CLINICAL
Overview
This topic provides a systematic approach to identifying patients at risk for developing pressure ulcers/injuries (PUs/PIs) and developing specific care plans, primarily based on the latest evidence-based clinical guidelines by the National Pressure Injury Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance (NPIAP/EPUAP/PPPI), Wound, Ostomy and Continence Nurses (WOCN) Society, the National Institute for Health and Care Excellence, and the Canadian Best Practice Guidelines for the Prevention and Management of Pressure Ulcers in People with Spinal Cord Injury, and the American College of Physicians. [5][6][7][8][9]
For a list of guidelines and quality measures related to PU/PI, see topic "
Pressure Ulcers/Injuries - Overview
". For an introduction and assessment of PU/PI including epidemiology, risk factors, etiology, pathophysiology, history, physical examination, diagnosis, differential diagnoses, documentation and ICD-10 coding, see "
Pressure Ulcers/Injuries - Introduction and Assessment
". For management of PU/PI, see topic "
Pressure Ulcers/Injuries - Treatment". For best practices in care coordination, see " Pressure Ulcers/Injuries -Coordination of Care".
Background
-
Definition: According to the NPIAP, pressure ulcers/injuries (PUs/PIs) are localized damage to the skin and/or underlying tissue, usually over a bony prominences or related to a medical or other devices, resulting from prolonged pressure or pressure in combination with shear.[5] The lesion can present below intact skin or as an open ulcer, which may be painful.[5] Synonyms for this condition include, bedsores, decubitus ulcers, pressure sores and many more.[5]
-
Relevance: PUs/PIs pose a large burden to affected individuals, caregivers and healthcare systems. As in any illness or injury, preventing PUs/PIs is better than treating them. From a patient's perspective, PUs/PIs can significantly impact quality of life of affected individuals and caregivers. From a healthcare system's perspective, PUs/PIs treatment is onerous, with estimated costs in the U.S. ranging between $9.1-11.6 billion a year. [1] In addition, PUs/PIs have been identified by the Centers for Medicare and Medicaid Services (CMS) as one of the 14 hospital-acquired conditions (HACs) that are reasonably preventable using evidence-based guidelines. [2] Along with the many recent CMS “value-based purchasing” initiatives, starting in 2008 CMS decided not to reimburse hospitals for hospital-acquired Stage 3 and 4 PU/PI and other preventable HACs. [10]
- Increasing clinicians' knowledge and attitude toward PU/PI prevention can improve their practice toward prevention of PU/PI. [11] Coordination of care is critical to decrease incidence and severity of PUs/PIs. See topic " Pressure Ulcers/Injuries - Coordination of Care"
Best Practices/ Recommendations for PU/PI Prevention
The 'Bundle' Concept
A care bundle can be defined as a group of best practices/recommendations derived from evidence-based clinical guidelines that if done in combination are likely to lead to better outcomes. [12] Bundles are meant to organize these best practices and recommendations and tie them in a systematic way that facilitates their implementation by clinicians, patients and caregivers in a practical manner. This topic outlines a PU/PI prevention bundle that incorporates the main components in PU/PI prevention [5][13]
:
-
Structured PU/PI risk assessment
-
Comprehensive skin assessment
-
Development/implementation of a personalized care plan that includes preventative interventions related to pressure redistribution, repositioning, mobility and activity, nutrition, management of moisture and shear, lifestyle/psychological interventions, measures to prevent medical device-related PU/PI, patient and caregiver education
Bundles are often customized according to care settings and facilities. Acronyms may help facilitate dissemination of care bundles for PU/PI within healthcare systems. Examples are illustrated in Table 1.
Table 1. Care bundles for PU/PI prevention
|
INJURY [14]
-
Inspect: Skin and structured risk assessment, support surface
-
Nutrition
-
Just Move: Mobility
-
Under and around devices: Medical Devices
-
Reposition
-
You are important: patient/caregiver education and engagement
SSKIN
[15]
-
Skin assessment
-
Surface
-
Keep moving
-
Incontinence
-
Nutrition
|
Best Practices/ Recommendations - In a Nutshell
Table 2 summarizes the best practices/ recommendations for PU/PI presented in this topic. For more details, see specific sections on each preventive intervention. Best practices/ recommendations shown in Table 2 apply to all care settings (e.g. acute care, long-term acute care hospitals, long-term care (skilled nursing facilities), home health, community, etc). However each care setting presents specific barriers and needs that require clinicians to adapt these general best practices/ recommendations. For instance:
-
Acute care: treatment goals in acute care settings may conflict with recommendations for PU/PI prevention. As an example, patients with respiratory issues may need to have head-of-bed elevated more than the 30 degrees angle recommended by clinical guidelines.
-
Long-term acute care hospitals: patient hand-off may result in gaps of information that preclude adequate fulfillment of a patient's care plan. A wound care team may not always be available or easily accessible. [16] It may be difficult for clinicians who receive the patient to identify all players accountable for wound care [e.g, physical therapy (PT), occupational therapy (OT), etc] from prior care settings.
-
Home health/community settings: each individual's daily life is permeated with an unique constellation of circumstances, some of which may turn out to be disruptive events that culminate in a PU/PI risk episode. These circumstances need to be factored in when developing/monitoring an individualized prevention plan. [17][18][19][20] To illustrate this point, please refer to case "How 20 minutes of fun can cost 4 months of disruption".
-
Outpatient wound clinics: commuting to/from the wound clinic for an office visit can be a major event for the patient/caregiver. If adequate transfer equipment/methods are not employed, the act of coming for an office visit itself can pose a PU/PI risk episode.
