CLINICAL
Overview
This topic provides an overview on the use of compression therapy in the treatment of VLU (not for lymphedema). VLU is discussed in detail elsewhere (see "Venous Ulcers"). For more details on compression subtypes please see “Compression Bandages”, “Tubular Dressings (Bandages)”, "Gradient Compression Stockings" and “Dynamic or Intermittent Compression”. For decision support on choices for effective compression therapy see "How to Select Adequate Compression Therapy Pressure Levels and Products". For information on major brands of compression devices, see "Compression Brands Quick Reference".
Background
- Compression therapy is considered the mainstay of VLU treatment [1] and, along with standard care, has the potential to heal 50%-75% of VLUs [1][2].
- Compared with people with VLU who do not utilize any compression, people with VLU who utilize compression bandages or stockings are more likely to experience complete wound healing more quickly, have their VLU completely healed, experience less pain and better quality of life [4].
- Despite existing references and guidelines, many patients with VLU who are treated in primary care settings do not receive compression therapy. In Europe records indicate that only 10-53% of patients with VLU receive adequate compression therapy [3]. In contrast, there is evidence that at European specialist centers, up to 88% of patients with VLU may receive compression therapy [5].
- A 2010 study by the U.S. Wound Registry showed that patients with venous ulcers were provided adequate compression in fewer than 17% of visits, even at hospital based outpatient wound centers. [6]
- Some of the reasons why compression therapy is underutilized are: lack of knowledge or confidence by clinicians, unclear referral pathways because of the variety of specialties that may be involved, local unavailability of compression bandages or hosiery and unwillingness of patients to wear compression therapy [3].
How the intervention works
- Most VLU are associated with chronic venous insufficiency, however the etiology of VLU is not yet fully understood [1] [7]. Chronic venous insufficiency has been shown to be associated with venous hypertension [8], which most often results from thrombosis and/or valve disease affecting the superficial, perforator or deep veins [2]. In individuals with healthy venous valves, calf muscle contraction during ambulation (muscle pump) reduces the intravenous pressure at the ankle. However, in venous dysfunction intravenous pressure remains high, resulting in ambulatory venous hypertension (Video 1, Figure 1) [9] [10]. Venous hypertension results in inflammatory alterations with microcirculatory changes that can culminate in edema, venous stasis and VLU [11].
Video 1. Muscle pump
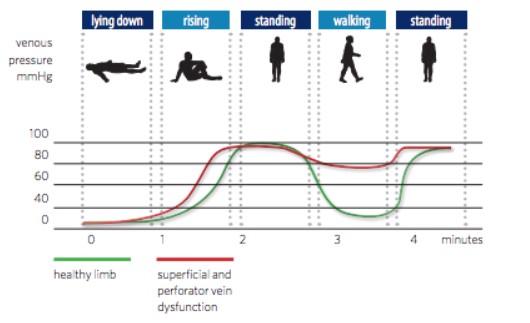
Figure 1 – Changes in pressure (measured at the ankle) in venous system of individuals with healthy and dysfunctional venous valves during lying, rising, standing and exercise
- External compression has been used in an attempt to reverse venous hypertension and aid venous return [8]. Venous stasis and edema can be reduced by effectively applying external local compression which facilitates reabsorption of fluid from the interstitium into the lymphatics (Figure 2) [9]. This phenomenon has been described by the Starling equation (Figure 3) [9] [12].
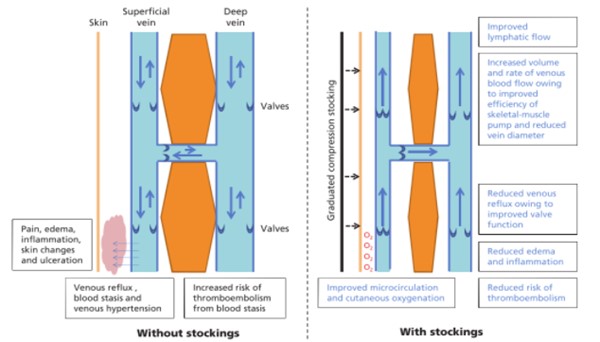
Figure 2. The mechanism of action on compression
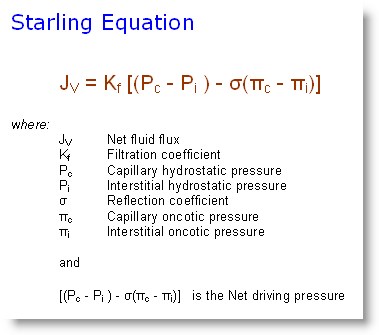
Figure 3. Starling equation
-
Working pressure and resting pressure: to understand how compression therapy works, it is necessary to understand the difference between working and resting pressure [13].
