stroke, other neurologic impairment or due to cachexia and debility);
- Patients who are on prolonged mechanical ventilation and therefore unable to swallow;
- Patients who have either an obstruction from an upper aerodigestive (e.g. tracheal, esophageal) malignancy, or who are expected to undergo treatment with radiation therapy involving the neck area.
In patients who cannot tolerate a gastrostomy (due to an obstruction at or distal to the stomach, or due to severe risk of aspiration of intra-gastric feeds), a jejunostomy tube is placed in the small bowel, distal to the stomach and the pylorus.
Tracheostomy
Tracheostomies are indicated in patients who require endotracheal intubation for prolonged mechanical ventilation. In these patients, an open or percutaneous tracheostomy tube is inserted. The shorter tracheostomy tube, compared to a long endotracheal tube, facilitates the aspiration of tracheal secretions. It also helps with weaning from mechanical ventilation, as patients can undergo a trial of spontaneous breathing while fully disconnected from a mechanical ventilator. It also enhances the ability to provide oral care and decreases bacterial burden of the oropharynx.
Nephrostomy
A nephrostomy involves the insertion of a tube posteriorly into the renal collecting system through the skin by image guidance. This is performed in patients with hydronephrosis due to obstructing nephro/ureterolithiasis or tumor.
Ileal Conduit
An ileal conduit is created by connecting a small segment of distal small bowel (which is excluded from the gastrointestinal tract) between the ureters and the skin. This is done in order to divert the flow of urine in patients who have their bladders surgically removed, usually due to cancer.
Ileostomy
An ileostomy may be performed to bypass the entire colon and rectum, to protect a distal anastomosis, or when the colon and rectum have been resected. It may be constructed as an end stoma or loop stoma (Figure 2).
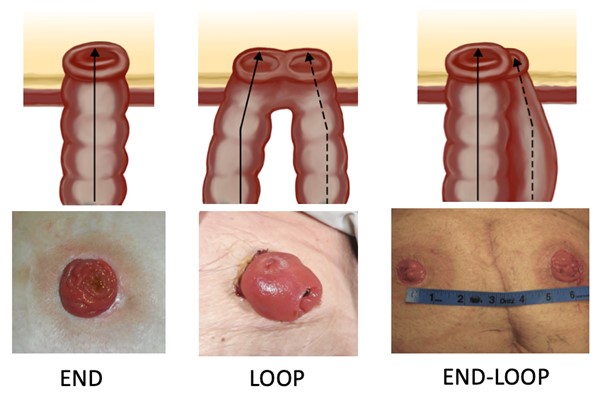
Fig. 2. Types of stoma. The end-loop type is physiologically similar to a "double barrel" stoma type, but the distal end may be separate from the proximal end (end-loop stoma by Lebedinskaya N)
End ileostomy
End ileostomies are performed in association with a partial or total colectomy. If the entire colon and anorectal sphincter mechanism is removed, the end ileostomy becomes irreversible and therefore permanent.
- Surgical technique: Following an open or laparoscopic colon resection, the premarked skin disk is excised. It is usually planned in the right lower quadrant of the abdomen, and is approximately the size of a quarter. The anterior rectus sheath is identified and incised vertically or in a cruciate fashion. The rectus muscle is split in the direction of its fibers and the posterior rectus sheath, if present at that level, is divided as well. The defect is gently stretched to accommodate two fingers. The prepared ileum is advanced through the stoma with approximately 5 cm beyond the skin level with the mesenteric edge oriented superiorly. The staple line of the ileum is excised and the stoma is matured. Since the ileostomy output tends to irritate the skin, the ileostomy is created at least 2 cm tall above the skin (referred to as "brooking"). It is important that there is no tension at the ileostomy, and that there is good viability of the bowel. The stoma appliance is placed as close to the edge of the stoma to minimize contact of the effluent to the skin.
Loop ileostomy
A loop ileostomy is usually created in order to protect a distal bowel resection, such as a low anterior resection for rectal cancer, where the anastomosis is low and associated with risk of anastomotic leak, or if the dissection is difficult, or when there is concern for a possible postoperative leak.[8] Loop ileostomies are temporary and are usually closed between eight weeks and three months after their creation, once the anastomosis is healed. In most cases, a loop ileostomy is preferred over transverse loop colostomy for temporary fecal diversion due to lower complication rates.[5][9]
- Surgical technique: The premarked skin in the right lower quadrant is excised, and a loop of distal small bowel, about 20 to 30 cm proximal to the ileocecal valve is chosen. The loop is passed through the opening created in the abdominal wall. Again, care is taken to avoid tension, twisting or ischemia. The antimesenteric aspect of the bowel is incised closer to the distal end of the loop above the skin. The distal end is matured to the dermis. The proximal end is everted similarly to the end ileostomy, allowing at least 2cm above the skin at its higher end.