Given the above, for each preventative intervention described in this topic, authors strive to provide examples of how it has been successfully adapted in specific care settings. In addition, because PU/PI patients are often treated by distinct healthcare professionals across the continuum of care, care coordination is paramount for a successful prevention program. For more information, refer to the topic " Pressure Ulcers/Injuries - Coordination of Care". In addition, the editable " Provider-to-Provider Communication Form" can help ensure no information gaps are created upon transition of care.
Table 2. Summary of Best Practices/ Recommendations for Prevention of PU/PI [5][13]
Best Practices/ Recommendations
|
Description/ Comments
|
1. Structured risk assessment
|
- For all patients: Conduct a structured risk assessment using a validated risk assessment tool + identification of additional risk factors not included in validated tools
- Frequency: upon admission/discharge from a healthcare facility, upon a significant change in health condition, on a regularly scheduled basis based on the patient's acuity and care setting, prior to discharge from the care service
- Supplement use of a risk assessment tool with assessment of additional risk factors. [13] Examples of risk factors not captured by validated tools: presence or history of PU/PI, co-morbidities such as diabetes, peripheral arterial disease, neurological conditions affecting mobility/activity, smoking, psychosocial conditions (e.g. depression), care refusal
- See details in section 'Structured risk assessment across care settings': for acute care, long-term care, home health, community, Table 3 and Table 4 below.
|
|
2. Comprehensive skin assessment
|
- Conduct a comprehensive skin assessment whenever a risk assessment is conducted.
- Technique: Head-to-toe assessment with a focus on skin over bony prominences (e.g., sacrum, ischium, trochanters and heels) and on areas in contact with medical devices. See framework/checklist for skin assessment in Table 5.
- See details on 'Comprehensive skin assessment across different care settings': acute care, home health, community and Table 6.
|
|
3. Individualized care plan
|
- For individuals at risk for PU/PI, develop and implement an individualized risk-based prevention plan
|
| 3.1. Pressure redistribution
|
- For patients at risk for PU/PI, clinical guidelines recommend high-specification reactive foam or air pressure redistribution support surfaces (as opposed to a non-high specification reactive foam mattress)
- See details on 'Pressure redistribution support surfaces across care different settings': for acute care, home health, community
|
|
3.2 Re(positioning)
|
- All patients at risk for PU/PI should be repositioned, unless contra-indicated
- Frequency of repositioning is tailored to each individual and care setting. Generally, the following are starting points that can be adjusted:
- For seated individuals: shift weight every 15 - 30 minutes
- For individuals in bed: turn according to individualized tissue tolerance, which can be as often as every 1-4 hours, unless they can reposition themselves. Inspect areas at risk at every turn.
- For individuals in bed:
- 30° tilted side-lying position (alternate right side, back, left side) or the prone position as tolerated by the individual
- L i
mit head
-of-bed elevation to 30°
-
'Float the heels' off the bed
-
For seated individuals:
-
Provide adequate seat tilt to prevent the person from sliding off the chair
-
Ensure adequate feet support
- See details on '(Re)positioning across different care settings': for acute care, home health, community and Table 7.
|
|
3.3 Mobility and activity
|
- For individuals at risk for PU/PI, guidelines recommend early implementation of a mobility and/or activity program so that the patient can increase mobility and activity as rapidly as tolerated
- See details on ' Mobility and activity across care settings': for home health and community
|
|
3.4 Nutrition
|
- For all patients with PU/PI or at risk for PU/PI, clinical guidelines recommend screening of nutritional status upon admission to a healthcare setting, at each significant change in clinical condition and/or if progress towards healing of PU/PI is not observed.
- For individuals at risk for malnutrition, referral to a registered dietitian is recommended
- See details on 'Nutrition across care settings': for acute care, long-term facilities, home health and community
|
|
3.5 Management of moisture and shear
|
- For all patients at risk for PU/PI, clinical guideline recommends keeping the skin clean, dry and cool
- Limit layers under the patient to only one and keep it wrinkle free.
- Protect the skin from exposure to excessive moisture with moisture barrier products
- If possible, select support surfaces and support surface covers that allow control of skin temperature and moisture (microclimate control)
- Avoid skin contact with heated surfaces/devices/pads
- For individuals with urinary/fecal incontinence:
- Cleanse the skin promptly, apply moisture barrier products with emollients and skin protectants (e.g., made with zinc, silicone, dimethicone, cyanoacrylate) on perineal skin to protect skin from excessive moisture.
- For individuals at risk for PU/PI, clinical guidelines suggest use of prophylactic dressings (i.e. polyurethane/silicone 5 layer-foam dressings) to minimize skin shear on areas subject to higher pressure (e.g., bony prominences such as sacrum, heels) and prevent PU/PI.
- In operating rooms, if patients need to be in prone position during surgery, consider placing prophylactic dressings on areas subject to increased pressure (e.g. face, chin, and chest) to protect and minimize skin shear.
- For individuals with limited mobility, ensure transfers at the patient's environment are smooth and free of harmful pressure and shear
- See details on 'management of moisture and shear' across care settings: for home health and community
|
3.6 Lifestyle/psychosocial Interventions
|
- For individuals at risk for PU/PI, guidelines suggest clinicians confirm presence of healthy lifestyle choices and a supportive social network prior to discharging the individual from a facility.
- For any change in the patient’s routine, patients, caregivers, and clinicians should assess presence of increased risk for pressure injuries (see case " How 20 minutes of fun can turn into 4 months of disruption")
|
|
3.7 Preventative measures for medical device-related PU/PI
|
See Table 8
|
|
3.8 Patient and caregiver education
|
- Clinical guidelines recommend clinicians provide or facilitate access to PU/PI prevention education for the individual and caregivers upon discharge from a healthcare facility, on an ongoing basis, and every time health or lifestyle/psychosocial conditions change.
|
Structured Risk and Skin Assessment
Structured Risk Assessment
-
1C
For all patients, clinical guidelines recommend conducting a
structured PU/PI risk assessment upon patient's admission to a healthcare setting, on a regularly scheduled basis, and whenever there is a significant change to the individual's condition (Grade 1C). [9][13][21]
-
Rationale: For all patients, a structured risk assessment should be undertaken to identify those at risk at development of PU/PI. PUs/PIs impose a significant burden on individuals and healthcare systems, which can be largely avoided with implementation of individualized, adequate PU/PI care/prevention plans.[9][13][21] Frequency of regularly scheduled assessments vary according to the individual's acuity. Critically ill patients will need more frequent assessments than patients who can ambulate.