-
- Resting pressure is the result of compression of the extremity at rest. It corresponds to the force exerted by the bandage when the muscles are relaxed.
- Working pressure is the pressure generated through the interaction of muscle contraction and the compression bandage when walking; it results from the resistance the bandage exerts to counteract muscle movement. The less the bandage yields in this process, the higher the working pressure and the stiffer/inelastic the bandage is.
- Both kinds of pressure depend on several factors. Given that the working pressure is generated by active muscle contraction, it is always higher than the resting pressure.
- Factors that affect pressure:
-
- Compression device-related:
-
- Material used: inelastic components have high stiffness and so usually produce lower resting pressures but higher working pressures.
-
Number of components applied: stiffness increases with the number of components applied. Although the single components of multi-component bandages (e.g, 4 layer bandages) are elastic, the final product has properties of an inelastic bandage [14].
-
Patient-related: calf muscle and foot pump function, shape of the limb, ability to tolerate compression [3].
-
Clinician-related: pressure applied and application skills. Many clinicians are not familiar with compression therapy in general [15]. Compression application skills and available resources can affect sub-bandage pressure (i.e., pressure measured underneath the [2]. Even clinicians who are confident in their ability to apply compression can apply compression in a suboptimal way [16][17]. Some bandages offer visual guides that indicate proper application of the device.
- Other important facts about compression, explained by 2 physical laws: Pascal's law (Figure 4) and Laplace's Law (Figure 5) [9]
-
- The same tension applied at the ankle will generate more pressure than if applied at the calf, due to the smaller radius at the ankle [18].
- More layers of elastic compression bandaging incrementally increase compression and result in a less elastic bandage. This is in part due to friction between the layers [19].
- The calculated value for sub-bandage pressure is the average pressure that will be exerted by a bandage on a limb of known circumference. Padding can be applied beneath compression bandages to reduce local variations in sub-bandage pressure [18].
- Bandage width matters. A 10cm wide bandage applied with a total force of 'F' Newtons will produce only half the pressure a 5cm wide bandage applied with the same force, as the force is distributed over twice the area [18].
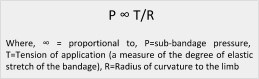
Figure 4. Pascal’s Law: external static pressure exerted on a confined fluid is distributed evenly
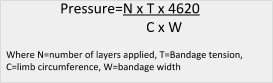
Figure 5. Laplace’s Law. Pressure applied by compression is proportional to the tension at the interface with skin and inversely proportional with limb radius
Compression levels
-
Sub-bandage pressure is measured in mmHg at the ankle level. Classification of pressure exerted by compression devices varies across countries. Pressure measured in vivo in the medial gaiter area in the supine position for training purposes may be classified into the following categories (Table 1) [20]:
Table 1. Pressure measured in vivo in the medial gaiter area in supine position for training purposes, as per the International Compression Club [20]
| Classification |
Pressure (mmHg)
|
|
Mild
|
<20
|
|
Moderate
|
=20-40
|
|
Strong
|
=40-60
|
|
Very strong
|
>60
|
General Indications and Contraindications
Indications
- Chronic venous insufficiency (including manifestations ranging from varicose veins to VLU)
-
- Different pressure levels are indicated according to the severity of the diseased being treated [9]. The CEAP (Clinical - Etiology -Anatomy - Pathophysiology) classification system has been used to standardize documentation and description of the manifestations of chronic venous disease. The C (Clinical) category is divided as shown in Table 2. Table 3 summarizes indications and pressure levels commonly used in compression therapy for chronic venous disease.