More recently, the creation of loop ileostomy has been described as an alternative to a total colectomy with end ileostomy in patients with severe Clostridium difficile colitis, by performing a less extensive operation on a critically ill patient while diverting the fecal stream from the colon and allowing instillation of vancomycin into the colon via the ileostomy. [10]
Colostomy
Colostomies may also be constructed as an end stoma or as a loop stoma. They can be permanent or temporary. If the distal rectum and anorectal sphincter mechanism are still present, the colostomy may be temporary. However, if the sphincter mechanism has been removed, the colostomy will be permanent.
Loop colostomy
Loop colostomies are typically temporary and created in order to decompress the colon (e.g. due to a distal obstruction) or to divert the fecal stream proximal to a fistulous tract, inflammation, or distal anastomosis. Of note, for temporary diversion of fecal stream, guidelines recommend loop ileostomy as opposed to loop colostomy due to lower morbidity rates.[5]
End colostomy
End colostomies can be permanent or temporary. For permanent fecal diversion, an end colostomy is preferred over a permanent ileostomy, due to decreased risk of dehydration and electrolyte imbalance.
A typical scenario for a temporary end colostomy is the unprepared sigmoid colon resection, where an anastomosis is not created, such as in the perforated sigmoid diverticulitis patient.
- Surgical technique (Hartmann's procedure): the colon is mobilized by incising the white line of Toldt. The premarked stoma site is excised, the abdominal wall defect is created, and the proximal colonic stump is advanced through the opening, with care to avoid twisting or tension, and assuring good perfusion of the colon. The staple line is excised and the bowel is matured. The distal end is sutured or stapled and kept in the abdominal cavity as a nonfunctional stump. Unlike ileostomies, colostomies can be created without being everted (brooked).
Double barrel stoma (End ileostomy and end colostomy with mucous fistula: end-loop ileostomy, end-loop colostomy or end-loop ileocolostomy)
As an alternative to the above stomas, an end-ileostomy or end-colostomy can be created with the distal segment right next to it, in preparation for future reversal and/or monitoring for ischemia. For example, if a right colon resection is performed and the situation dictates the creation of a stoma, the patient may get an end ileostomy, with a small stoma including the proximal transverse colonic stump next to it. The distal stump can be left closed, or matured as a mucous fistula. This technique offers the advantage of making the stoma less bulky than loop stomas, maintain the appearance of an end stoma, and may avoid a formal laparotomy for the stoma reversal as both ends to be subsequently connected are already next to each other. If the mucous fistula is positioned at another separate site on the abdominal wall due to short length of that segment of bowel, it may require formal laparotomy for reversal.
Preparation for surgery and follow up
The importance of preoperative preparation, as well as postoperative care cannot be overemphasized.[1][2][3][5]
- Whenever possible, this should include preoperative education by the surgeon and the ostomy specialist. The ostomy specialist can provide education on the management of stoma appliances, and advise on diet, clothing, and other lifestyle modifications. In addition, the ostomy specialist can help plan the site of the stoma, which can significantly improve the quality of life of the patient after surgery and decrease postoperative complications (Figure 3).
- After surgery, the stoma specialist can again counsel on the stoma care, reinforce his/her advice on lifestyle changes, and introduce the patient to support groups. Patients can identify and avoid foods that produce an increased amount of gas, and make use of strategies to minimize odor, such as the use of deodorants for the pouch, or consumption of orally ingested deodorants, such as bismuth subgallate.
- Dietary counseling should be considered mandatory. It is especially important for patients with ileostomy, in order to thicken the effluent and to minimize short bowel syndrome symptoms.
- After discharge from the hospital, home health services are key to help patients achieve independence in ostomy management and successfully adjust to life with an ostomy.

Fig. 3. Preoperative stoma marking
Complications
Even with the best surgical and enterostomal care possible, complications related to stomas are very common. Complication rates in literature range from 20-70%.[11] Virtually every patient will experience at least some degree of peristomal skin irritation in their lifetime. Consultation with an ostomy specialists before and after surgery may reduce the rates of complications.