- As part of the structured risk assessment, clinicians may opt to adopt a validated risk assessment tool (e.g. Braden, Norton). However, clinical judgment is essential, as these tools do not capture all relevant risk factors (e.g., perfusion, skin status, etc). See risk factors and framework for history and physical examination focused on identifying risk factors in topic " Pressure Ulcers/Injuries - Introduction and Assessment"
-
Rationale: Currently there is no reliable evidence suggesting that the use of validated PU/PI risk assessment tools reduces the incidence of pressure ulcers, compared to clinical judgment alone. [22][23][24] However, due to the potential differences in clinical judgment due to gaps in healthcare professionals' knowledge of wound care and PU/PI [25]
, use of a validated tool can be helpful not only in clinical assessment but also in
documentation standardization and medical-legal purposes. To improve documentation and care coordination, clinicians at each institution should receive training and utilize the same validated risk assessment tool.
- Relying on the total risk assessment tool score alone when creating a prevention plan is not recommended. Risk assessment tool subscale scores and other risk factors should also be examined to guide risk-based planning. [13] Subscale scores provide information on specific deficits such as moisture, activity, and mobility, which should be addressed in their care plan. Even a score that indicates no risk does not guarantee that a person will not develop a PU/PI, especially as their condition changes.
Validated risk assessment tools
Validated PU/PI risk assessment scales for adults
Commonly used scales in the acute and post-acute settings include the Braden Scale, Waterlow Scale, the Norton Scale. [26] Intensive care units may consider the Cubbin & Jackson Index and the EVARUCI scale, which offers good diagnostic test accuracy in this setting. [27]
-
Braden Scale for Predicting Pressure Sore Risk: is the most commonly used in North America and has 6 subscales (sensory/perception, moisture, activity, mobility, nutrition, and friction/shear). [28]
- In the United States, the most used structured risk assessment tool for people over 8 years of age is the “ Braden Scale for Predicting Pressure Sore Risk
” tool.
[28]
[26]
A specific version for home care exists:
"Braden Scale for Predicting Pressure Sore Risk in Home Care".
- There is evidence that the Braden Scale has a moderate predictive validity. It is more suitable for mean age <60 years, hospitalized patients and the Caucasian population, and the cut-off value of 18 might be used for the risk assessment of PUs/PIs in clinical practice. [29]
- The Braden Scale has 6 categories, namely: Sensory perception, Moisture, Activity, Mobility, Nutrition, Friction/shear. To use the tool:
- Assess each of the 6 categories and select the description for each category that best describes the person's condition
- Assign a score for each of the 6 subscales from 1 to 4 according to descriptions on the tool (except for friction/shear, which is scored from 1 to 3)
- Calculate the total score, which will be between 6 and 23 points. The lower the score, the greater the risk for skin breakdown. Patients scoring 18 or less are considered to be at risk.
-
At risk: 15 – 18
- Moderate risk: 13 – 14
- High risk: 10 – 12
- Very high risk: 9 or less
-
As noted above, it is important that all subscale scores and additional risk factors be considered when developing a prevention/care plan. To illustrate this point, consider the 2 patients below [12]:
-
Case 1
: a patient has an overall Braden Scale of 19 (not at-risk for PU/PI), but in analyzing the subscales, the patient is chairfast (subscale score of 2), and has very limited mobility (subscale score of 2). These subscale scores are important indicators of risk and need to be addressed in the prevention plan.
-
Case 2: a patient with Braden Scale of 19 has a history of healed PU/PI or uncontrolled diabetes. These are important risk factors for recurrence and need to be addressed.
-
Waterlow Scale
: most frequently used scale in the U.K.
[30]
[31]
, has 9 subscales: (BMI, continence, skin type, mobility, appetite, tissue malnutrition, neurological deficit, major surgery/trauma, and medications).
[30]
The higher the score, the higher the risk of developing PU/PI.
-
The Norton Scale
was developed in England in 1962 and was the first PU/PI risk evaluation scale to be created. [32]
-
The Norton Scale has 5 subscales (physical condition, mental condition, activity, mobility, and incontinence). To use the tool:
-
Assess each of the 5 subscales and assign a score for each subscale:
- Physical condition: Good (4), Fair (3), Poor (2), Very bad (1)
-
Mental condition: Alert (4), Apathetic (3), Confused (2), Stupor (1)
- Activity: Ambulant (4), Walk with help (3), Chair bound (2), Bed bound (1)
- Mobility: Full (4), Slightly impaired (3), Very impaired (2), Immobile (1)
- Incontinence: Not (4), Occasionally (3), Usually/Urine (2), Doubly (1)
- Calculate the total score, which will be between 5 and 20 points. The lower the score, the greater the risk for skin breakdown. Patients scoring 14 or less are considered to be higher risk.
- Low risk: greater than 18
- Medium risk: 14-18
- High risk: 10-14
- Very high risk: 10 or less
-
Table 3 provides comments, tips and clinical examples to facilitate assessment of PU/PI risk factors and scoring when utilizing PU/PI risk assessment scales.
Table 3. Assessment of risk factors for PU/PI and clinical examples
|
Risk Factor
|
Comments/ Tips
|
Clinical Examples
|
Sensation
|
- Assess for comorbidities that can affect sensory perception:
- Does the patient have neuropathy (e.g. due to diabetes mellitus), spinal cord injury, or dementia?