- Lymphedema (recommend referral to lymphedema specialist). See topic " Lymphedema - Treatment and Emerging Strategies for Prevention"
- Post-thrombotic syndrome
- Prevention of deep venous thrombosis [9]
Table 2. CEAP (Clinical - Etiology - Anatomy - Pathophysiology) Classification
- C0: No visible or palpable signs of venous disease
- C1: Telangiectasies or reticular veins
- C2: Varicose veins
- C3: Edema
- C4: Changes in skin and subcutaneous tissue divided into two subclasses:
-
- C4a Pigmentation or eczema
- C4b Lipodermatosclerosis or atrophie blanche
- C5: Healed venous ulcer
- C6: Active venous ulcer
|
Table 3. Chronic venous insufficiency and compression pressure levels
| Condition |
Recommended pressure levels (sub-bandage, at the ankle)
|
|
Active VLU (C6) with no contraindications to compression
|
30-40 mmHg [21][22][23]
|
|
Healed VLU, to reduce recurrence (C5)
|
Highest pressure patient can tolerate, ranging from 18-35 mmHg. VLUs tend to recur less with higher pressure, however patient adherence is lower compared to lower pressure levels [1][24]
|
|
Varicose veins and edema (C2, C3)
Skin and subcutaneous changes (C4)
|
30-40 mmHg [25], however even low levels of compression (10-20 mmHg) can improve symptoms and edema [24]
|
|
Simple varicose veins (C2)
|
20-30 mmHg [22]
|
Contraindications
-
Severe peripheral arterial disease (PAD): all patients should be screened for arterial disease using Doppler measurement of the ankle-brachial pressure index (ABI) or Doppler continuous waveform analysis [26] by trained staff before receiving compression therapy [1]. Inadequate compression on a limb compromised by arterial disease can lead to ischemic sequelae and tissue necrosis [27]. ABI below 0.8 is often considered clinically significant PAD.
-
- Patients with ABI between 0.5 and 0.8 may be eligible to receive modified (reduced) compression (20-30 mmHg at the ankle), pending vascular assessment and/or indication by a vascular specialist [1][28].
- Patients with ABI below 0.5 or above 1.3, ankle pressure < 50 mmHg or toe pressure < 30 mmHg should not receive compression unless ordered by a physician and supervised by a vascular specialist [3][27][28].
-
Unstable congestive heart failure (CHF) with pulmonary edema: CHF and hemodynamic condition need to be under control prior to commencing compression, as heart can be overloaded once fluid is mobilized and leg edema starts to subside [3]. Signs and symptoms of unstable CHF and pulmonary edema include: significant peripheral edema, dyspnea, altered mental status, decreased diuresis, tachycardia, hypoperfusion, markedly elevated neck veins and rales heard with lung auscultation [29].
-
Acute DVT: if present, acute DVT needs to first be treated with anticoagulants for 7 days before compression therapy is started [30].
-
Untreated cellulitis: if present cellulitis needs to first be treated with systemic antibiotics for 24 hours and the patient should be afebrile before compression therapy is applied [3]. Patients can receive reduced compression if standard compression is difficult to tolerate. Dressing change frequency can be increased to monitor infection.
Types of compression therapy devices
- Adequate compression can be achieved by several methods, including use of a single component or layer (such as a compression stocking or one type of bandage) or using multiple components or layers (different types of bandages or stockings and bandages used together) [1][31]. Overall, evidence shows that multi-component systems are more effective than single-component systems. High compression is more effective than low compression, but among different types of high compression no clear differences have been observed [1].
- All patients who are candidates for compression therapy should have their ABI, doppler waveform or toe brachial index (TBI) measured and recorded [3]. Assessment of arterial blood supply with these tests is a major determinant of the pressure level of compression to be applied. Other factors that influence choice of compression devices are: clinician’s preference and experience, wound status, exudate level, patient mobility, ability of the patient to self-apply compression, patient’s preferences, pain level, access to care, level of compression required, and availability of compression systems [3]. For decision support on choices for effective compression therapy, see "How to Select Adequate Compression Therapy Pressure Levels and Products". For information on major brands of compression devices, see "Compression Brands Quick Reference".
- In general, compression devices for treatment of VLU can be classified as static or dynamic:
-
-
Static: Compression bandages and gradient compression stockings are forms of static compression and apply a constant pressure gradient from distal to proximal in the extremity [3][32]. This gradient of a 20–30% reduction in pressure from ankle to below knee is thought to aid venous return to the heart and occurs naturally when compression is applied to a limb of normal proportions due to the principles of Laplace’s Law [32]. Patients with altered limb shape, such as inverted champagne bottle shape, may require reshaping of the limb with padding prior to the application of compression in order to benefit from graduated compression. However, it is not clear how important this gradient is, especially for mobile patients [32].
-
Dynamic: Intermittent pneumatic compression (IPC) is an example of dynamic compression. The sequential inflation and deflation of the chambers creates intermittent pressure peaks, mimicking the effect of the calf muscle pump and offering a number of benefits. It may be useful for patients with reduced mobility or wasting of the calf muscle [32].