- Risk factors for complications include stoma type (colostomy), short stoma length, obesity, emergency surgery and lack of preoperative site marking.[12]
Stoma complications may be categorized as stomal or peristomal.[1]
- Stomal complications can further be categorized in early and late complications.[11]
- Early complications occur within the first 30 days of stoma creation and include ischemia/necrosis, mucocutaneous separation, and peristomal abscess.
- Late complications include parastomal hernia, prolapse, retraction and varices.
- Peristomal complications include skin irritation due to leakage (e.g. peristomal moisture-associated skin damage, allergic contact dermatitis, lichenification), mechanical injury, fungal/candidiasis infection, varices, folliculitis, pyoderma gangrenosum (PG), hyperplasia, and suture granulomas. Many of these problems are related to construction and placement of the stoma or inappropriate use of the pouching system.[1]
The following section focuses primarily on stomal complications. Further discussion on peristomal complications will be addressed elsewhere in Wound Reference (coming soon).
Stomal complications
Ischemia and necrosis
Ischemia can occur in up to 13% of ostomates.[13] It is most commonly associated with colostomies, emergent operation, and obesity.[11] A stoma may appear mildly dusky in the immediate postoperative period, in which case it is important to distinguish between early venous congestion and arterial insufficiency. Early ischemia is commonly associated with devascularization of the bowel conduit, oftentimes a technical issue (excessive “cleaning off” of the mesentery). Occasionally, delayed ischemia can happen. The level of ischemia can be assessed with a glass test tube inserted into the stoma and a flashlight, or with endoscopy.
- Treatment:
- If the ischemia is above the fascia and the patient is not septic, local care may be attempted.
- However, if there is concern that the ischemia extends to the level of the fascia, the surgeon should consider re-exploration and revision.
High-output and dehydration
Since the colon is responsible for a significant amount of water absorption, it is easy to understand that patients with ileostomies are more prone to high output stomas, as well as dehydration and electrolyte abnormalities. Hyponatremia is a common electrolyte disturbance resulting from high output ileostomies.
- Treatment:
- Although most patients can be managed with oral hydration, some may require a period of intravenous hydration and electrolyte replacement. The alterations in pH by loss of bicarbonate and volume loss can also make the patients prone to kidney stone formation and even acute kidney failure.
- For patients with a high output ileostomy, anti-motility agents such as loperamide or somatostatin analogues, and PPIs may be needed. Bismuth subgallate, codeine sulfate and deodorized tincture of opium have also been used for this purpose.[14] In time, the small bowel tends to adapt and the output tends to decrease. However, in patients with temporary protective loop ileostomies, consideration should be given to earlier reversal of the stoma.
- For adults and pediatric patients 1 year of age and older with short bowel syndrome who are dependent on parenteral support, FDA-approved teduglutide may be administered. Teduglutide is an analog of glucagon-like peptide 2 (GLP-2) that increases intestinal absorption. Subcutaneous teduglutide (0.05 mg/kg once daily) has been shown to improve intestinal absorption and reduce parenteral support requirements in patients with short bowel syndrome.[15] These patients should be followed at tertiary care centers with short bowel clinics. It is helpful to measure urine output to assess dehydration status pre and post implementation of these drugs. Measuring urine sodium is a helpful test to determine if the loss is pre-renal or secondary to renal compromise.
Stoma retraction and stenosis
Stoma retraction may occur due to ischemia, and/or inadequate bowel mobilization leading to tension on the mucocutaneous junction and subsequent separation or inversion (Figures 4-6). Early postoperative mucocutaneous separation and stoma retraction will commonly result in late term stoma stenosis, as the wound tends to contract as it heals. Fascial stenosis may lead to a stenotic stoma.
- The rate of stoma retraction ranges from 1-30%; the presence of retraction is associated with colostomies and emergency operations.[11]
- The rate of stenosis ranges from 1 to 9%.[13] An attempt may be made to dilated the stoma aperture locally, or otherwise stenosis correction may be accomplished through laparoscopy or laparotomy.
- Although use of a bridge/ rod for loop ostomies may seem an intuitive way to decrease retraction (Figure 7), a recent meta-analysis suggests that placement of a rod does not reduce the incidence of retraction and instead leads to increased rates of dermatitis and stoma necrosis.[16] Other factors such as abdominal wall thickness, patient comorbidities, excessive tension may play a larger role in such complications.[16] The use of a bridge does not replace careful surgical technique to avoid excessive tension.