- A monofilament test may be used to check for sensation
|
- Completely impaired:
- A patient who does not respond to pain or does not feel pain over most of the body
- Very impaired:
- A patient who can only show that he/she is feeling pain by moaning or being restlessness
- A patient with paraplegia with loss of sensation to the lower half of the body
- Slightly affected:
- A patient who can respond to verbal commands, but often has difficulty in showing he/she is in pain
- A resident with diabetes with some neuropathy in the feet, who cannot feel pain or discomfort in one or more of their extremities
- Not affected:
- A patient who is able to feel and communicate when in pain
|
|
Moisture
|
Assess for sources of moisture:
-
Urinary or fecal incontinence
- Moisture near the peristomal region in individuals with a tracheostomy
- Accumulated sweat in body creases/folds, particularly in hot weather
- Accidental urinal spills during bed use (common in men)
- Highly exudative wound
- Malfunctioning ostomy pouch
-
Fistula output leakage
-
Excessive sweat (diaphoresis)
|
- Excessively moist
- Diaphoretic patient who is constantly sweating
- Linen is always damp
- Often moist
- Patient with urinary incontinence who is often but not always moist.
- Linen must be changed at least once a shift.
- Sometimes moist:
- Patient with limited mobility who cannot always get to the bathroom on time (i.e. functional incontinence)
- Needs an additional daily change of linens
- Rarely moist:
|
|
Activity level
|
Assess for degree of physical activity:
- How much can the patient move independently?
- Is there a wound on their foot preventing ambulation?
- Is the patient at risk of fall and need help ambulating?
- Does the patient have any respiratory conditions resulting in shortness of breath?
- Assess the patient’s overall activity and not just during a shift (e.g. activity level is often lower at night)
- Patients who are chairfast or bedfast are almost always at risk for skin breakdown.
|
- Confined to bed:
- Patients who cannot move due to conditions such as with spinal cord injury, severe stroke, or with any condition requiring prolonged bed rest.
- Confined to chair:
- Ability to walk is severely limited or nonexistent. Cannot bear own weight and/or must be assisted into a chair or wheelchair. Examples include patients who cannot bear weight on their foot due to surgery, wounds, stroke, etc.
- Somewhat ambulatory
- Occasionally takes brief walks during the day, sometimes with help, but predominantly remains seated or in bed throughout the shift.
- Patients who primarily rely on a wheelchair for mobility.
- Regularly ambulatory:
- Walks outside their room at least twice a day and moves around inside their room at least once every two hours while awake.
- Typically applicable to patients who do not require a wheelchair, maintain a high level of independence, and have a low risk of falling.
|
Ability to change body position (repositioning)
|
Assess for ability to change position of body and/or extremities independently
- If confined to chair, can the patient perform weight shifts every 15 minutes?
|
-
Totally immobile:
-
Requires assistance to alter any body or limb position.
- Minimally mobile:
- Can make only minor, infrequent positional adjustments and needs help for more substantial or regular movements.
- Moderately mobile:
- Capable of making regular, small positional changes.
- Fully mobile:
- Can frequently and substantially adjust their position independently.
|
Nutrition
|
Assess nutritional status:
- Has the dietitian evaluated the patient?
- Is the patient being offered protein?
- If poor appetite/food intake, determine the cause:
- Does the patient dislike the food being offered?
- Does the patient have any condition that prevents them from chewing/swallowing?
- Does the patient have new/worn out dentures causing pain?
- Is the patient approaching the end of life?
- Is there any underlying condition affecting appetite?
- If the patient is on tube feeding, is it resulting in gastro-intestinal discomfort/diarrhea?
|
For patients with dietary restrictions, which may include fasting (NPO), diet limited to clear liquids or intravenous fluids, or total parenteral nutrition (TPN):
- Severely Compromised:
- The patient is not permitted oral intake (NPO).
- The patient has been on clear liquids or intravenous fluids for more than five days.
- Likely Insufficient Nutrition:
- The patient is on tube feedings or a liquid diet but is not receiving the ideal amount (e.g. sporadically refusing liquid diet or tube feedings)
- Sufficient Nutrition:
- The patient is on a regimen of tube feedings or TPN that likely fulfills most nutritional requirements.
For patients who are consuming solid foods:
- Severely Compromised Nutrition:
- Incomplete meals are the norm, with typically less than a third of offered food consumed.
- Protein consumption is low, at two servings or fewer from meat or dairy each day.
- Fluid intake is insufficient, and liquid dietary supplements are not consumed.
- Likely Insufficient Nutrition:
- The patient often does not finish a meal, often eating only half of the food provided.
- Patient consumes only three daily servings of protein from meat or dairy.
- Dietary supplements are taken but not regularly.
- Sufficient Nutrition:
- The patient consumes the majority of each meal.
- Protein is consumed adequately, with four daily servings from meat and dairy.
- Meal refusal happens on occasion, yet supplements are taken when presented.
- Excellent:
- The patient consistently eats entire meals.
- Protein intake is excellent, with at least four servings of meat and dairy each day.
- Snacks are taken between meals
- No need for dietary supplements
|
|
Mechanical forces (friction shear)
|
Assess for friction of skin against chair, bed:
- Does the patient require assistance in moving or repositioning?
- Does the patient have conditions that may lead to friction (e.g. spasticity, contractures or agitation)?
- If patient needs a prosthesis to walk, is it causing friction or shear on the skin in contact with the prosthesis?
|
- High exposure to mechanical forces:
- The patient is unable to be lifted without sliding against sheets.
- Regularly slides down when in bed or seated, necessitating frequent and substantial help to reposition.
- Spastic movements, muscle tightness, or restlessness cause nearly continuous skin friction.