- Static or dynamic compression devices can be elastic, inelastic or a combination of both:
-
-
Elastic: elastic systems (also known as “long stretch”) contain elastomeric fibers and are capable of stretching and returning almost to their original size. They can sustain pressure for up to a week due to their ability to accommodate changes in limb shape and movement [10][32]. Elastic compression provides compression when patients are either walking or resting, which may not be desirable in patients with PAD [2].
-
Inelastic: inelastic systems contain no or few elastomeric fibers. They include “non-stretch” materials, such as zinc paste bandages, and “short-stretch” materials, which have a minimal extensibility (SSB) [32]. Inelastic systems can maintain levels of 30-60 mmHg in the first 24 hours after application, but this level decreases with movement of fluid and edema reduction. Most multi-component systems (two and four-components) function as an inelastic system even if they contain mainly elastic components [10]. Inelastic systems will produce higher pressures during standing and lower pressures when lying down than elastic systems [2] [10] making it more desirable in patients with mild arterial insufficiency [2].
-
Combination: compression system composed of both elastic and inelastic materials. Multi-component layers (e.g. Profore) behave as an inelastic or high stiffness system [14].
- High or low stiffness:
-
- Single or double-layer bandages are characterized by use of the terms ‘‘elastic and inelastic". Final behavior of kits or systems (e.g., multi-component systems) is characterized as ‘‘high or low stiffness’’ [20]. Stiffness may be characterized by the increase of interface pressure measured in the gaiter area when standing up from the supine position [20].
- High stiffness: Inelastic behavior. A pressure increase of > 10 mmHg measured in the gaiter area when standing up from supine position is characteristic of a stiff bandage system [20].
- Low stiffness: Elastic/long stretch behavior. A pressure increase of < 10 mmHg measured in the gaiter area when standing up from supine position.
-
Table 4 below summarizes characteristics of the different types of compression devices. For guidance on selecting compression pressure level, see "How to Select Adequate Compression Therapy Pressure Levels and Products". For examples of different brands, see "Compression Brands Quick Reference".
Table 4. Types of compression devices, their stiffness and indications. (*) Stiffness listed as classified by Dissemond et al [13]
Types of devices with examples / stiffness (*)
|
Beneficial to
|
Comments
|
|
Static
|
|
Compression bandages
|
Elastic:
- Long-stretch (Shur-Band, EZe-Band)
|
Low stiffness |
Elastic bandages are beneficial to individuals who do not ambulate or who have reduced mobility [30][33]
|
Not desirable for patients with PAD
|
|
Inelastic:
- Non-stretch (Gelocast Unna Boot)
- Short-stretch (Rosidal K, Comprilan, Coban 2, Coban 2 Lite)
|
High or very high stiffness
|
Inelastic bandages are useful when frequent dressing changes are needed due to weeping or when there is pressure damage from elastic bandages [30][32], and for patients with mild/moderate PAD [2]. Not indicated for patients with reduced mobility as it requires functional muscle pump to be effective [33].
|
Inelastic bandages may be more adequate for patients with mild PAD [2]. Inelastic systems can maintain 30-60 mmHg in the first 24 hrs, but decreases with movement and edema reduction [10][32].
|
|
Multi-component
(Profore, Profore Lite)
|
High stiffness |
Clinical guidelines suggest multi-component compression systems with an elastic component (4LB) as the first choice of initial therapy for most patients with VLU with no contraindications [1][34]. Even with elastic component, a 4LB behaves as a high stiffness, inelastic system.
|
4LB has been shown to be more cost-effective than multi-component compression systems without an elastic component in the U.K. [35][36]. In practice, patient adherence to 4LB may be lower than to 2LB. Most multi-component compression systems are designed to deliver 40 mmHg at the ankle, decreasing to around 17 mmHg at the calf.
|
|
Tubular Dressing
|
Elastic (Tubigrip)
Inelastic (Juzo Cotton Stockinette)
|
Low or high stiffness |
Patients with VLU who cannot tolerate high pressure levels or patients with PAD and ABI between 0.5 and 0.8
Patients with VLU who require frequent daily dressing changes [37]
|
Tubular dressings can provide either uniform or graduated compression.[1] They can be used as a single layer or more layers can be added, offering incremental pressure.