Fig. 4. Necrotic, retracted end colostomy (post multiple revisions and relocations)
| 
Fig. 5. Necrotic loop ileostomy (by Lebedinskaya N)
|

Fig. 6. Necrotic, retracted stoma with visible mucocutaneous separation (by Lebedinskaya N) | 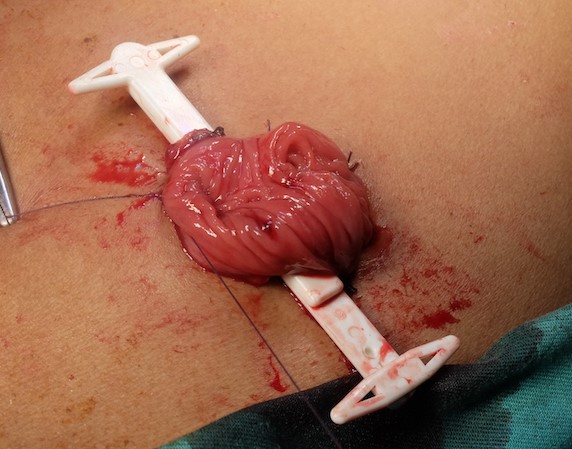
Fig. 7. Rod (or bridge) placed under the loop of intestine |
Prolapse
Stoma prolapse (Figures 8 and 9) can occur in 3% of ileostomies, 2% of colostomies, and 1% of urostomies.[11][17] However, the risk of prolapse has been reported to be as high as 11.8% at 13 years.[18] Transverse loop colostomies tend to be associated with higher rates of prolapse, and thus are not commonly performed.
- Treatment:
- Smaller prolapses are managed without surgery.
- However, if the prolapse is associated with ischemia, obstruction, or other issues, surgical intervention is recommended. The stoma is reversed if possible, or the stoma can be freed up and delivered until taut. The redundant bowel is excised and the stoma re-matured. In the case of a loop colostomy, conversion to an end colostomy with or without a mucous fistula can be performed.
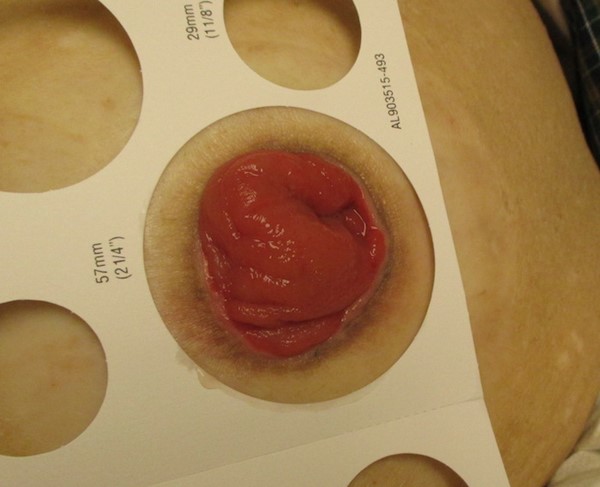
Fig. 8. End stoma prolapse (by Lebedinskaya N) | 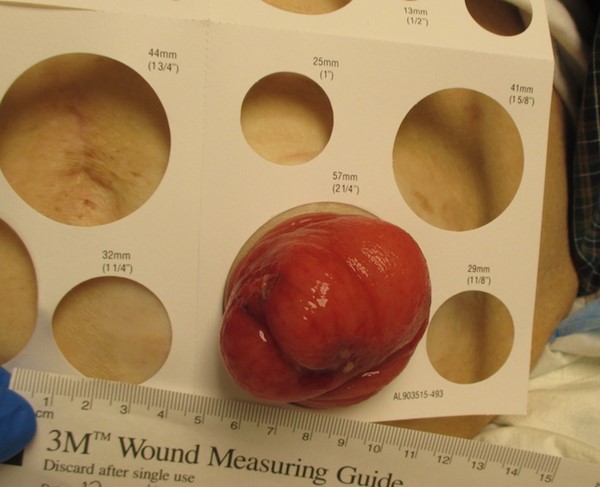
Fig. 9. End stoma prolapse, Valsalva maneuver (by Lebedinskaya N) |
Parastomal varices
Parastomal varices (Figure 10) can cause significant bleeding in patients with portal hypertension. It can occur at the mucocutaneous junction when the low-pressure subcutaneous veins join the higher pressure veins from the bowel in patients with liver cirrhosis. Parastomal varices can happen in patients with cirrhosis of any etiology, including alcoholic cirrhosis, and also in patients with colorectal cancer and extensive liver metastasis, or sclerosing cholangitis associated with inflammatory bowel disease. This is a rare but potentially life-threatening complication, and therefore a high index of suspicion is very important and can be life-saving. The ideal scenario is to avoid stoma creation in patients with portal hypertension altogether.