- Moderate exposure to mechanical forces:
- Skin contact with sheets or devices like restraints or prosthetics occurs to an extent during movement.
- Patient generally maintains position in a chair or bed, though occasionally slides down.
- Low exposure to mechanical forces:
- The patient is capable of moving independently in bed and while seated, with enough muscle strength to lift themselves without sliding.
- Consistently maintains a good position whether in bed or seated.
|
Validated tools for children
Those include:
-
Braden Q Scale is a validated, adjusted version for children under 8 years of age.
[33]
-
Braden QD scale: revised, simplified version is the "Braden QD Scale", for immobility-related and device-related pressure injuries in the pediatric acute care environment. [4]
structured risk assessment across different care settings:
The general recommendations/best practices described above apply to all care settings. Table 4 highlights how those have been adapted to some specific care settings:
Table 4. Structured Risk Assessment Across Different Care Settings
|
Care Setting
|
Frequency of structured risk assessment
|
Common risk factors not captured by validated risk assessment tools
|
|
Acute care
|
The ideal frequency of s
tructured risk assessment varies
according to the specific acute care setting and patient's acuity
[12]
:
-
Acute care settings, in general: perform upon admission and then at least daily (refer to each organization's policies) or with a significant change in condition, upon discharge,
-
Critical care: perform in every shift, as patients' status may change quickly
-
Operating room: perform upon admission, at discharge to the recovery room, and every 4 hours for longer operations (include time in the holding and recovery room when assessing time)
|
- Stays in operating room, emergency room
- Prolonged immobilization
- Need for/use of transport
- Use of medical devices
- Hemodynamic instability precluding turning
- Use of vasopressors
- Multi-system organ failure
- History of loss of consciousness pre and during hospital stay
|
|
Long-term care
|
In skilled nursing facilities, 80 percent of PU/PIs develop within two weeks of admission and 96 percent develop within three weeks of admission.
[34]
As for frequency of assessment, Medicare recommends completion of a risk assessment upon admission, weekly for the first four weeks after admission, then monthly or whenever there is a change in the resident’s condition (e.g., upper respiratory infection, pneumonia, or exacerbation of underlying congestive heart failure).
[34]
|
- End-of-life/ palliative care
|
Home health
|
For all home health patients, it is recommended that home health clinicians complete a risk assessment upon first evaluation, weekly or with each Outcome and Assessment Information Set completion, when the patient's condition changes, and upon discontinuation of home health services.
[35]
|
- In addition, risk assessment in the home health setting should include assessment of [35]:
- Patients' economic and insured status to determine implementation options
- Caregiving resources and caregivers' ability to manage PU/PI prevention
- Ability to obtain needed prevention materials and supplies from community resources and health care vendors
|
Community
|
For individuals at risk for PU/PI, it is important that clinicians identify potential psychosocial risk factors before discharging from a healthcare setting or during outpatient clinic visits. [7]
[20]
[17]
|
- Even after rehabilitation and education sessions, individuals with limited mobility (e.g. with spinal cord injury) face several obstacles upon returning to their communities where unpredictable life events may lead to a new PU/PI. Those events can range from seemingly trivial events (e.g., wheelchair cushion or mattresses breaking down, wearing ill-fitting hand-me-down shoes, vital equipment not being available in a timely manner, change in environment during travel/sports activities) to disruptive events (e.g., extremely poor caregiving, untreated illness). [20]
[17] S ocioeconomically disadvantaged individuals with spinal cord injury face even higher risks in their daily lives, and more complex lifestyle/psychological interventions (usually offered by OTs) should be considered.
|
Comprehensive Skin Assessment
-
For all individuals being admitted to a care setting, clinical guideline and expert consensus recommend conducting a
comprehensive skin assessment whenever a PU/PI risk assessment is conducted (Grade 1C).
[13]
[12]
- A nurse or healthcare professional trained to complete the skin assessment should perform a comprehensive, head-to-toe skin assessment, ensuring special attention is given to the skin overlying bony prominences (e.g., sacrum, ischium, trochanters, heels, etc) and areas in contact with medical devices. [13][12] Table 5 below provides a sample checklist that may be adapted to each healthcare facility.
Table 5. Checklist for comprehensive head-to-toe skin assessment by healthcare professionals
|
Comprehensive head-to-toe skin assessment
Ensure all skin is checked, including under medical devices, catheters, tubing, compression stockings. Focus on bony prominences and areas in contact with medical devices
Inspection of the skin:
-
Skin color: ensure adequate light for visual skin inspection (the best lighting includes ambient or natural sources, or penlight may be helpful). Compare symmetrical body parts and look for:
-
Differences in color between symmetrical body parts (e.g. paleness, flushing, cyanosis)
-
Redness (erythema) or darker skin tone: may indicate infection or increased pressure. If erythema is found, depress erythema with finger or transparent disc to determine if it is blanchable (turns white) or non-blanchable (stays the same color).
-
Blanchable erythema signals normal reactive hyperemia. Blanchable erythema, along with changes in sensation, temperature or firmness, may precede visual changes due to PU/PI [13] and represent an opportunity to implement offloading and pressure redistribution strategies before further skin damage occurs.
-
Non-blanchable erythema indicates a Stage 1 PU/PI.
-
Assessing if erythema is blanchable or non-blanchable :
-
Finger method: apply pressure for three seconds and assess blanching following removal of the finger.
-
Transparent disc method: apply pressure with a transparent disk equally over an area of erythema. Assess blanching underneath the disk during its application.
-
Of note, darkly pigmented skin does not have a visible blanche response. Other skin findings that signal PU/PI should be prioritized (e.g. localized heat, pain, edema and induration).
[13]
[36]
-
Skin integrity:
-
Assess findings: is skin injured? Are there cracks, openings, excoriations?