|
|
Gradient Compression Stockings
|
Elastic
(Ulcercare)
|
Moderate stiffness |
Patients with CEAP C0-6 (different levels of compression needed)
Prevention of new or recurrent VLU, healing of VLU
Can be used as a first-line treatment for patients with small, uncomplicated ulcers who wish to self-care and who find bandages too hot or bulky [32] and patients without morbid obesity, lipodermatoesclerosis or severe edema [38]
|
Custom fitt stockings may provide adequate compression to patients, however they are difficult to don and may lead to low adherence to therapy [39]
Two-layer compression stockings (HH) that deliver 40 mmHg are as effective in healing VLU as 4LB and they appear to have additional benefit of reducing recurrence rates and being more cost-effective [38]
|
|
Gradient Compression Wrap
|
Inelastic (ReadyWrap, Circaid Juxtacures)
|
High stiffness |
Patients who are unable to wear 35 to 45 mmHg gradient compression stockings because of weakness or arthritis or those who are unable to tolerate inelastic non-stretch compression bandage (e.g. Unna boot) [40]
|
Inelastic compression provided by Velcro bands, can be adjusted as limb swelling decreases. Provides higher working and lower resting compression levels with low-stretch materials. A lower resting compression level can make it more tolerable to patients
|
|
Dynamic
|
|
Intermittent Pneumatic Compression
|
n/a
(Flowtron)
|
n/a |
Patients with VLU who cannot wear or tolerate any of the other compression methods due to severe PAD, excessive pain, pressure damage [30], severe difficulty in donning compression stockings or have failed to respond to prolonged compression therapy alone [27][41]
Patients with VLU with reduced mobility or wasting of the calf muscle [32]
|
Whereas it is advantageous to use IPC compared with no compression therapy, currently there is limited evidence to suggest that the addition of IPC to compression therapy offers benefit [27] [42]
Pressure levels are generally set to 50 mmHg but are never greater than diastolic pressure [33] |
Evidence and Recommendations
Please see “Venous ulcers” section on 'Compression' for rationales and summary of evidence supporting the recommendations below.
-
1B
For VLU patients with no contraindications we recommend compression over no compression therapy to promote wound healing (Grade 1B).
-
2B
As for initial choice of compression therapy, we suggest multi-component compression bandages over single-component compression bandages (Grade 2B).
-
2B
Two-layer gradient compression stockings (HH) that deliver 40 mmHg pressure at the ankle can be considered an effective alternative to multi-component compression systems (4LB) (Grade 2B).
-
2C
Intermittent pneumatic compression (IPC) therapy can be used when all other compression therapy methods have failed or on patients that do not tolerate multi-component compression systems or high compression gradient stockings (Grade 2C).
-
2C
To decrease risk of ulcer recurrence in patients with a healed VLU, we suggest compression therapy with gradient compression stockings at the highest pressure patients can tolerate (Grade 2C).
Practice Tips
CHOOSING AN IDEAL COMPRESSION DEVICE
- With the goal of achieving optimal sub-bandage pressure and gradient compression, clinicians should choose the type of compression device according to availability of resources, clinicians’ experience and familiarity with the compression method, characteristics of the ulcer, patient preference and support from caregivers. For decision support on choices for effective compression therapy see "How to Select Compression Therapy". For information on major brands of compression devices see "Compression Brands Quick Reference".
GETTING A HEAD START ON REDUCING EDEMA
- If a patient with VLU has significant edema and no CHF, and resources and time are available, a quick course of high pressure compression (e.g., with Ace wrap) can be applied to the patient’s leg for 10-20 minutes in the clinic before applying the dressings and compression bandages/stockings/wrap that the patient will go home with. Practitioners have seen patients lose 1-2 cm in leg diameter with the addition of this step.
COMPRESSION THERAPY FOR CASES THAT ARE HARD-TO-ASSESS and/or Hard-to-MANAGE
- For patients with CHF or history of CHF: if patient is stable, modified compression should be applied as long as patient is being treated and under control. If needed, diuretics can be increased upon application of compression for the first time and patient should be reassessed within 24-48 hours.
- For patients with PAD and ABI between 0.5 and 0.8: use reduced level of compression (20-30 mmHg at the ankle) and closely monitor for complications. If resources are available and if uncertain about whether compression can be applied, clinicians can measure toe pressure with the patient lying in dorsal decubitus before and immediately after application of modified compression (e.g., SSB like Coban™ 2 Lite). Clinicians have reported increased toe pressure after SSB application.
- For patients with acute DVT: ABI can be performed as long as the first dose of anticoagulation has been given.[43]
- For patients with high body mass index (BMI) or large limbs [43]: main challenges are to overcome immobility and venous hypertension in the lower limb and abdomen. The solution is often to commence and/or continue high compression in the absence of contraindications. Assessment can be facilitated if the service is prepared with appropriately sized equipment (e.g. probes and cuffs for ABI measurement, hoists for mobilization). If patient's leg has skin folds that hamper application of compression bandages or abnormally shaped limb, consider inelastic compression bandaging with additional sub-bandage padding to address skin folds and contour irregularities.