- Treatment:
- If peristomal varices are suspected, careful physical exam after gentle removal of the ostomy appliance is imperative. Varices are characterized by a purplish hue or caput medusae of the peristomal skin.
- It can be transiently treated with sutures, cautery, compression, or topical application of vasoconstricting agents.
- Percutaneous embolization with sclerosing agents has also been described. More durable options include transjugular intrahepatic portosystemic shunt (TIPS procedure) or liver transplantation.
- In patients with severe bleeding and short life expectancy, one option is to create a mucocutaneous disconnection, by freeing the stoma from the skin and subcutaneous layer down to the level of the fascia.

Fig. 10. Peristomal varices (by Lebedinskaya N)
Parastomal hernia
Parastomal hernia is the most common stoma complication requiring operative intervention (Figure 11). Incidence varies according to the stoma type and configuration (1.8 to 28.3% for end ileostomies, 0 to 6.2% for loop ileostomies, 4 to 48% for end colostomies and 0 to 30.8% for loop colostomy).[11][19] It is however, important to keep in mind that the reported incidence in parastomal hernias depends not only on the types of stomas, but on the length of follow up as well. Parastomal hernias often develop within the first 2 years, but may occur years later.[11]
- Risk factors: risk factors for parastomal hernias include obesity, chronic obstructive lung disease, corticosteroid use, postoperative sepsis, abdominal distention, constipation, excessive splitting of muscle fibers or opening of the fascia when constructing the stoma, placing the stoma in an incision, emergency surgery, premature use of abdominal muscles by the patient leading to increased intraabdominal pressure (e.g. lifting heavy objects, exercising before being cleared by surgeon).[11]
- Diagnosis: most parastomal hernias are diagnosed by physical exam with the patient standing. If the diagnosis is ambiguous, then a computed tomography scan can be performed.
- Treatment: parastomal hernias can impair the patient's quality of life, but are generally well tolerated.
- Indications for surgical repair:
- Absolute indications for surgical repair of a parastomal hernia include obstruction, as well as incarcerated hernia with strangulation.
- Relative indications include incarceration, prolapse, stenosis, large size, difficulty with appliance management, and pain.
- Parastomal hernias can be repaired through a local repair (open primary fascial repair), stoma relocation or parastomal hernia repair with mesh. The best treatment, however, is the reversal of the stoma if feasible, as the recurrence rates of parastomal hernia repair are very high.
- Recurrence rates can be as high as 75% with primary suture repair, 24 to 86% with stoma relocation, or 33% with mesh repair.[19][20][21]
- Due to its high recurrence rate, primary suture repair is not recommended in most cases.[22] Evidence shows that use of mesh in parastomal hernia repair significantly reduces recurrence rates. Mesh repair has been described using a keyhole shaped mesh, or the Sugarbaker technique.
- With the keyhole technique, a slitted mesh with a 2-3cm central hole is placed surrounding the stoma intraperitoneally (mesh is C-shaped, with a central opening for the bowel).
- With the Sugarbaker technique, the fascial defect is widely covered by the mesh, except for one side where the stoma conduit traverses between the mesh and peritoneum (mesh is a solid circle and hammocks the bowel between the abdominal wall and the mesh, covering the defect). In laparoscopic parastomal hernia repair, the Sugarbaker technique has been described to be superior over the keyhole technique, showing fewer recurrences.[22]. However, the technique was described using ePTFE, a type of mesh that is not as widely used due to lack of integration, but which may be associated with less mesh erosion when used with this technique.
- For patients who are not surgical candidates, the patient should be measured and fitted for a specialty ostomy hernia belt (e.g. Nu Hope, Brava).

Fig. 11. Parastomal hernia (by Lebedinskaya N)
Peristomal complications
Skin irritation and leakage
Skin irritation is very common, and to some degree it may be inevitable (Figure 12). However, severe skin irritation can be prevented. As mentioned, careful planning of stoma location and application of the appliance is paramount. Elderly patients may need help with the care of the stoma, and obese patients may benefit from a stoma placed higher in the abdomen so they can inspect and change their appliance more easily. Patients typically need guidance from the ostomy specialist to develop a routine that will avoid leakage from the ostomy appliance.

Fig. 12. End ileostomy with severe peristomal irritant contact dermatitis with fungal component and lichenification
Further discussion focused on peristomal complications will be addressed separately in Wound Reference (coming soon).