-
If integrity is compromised: investigate cause and differential diagnoses (e.g. skin tear, PU/PI, moisture-associated skin damage, eczema)
Palpation of the skin:
-
Skin temperature:
-
Touch the skin with the back of your hands and compare symmetrical body parts to detect differences in temperature:
-
Warmer skin may indicate infection or inflammation
-
Colder skin may indicate areas with poor blood flow (ischemia)
-
If available, an infrared thermometer or imaging device can be used to help assess skin temperature, after proper training is provided.
[13]
-
Skin turgor: abnormal turgor may indicate aged skin, dehydration, connective tissue disease. Pinch the skin near the clavicle or forearm so that the skin lifts up from the underlying structure, then let go. If skin quickly returns to place, skin turgor is normal. If the skin does not return to place (tenting), skin turgor is abnormal.
-
Edema: is it pitting or non-pitting edema?
-
Pain: is it present and how strong is the pain?
-
Moisture: excessive moisture is a risk factor for PU/PI. Touch the skin to feel if the skin is wet or dry or if it has the right balance of moisture. Also, assess if it is dry, oily, clammy.
Assessment of darkly pigmented skin
[13][36]:
- For a reliable visual assessment of skin tone, the skin should be clean and free of skin products.
- A skin color chart (e.g. Munsell color chart or Fitzpatrick Classification Scale) may be used for objective measurement of skin tone (Figure 1).
- Tangential light and slightly moistening the skin may aid in the detection of early pressure injury in darker skinned individuals.
-
Carefully inspect any discoloration over pressure areas.
-
Areas of discoloration in relation to surrounding skin should be assessed more closely for temperature changes, edema, changes in tissue consistency and pain.
-
If resources and training are available, an infrared thermometer/imaging device and a sub-epidermal moisture/edema measurement device can be used to help detect PUs/PIs.
|
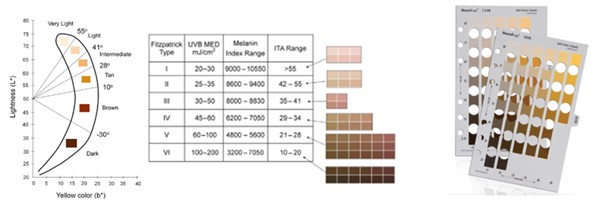
Figure 1. Tools for objective assessment of skin tone. Fitzpatrick Classification Scale (left) and
Munsell color chart (right). By Tânia Santos, RN, MSc
Skin ASSESSMENT across DIFFERENT CARE SETTINGS:
The general recommendations/best practices described above apply to all care settings. Table 6 highlights how these general recommendations/best practices are adapted to some specific care settings:
Table 6. Skin Assessment Across Different Care Settings
|
Care setting
|
Frequency of skin assessment
|
Comments
|
|
Acute care
|
In regards to frequency, skin assessment should be performed whenever a structured risk assessment is completed. (See section ' Structured Risk Assessment' above). Frequency of assessments should be increased on units where patients are critically ill and/or less mobile (critical care unit, operating room).
|
-
Coordination: staff communication upon shift changes is key, nurse assistants should be empowered to recognize/ report skin abnormalities
-
Documentation: In addition to the medical record, a log can be kept at each unit to determine which patients have had a comprehensive skin assessment, which have PU/PI, and the highest stage of the deepest ulcer. [12] This log will also be critical in assessing the unit's incidence and prevalence rates.
|
|
Home Health
|
- For all home health care patients: conduct a comprehensive skin assessment of the patient upon admission [13][35]
- For patients identified as being at risk for PU/PI: conduct skin assessment at each home visit, teach patient and caregivers to perform skin inspections and to detect signs of altered skin integrity, and monitor patient and caregiver report of patient skin integrity at each home visit [35]
|
As healthcare professionals are not at the bedside 24 hours a day, patients' and caregivers' education and engagement is paramount.
|
|
Community
|
- Clinical guideline recommends community patients at high risk for PU/PI (e.g. with spinal cord injuries) perform visual and tactile skin inspections daily, when trying new equipment, when health or lifestyle conditions change, when problems are identified [7]
|
-
Visual inspection includes:
search for redness, discoloration, and bruising; changes in texture, such as rashes, dryness, and swelling; and abnormalities such as cracks, scabs, and blisters.
-
Tactile inspection includes
: assessment of skin temperature, moisture, and induration, or bogginess.
- Individuals who cannot perform visual/tactile inspection themselves (e.g. due to quadriplegia), should have a caregiver check their skin
|
Customized Care Plan - Preventative Interventions
-
For all individuals at risk for PU/PI, we recommend clinicians develop and implement an individualized risk-based prevention plan.
[13]
[12]
- Most patients do not fit into a "routine" care plan, and need a personalized prevention plan that addresses the needs identified through a structured risk assessment. [12] A proper prevention plan includes interventions that aim at stabilizing, reducing or removing underlying risk factors.
- To facilitate implementation of customized care plans, facilities might opt to have preset order sets that can be customized for each individual, based on structured risk and skin assessments. To expedite implementation of preventive measures, many healthcare facilities allow nurses to place order sets for PU/PI prevention, without the need to wait for a prescribing provider to sign them off.
- Computerized decision support systems have been shown to reduce incidence of PU/PI in long-term care facilities for older people. In a study, the system chose residents' skin care products, absorbent briefs and mattresses based on resident's assessment and PU/PI risk. [37]
[38]
- A sample care plan with examples of interventions that may be considered for each specific Braden subscale scores is listed on the AHRQ.gov website. [39]Nurses and certified nurse assistants should tailor these interventions to meet the needs of each patient.