- For very tall patients (defined as over 6 foot/182 cm) [43]: the goal is to combat a higher hydrostatic pressure with a higher sub-bandage pressure (i.e. at least 40 mmHg). A custom compression kit or longer bandage may be needed if the length between ankle to knee is longer than average.
- For patients with impaired mental capacity or ability to understand [43]: these patients may not understand the need for compression bandages and may thus try to remove them. Some tips to decrease likelihood of removal include:
- Finish bandage at the back of the leg
- Encourage the patient to wear paints rather than skirts or shorts, and wear loose socks over compression bandaging
- Apply a tubular bandage on top of bandage and tape in place
- For patients with recalcitrant VLUs (i.e., VLU that failed to reduce in size by more than 25% in 8 weeks of adequate treatment), and with painful ulcers that limit the use of conventional compression bandaging, or of mixed etiology: IPC applied to the lower extremity or thigh-administered IPC may be considered. In one non-randomized pilot study, thigh-administered IPC device applied daily for at least 2 hours per day, in addition to standard therapy led to improved VLU healing. [41]
Risks and Complications
Most complications due to compression therapy are avoidable if appropriate measures to mitigate risks are taken. If complications arise, it is important that they be addressed promptly. Below are some of the complications and a few practical suggestions to manage them [32]:
- Pain: compression, when applied appropriately should reduce pain. However, effective compression may cause initial discomfort and anxiety. Suggestions based on expert opinion include:
-
- Rule out any other causes of pain, such as PAD-related pain. Teach patient to recognize signs of PAD (e.g., changes in limb color/perfusion)
- Ensure local wound care is done properly (see “Venous Ulcer” section on ‘Local Wound Care’)
- If pain is related to compression: offer analgesics during the initial phase (1-2 weeks) until discomfort subsides or stage compression (start with a lower pressure level)
- If pain remains uncontrolled, perform full reassessment (see “Venous Ulcer” section on ‘Plan Reassessment’)
- Pressure Damage: signs of pressure damage resulting from compression therapy are erythema, blistering, altered/uneven limb shape. Among the risk factors are: patients with impaired peripheral perfusion, thin or altered limb shape, foot deformities, reduced sensation/pain sensation, long-term systemic steroid use and presence of a chronic disease (e.g., rheumatoid arthritis) associated with reduced mobility, loss of calf muscle and foot/ankle deformity. Suggestions based on expert opinion include:
-
- Avoid strong, sustained compression. Consider using inelastic compression or IPC associated with hosiery
- Apply extra padding over bony prominences
- Ensure overlap is even mainly at the dorsum of the foot, ankle and calf
- Loss of calf muscle: may be seen in patients receiving long-term compression, most likely due to reduced patient activity and underlying comorbidities (as opposed to compression itself). Suggestions based on expert opinion include:
-
- Ensure compression allows patient to flex knee and ankle at or near 90 degrees
- Ensure shoes do not restrict patient’s ankle range of motion (flat, comfortable shoes are preferred)
- Encourage calf muscle exercise
- Skin problems: can arise due to excessive exudate or allergic reactions. Suggestions based on expert opinion include:
-
- Fungal infection: excessive exudate can lead to fungal infection. Fungal infection needs to be treated to resolution before reapplication of occlusive dressings and compression. Prevent fungal infections by adequately managing exudate (see local wound care) and increasing frequency of dressing and compression system change until exudate is controlled.
- Contact dermatitis: susceptible patients may develop contact dermatitis from one of the components of the compression system (e.g., latex, zinc, wool). Remove irritant or use a cotton stockinette liner or paste bandage against the skin to avoid irritation from wool padding.
Patient Adherence
- Many patients cannot tolerate, or do not adhere to, compression bandaging therapy [44]. It is estimated that 60-70% of patients do not appropriately adhere to compression therapy [45][46]. Patients might find it difficult to tolerate compression due to several reasons, such as bandage bulk, lifestyle, climate or cultural factors [32]. Patients with obesity, frailty or arthritis will struggle to apply elastic compression stockings. Also, patients’ beliefs that compression is unnecessary and uncomfortable, or conversely that is worthwhile and prevents recurrence, affects adherence or non-adherence [47]. Thus, adherence can be improved by educating patients on the importance of compression therapy [48], and also by properly selecting the best compression alternative for each patient.
- Below are some practical suggestions based on expert opinion to aid in patient adherence [3]:
-
- Determine reasons for non-concordance and address any modifiable reason
- Consider implementing lower level of compression and gradually increasing to a level that is tolerable for the patient
- Consider the use of compression hosiery, tubular compression or IPC associated with hosiery
- Limit bulk around the ankle/foot
- Bandage protector to enable bathing/showering
Transitioning to Stockings
Once VLUs are healed, to decrease risk of ulcer recurrence clinical guidelines recommend compression therapy with gradient compression stockings at the highest pressure patients can tolerate [49][50].
- For simple VLU, when adherence is not an issue and patient is able to don gradient compression stockings: as ulcer is decreasing in size and complete healing is likely in about 2 weeks, gradient compression stockings can be prescribed and ordered (covered by Medicare if ulcer is active, not healed). After ulcer is healed, compression bandages may continue to be applied for 1-2 weeks to avoid damaging fragile newly healed area.
- For complex VLU, mixed etiology leg ulcers or when adherence is an issue: consult edema management specialist (e.g., physical therapist) early on (e.g., after initial evaluation), as patient education and choice of long-term compression according to patient preference and life-style may take several weeks.
- See indications, contraindications and how to use gradient compression stockings in " Compression: Gradient Compression Stockings".
PATIENT EDUCATION FOR CLINICIANS
- VLU are a chronic, long-term problem with recurrence rates as high as 70%. Therefore, long-term maintenance must be addressed even for healed ulcers [50]. See “Venous Ulcers” section on ‘Patient Education’ for details on patient education for VLU healing, prevention of new VLU and prevention of recurrence.
- We recommend sharing our patient education materials with VLU patients (for all materials, see Patient Education Materials).
Compression therapy patient education materials:
- Patient Education - Venous Leg Ulcers
-
Gradient Compression Stockings for Patients
Related Patient Education materials:
- Basic Principles of Wound Care (handout)
- Chronic Ulcers (handout)
- Debridement (handout)
- Nutrition (handout)
- Showering Instructions (handout)
- Smoking Cessation (handout)
- Ulcer Infection (handout)
CODING AND COVERAGE
This section provides an overview of how the different compression modalities for management of venous leg ulcers are coded and covered by Medicare in the United States. For detailed coding and coverage information for each compression subtype, please see section on “Coding, Coverage, Reimbursement” in the topics “Compression Bandages”, “Tubular Dressings (Bandages)”, "Gradient Compression Stockings" and “Dynamic or Intermittent Compression”. For coding and coverage information for compression therapy for lymphedema, see topic "Expanding Care: Medicare's 2024 Coverage Update for Lymphedema Compression Treatment Items".
HCPCS Level II
- Overall, compression bandages, wraps and certain gradient compression stockings for management of VLUs are covered by Medicare Part B under the Surgical Dressing Benefit as long as used on patients with active VLU. Medicare will cover IPC for patients with refractory edema from chronic venous insufficiency with significant ulceration of the lower extremities who have received standard therapy but have failed to heal after 6 months of continuous treatment.[51][52]
- If a provider applies surgical dressings (note: Medicare considers compression bandages or wraps as surgical dressings) as part of a professional service that is billed to Medicare, these supplies are considered incident to the professional services of the healthcare practitioner and are not separately payable. Claims for the professional service, which includes the supplies, must be submitted to the local carrier or intermediary. If surgical dressings (including compression bandages or wraps) are sent home with the beneficiary, claims for these dressings may be submitted as durable medical equipment (DME). In this situation, use the place of service corresponding to the beneficiary's residence (POS=12); Place of Service Office (POS=11) must not be used.[53]
- Medicare coverage of compression devices for VLU is managed by Durable Medical Equipment Medicare Administrative Contractors (DME MAC). As it relates to compression therapy devices, DME MAC Jurisdictions (A,B,C and D) follow the same coverage determination and policy:
-
-
Local Coverage Determination (LCD) Surgical Dressings (L33831) [54]
-
Local Coverage Article: Surgical Dressings - Policy Article (A52491) [53]