Pressure redistribution
Pressure redistribution with support surfaces is one of the key interventions for PU/PI prevention. Support surfaces redistribute pressure by either increasing the body surface in contact with the support surface and thereby reducing interface pressure, or by mechanically altering the parts of the body that bear load, thereby reducing the duration of the applied pressure on any given anatomical site. [5][40][41]
See definition and types of support surfaces in section '
Pressure Redistribution' in "Pressure Ulcers/Injuries - Treatment"
-
Mattress and bed support surfaces:
1B
To prevent PUs/PIs among individuals at risk for PU/PI, clinical guidelines recommend use of a high-specification reactive foam mattress as opposed to a non-high specification reactive foam mattress. (Grade 1B) [5][6][8][9]
-
Rationale: there is moderate certainty evidence supporting use of high specification foam mattress to prevent PU/PI among individuals at risk of developing PU/PI. [42] When used in the operating room, these support surfaces are also associated with a reduction of postoperative PU/PI. Clinical guidelines recommend usage of high specification foam mattresses compared with any other type of mattress at home or at healthcare facilities, to prevent PU/PI in people at risk of PU/PI.[5][6][8][9] There is no evidence justifying superiority of one higher specification foam mattress over any other higher specification foam mattress.
-
Coverage: Medicare covers high specification foam mattresses (Group 1 support surface) for beneficiaries who are completely immobile or are partially immobile and meet at least one of the following: A. impaired nutritional status, B. Fecal or urinary incontinence, C. Altered sensory perception, D.Compromised circulatory status. [43]
-
Selection: To help identify the appropriate support surface (i.e., overlay, mattress, integrated bed system) for adults (≥16 years of age) and bariatric patients in care settings where the length of stay is 24 hours or more, clinicians can use decision support tools such as the 'Algorithm for Selection of Hospital Bed and Pressure Redistribution Support Surface' in topic "Policy and Procedure: Pressure Injury Assessment, Treatment, and Prevention" and the WOCN Society's Evidence-and Consensus-Based Support Surface Algorithm. [44][45]
- For each individual, it is good practice to consider the following factors when selecting or changing the mattress, overlay or integrated bed support surface [5]:
- Overall risk of pressure injuries
- Response of the skin and tissues
- Independence, mobility and activity needs
- Posture and sleeping position and their effects on pressure redistribution
- Need for microclimate management and shear reduction features, and
- Preferences and care goals
-
Seating support surfaces: For individuals at risk for PU/PI using wheelchairs or who sit for prolonged periods, clinicians might opt for a high-specification foam pressure redistributing cushion. [8]
-
Rationale: Adequate pressure redistribution support surfaces and repositioning are crucial for prevention of PU/PI as it is estimated that more than half of PU/PI occurring among individuals in community settings happen as a result of pressure while sitting. [7][46]
-
Coverage: Medicare covers adjustable skin protection seat cushions (HCPCS E2622, E2623) for patients with a wheelchair and current or past history of PU/PI, or with absent or impaired sensation in the area of contact with the seating surface, or inability to carry out a functional weight shift. [47]
pressure redistribution ACROSS DIFFERENT CARE SETTINGS:
The general recommendations/best practices described above apply to all care settings. Below we highlight how these general recommendations/best practices are adapted to some specific care settings:
Acute care
- For patients at risk for PU/PI who cannot turn themselves or cannot be turned, consider a reactive support surface (overlay or mattress). [13]
- For all individuals with or at risk of PU/PI who are undergoing surgery, use a pressure redistribution support surface on the operating table. [13]
Home health and community
-
For home health patients at risk for PU/PI: it is important that home health clinicians assist the patient in obtaining a high-specification foam pressure redistribution mattress/chair surface. Clinicians can help patients and caregivers procure support surfaces by identifying most adequate model/brand and suppliers.
[15]
-
For home health patients and community individuals at risk for PU/PI:
-
Mattresses and bed support surface:
- These support surfaces need to be professionally reassessed at least every 4 years or sooner if the person’s medical condition changes. [7] Some clinicians may recommend reassessment of the support surface every 2 years.
-
Seating support surfaces:
-
For people with mobility issues (e.g. spinal cord injury): it is recommended that specialized seating professionals (OT/PT) assist with initial fit assessment and recommendation of wheelchairs and other sitting support surfaces including toilet, shower bench, seating for recreational activities . [7]
[17]
-
Individuals at risk for PU/PI should sit on their prescribed seating system: If sitting on another surface is needed (e.g., on a padded toilet seat), weight shifts/repositioning should be done more frequently than every 15 minutes.
[17]
-
Maintenance: many new and recurrent PUs/PIs occur due to worn equipment that has not been replaced. Clinical guideline recommends teaching the individual and caregiver to care and maintain the seating support surface according to manufacturer's instructions, to frequently monitor signs of wear, to set up cushion correctly and monitor bottoming out, to replace cushion as soon as signs of wear and tear are identified, and to avoid placing additional layers on top of the cushion. Scheduled reassessments should be done at least every 2 years or sooner if medical, living conditions change or if equipment wears. [7]
(Re)Positioning
Repositioning (i.e, changing the patient's position on a bed or seating surface) allows for relief of pressure on an existing PU/PI and on areas where PU/PI can develop.
Frequency of repositioning is tailored to each individual.
For patients who can reposition themselves, reminders (e.g., alarm clocks, apps) to prompt them to reposition can be helpful. Patients who cannot reposition themselves need assistance from trained healthcare professionals and caregivers. Repositioning/turning systems have been developed to help clinicians reposition patients more easily. Clinicians should avoid positioning patients on their ulcers and bony prominences.
See details on repositioning frequency and techniques in section '
(Re)Positioning' in topic "Pressure Ulcers/Injuries - Treatment"
.
In summary, for patients at risk for PU/PI, guidelines recommend
[13][21][48]
:
-
All patients at risk for PU/PI should be repositioned, unless contra-indicated.