- Local Coverage Article: Standard Documentation Requirements for All Claims Submitted to DME MACs (A55426) [55]
- LCD and Policy Article guidance is summarized in table 5 below:
Table 5. Medicare Coverage Guidelines for Compression Therapy Devices (refers to DME Supplies only, not procedural codes)
|
Type of compression device
|
HCPCS II code
|
Frequency of replacement
|
Coverage requirements
|
Not covered for
|
|
Bandages
|
Padding bandages, non-elastic
|
A6441
|
up to 1/week*
|
be part of multicomponent system to treat VLU **
|
strains, sprains, edema, or situations other than as a dressing for a wound
|
|
Conforming bandages, non-elastic
|
A6442-A6447
|
same as underlying dressing
|
hold dressings covering any wound or be part of multicomponent system to treat VLU **
|
|
Light compression bandages, elastic (i.e., ACE type)
|
A6448-A6450
|
up to 1/week*
|
hold dressings covering any wound
|
|
Moderate compression bandages, elastic
|
A6451
|
up to 1/week*
|
be part of multicomponent system to treat VLU**
|
|
High compression bandages, elastic
|
A6452
|
up to 1/week*
|
be part of multicomponent system to treat VLU**
|
|
Self-adherent bandages, elastic
|
A6453-A6455
|
up to 1/week*
|
hold dressings covering any wound or be part of multicomponent system to treat VLU**
|
|
Gradient Compression Wrap
Gradient Compression Stockings
|
Gradient compression wrap, non-elastic, used as a surgical dressing, each
|
A6545
|
1 per 6 months/leg
|
be used to treat VLU
|
- HCPCS A6531, A6532 and A6545: not covered for venous insufficiency without VLU, prevention of new VLU, prevention of recurrence of VLU that have healed, lymphedema in the absence of ulcers
- HCPCS A6552, A6554 and A6583: not covered for conditions other than lymphedema
|
Gradient compression wrap, with adjustable strap, below knee, 30–50 mmHg, each
| A6583
| 3 per each affected extremity or part of the body every 6 months
| lymphedema management
|
|
Gradient compression stockings 30-40, 40-50 mmHg, used as a surgical dressing, each
|
A6531, A6532
|
1 per 6 months/leg
|
be used to treat VLU
|
Gradient compression stocking, below knee, 30–40 mmHg, 40 mmHg or greater, each
| A6552, A6554
| 3 per each affected extremity or part of the body every 6 months
| lymphedema management
|
|
Gradient compression stockings other than above
|
A6530, A6533-A6544
A6549
|
n/a
|
non-covered under the surgical dressing benefit for any indications because they do not meet the statutory definition of a dressing; however, they may be considered for coverage under the lymphedema compression treatment items benefit and billed in accordance with CMS Final Rule CMS-1780-F
|
|
Other
|
Surgical stockings
|
A4490-A4510
|
n/a
|
not covered for any indication
|
|
Non-elastic binder
|
A4465
|
n/a
|
* unless part of a multicomponent system
** When multi-layer compression bandage systems are used for the treatment of a VLU, each component is billed using a specific HCPCS II code for the DME component. E.g., moderate or high compression bandages (A6451, A6452), conforming bandages (A6443, A6444), self-adherent bandages (A6454), padding bandages (A6441), zinc paste impregnated bandage (A6456).
CPT Codes
Typically, MACs will cover and separately reimburse the costs of the following procedures for non-lymphedema applications that meet Medicare coverage requirements, such as active VLU:
- 29581 - Application of multi-layer compression system, leg (below knee), including ankle and foot
CMS QUALITY MEASURES
Below are measures that are directly related to compression therapy for VLU. For other measures related to VLU see “Venous Ulcers” section ‘CMS Quality Measures’. For a comprehensive list of wound care related measures see “Wound Care Quality Measures”.
MIPS currently does not have VLU-specific measures. Listed below are VLU/compression therapy-specific measures issued by the qualified clinical data registry (QCDR) US Wound Registry.
|
QCDR
|
Title
|
Description
|
ID
|
Measure Type
|
|
US Wound Registry (USWR)
|
Adequate Compression at Each Visit for Patients with Venous Leg Ulcers (VLUs) Appropriate to Arterial Supply
|
Percentage of venous leg ulcer visits among patients aged 18 years and older in which adequate compression is performed at each treatment visit in the 12 month reporting period or until VLU outcome . Arterial status must first be assessed at least one time with any non-invasive method and the device chosen for compression must be appropriate based on whether arterial supply is normal or reduced
|
USWR32
|
Process
|
REVISION UPDATES
| Dates | Description |
| 1/01/24 | Updating 'Coding and Coverage' section |
| 6/19/19 | Expanded section 'Practice Tips', updated section 'Coding, Coverage and Reimbursement' |
| 10/24/19 | Updated section 'Practice Tips' |