-
For patients who cannot be repositioned due to medical reasons, PU/PI prevention plans should rely on alternative prevention strategies (e.g., pressure redistribution support surfaces)
-
Frequency of repositioning is tailored to each individual and care setting, taking into consideration the patient's general medical condition, overall treatment objectives, comfort and pain. Generally, the following are starting points that can be adjusted:
-
For seated individuals: at least every 1 hour while sitting, with weight shifts every 15-30 minutes
-
For individuals in bed: turn according to individualized tissue tolerance, which can be as often as every 1-4 hours, unless they can reposition themselves. Inspect areas at risk at every turn.
-
Repositioning techniques to prevent PU/PI in individuals at risk for PU/PI [13]:
-
Repositioning in bed:
-
Use the 30° tilted side-lying position (alternate right side, back, left side) or the prone position if the individual can tolerate this and her/his medical condition allows. Avoid extended use of prone positioning unless required for management of the individual’s medical condition.
-
Head-of-bed elevation: keep the head of bed as flat as possible. Limit head-of-bed elevation to 30° and avoid prolonged elevation unless medical conditions require otherwise
-
Heels:
'float the heels' off the bed, that is, ensure heels are free of the surface of the bed. For long term use (e.g, for patients with spinal cord injury) use heel suspension devices and ensure heels are not touching the surface of the bed. To redistribute pressure, it is important that the weight of the leg is redistributed along the entire length of the calf without placing pressure on a single, small area of the leg (e.g., Achilles tendon). See " Heel Protectors".
- Upon each turn/rotation, inspect skin subject to increased pressure for any signs of impending PU/PI (e.g., erythema, pain)
-
Repositioning seated individuals:
- Goal is to maintain comfort and minimize pressure/shear on areas in contact with seating surface.
- Provide adequate seat tilt to prevent sliding forward in the wheelchair or chair.
- Select a reclined seated position with the individual’s legs elevated. If reclining is not appropriate or possible, feet should be properly supported on the floor, on a footstool or on footrests.
- Check hamstring length. If individual cannot extend legs completely, use of elevating leg rests is not recommended, as individual would be pulled into a sacral sitting posture, causing increased pressure on the coccyx and/or sacrum.
- Teach and encourage individuals who spend prolonged durations in a seated position to perform pressure relieving maneuvers.
-
Positioning devices or pillows can be helpful in maintaining positions. To offload the occiput, clinicians might opt for fluidized positioning devices. [49]
-
Technology-guided repositioning: clinical guidelines suggest the use of continuous bedside pressure mapping as a visual cue to guide repositioning. [13]
REPOSITIONING ACROSS DIFFERENT CARE SETTINGS
The general recommendations/best practices described above apply to all care settings. Table 7 highlights how these general recommendations/best practices are adapted to some specific care settings:
Table 7. Repositioning Across Different Care Settings
|
Care setting
|
Frequency of repositioning
|
Repositioning techniques
|
|
Acute care
|
For all patients at risk for PU/PI:
- As it relates to frequency, typically clinicians are instructed to reposition all patients every 2 hours
|
- For patients who need to have the head of the bed elevated more than 30 degrees due to medical reasons
(e.g. feeding tubes, respiratory issues):
- PU/PI prevention plans should rely on alternative prevention strategies (e.g., pressure redistribution support surfaces) [13][12]
- Clinicians may try to shift the patient's body weight by placing several pillows under the patient’s shoulder and back. [12]
- Micro-shifts/offloading every 30-60 minutes are recommended. [14]
- For patients who do not want to reposition, address underlying cause and document on medical records. Clinicians may want to adopt the tips below [12]:
- For uncontrolled pain (e.g. following joint replacement surgery or abdominal surgery): address pain
- Explain why repositioning is important in preventing PU/PI
- Identify favorite position and if it is not possible (due to surgery, injury), try to find an alternative that the patient will like.
-
Use of technology:
turn and position systems can facilitate patient repositioning and lateral transfer by reducing the force/strain required from healthcare professionals when turning/transferring patients (e.g. Völkner® Turning System, AirTap Patient Repositioning System, Tortoise™ Positioning System). Monito ring systems with sensors attached to the patient may help clinicians understand which patients need to be repositioned by staff and which patients are able to reposition themselves (see Patient Monitoring
, e.g. Leaf Patient Monitoring System). New technologies that have been recently introduced to the market include sensors that monitor pressure interfaces and prompt clinicians to turn patients when needed (
VŪ
, an Advanced Pressure Visualization System).
|
|
Home health
|
Frequency for all patients at risk for PU/PI
[35]:
- Teach patient and caregivers to reposition patient every 2 hours while in bed and at least every 1 hour while sitting, with weight shifts every 15-30 min
- Assess resources and caregiver potential to maintain prescribed repositioning/turning schedule. Consider repositioning prompts such as an alarm or mobile apps. [15]
- Establish a nighttime turning schedule that optimizes patient repositioning and caregiver rest
|
Techniques for all patients at risk for PU/PI
[35]:
- Teach patient and caregivers to use pillows, towels, blankets, comforters, and foam/foam wedges to properly position patient and suspend heels off the bed.
- Teach patient and caregivers to pad tubing and medical devices.
- Assist the patient in obtaining positioning devices/supplies.
|
|
Community
|
Frequency for seated individuals :
- For patients with mobility impairments but with sufficient upper extremity strength and function, manual weight shifts every 15 minutes are one of the commonly taught repositioning strategies.
|
Techniques for seated individuals :
- For patients with mobility impairments but with sufficient upper extremity strength and function: Weight shifts include push-ups, leaning forward to elevate ischial tuberosities off sitting surface, side lean pressure relief. [17]
- For those who cannot perform manual weight shifts power wheelchair features, such as tilt and recline may be used. [7]
[17] Wheelchairs with power weight-shifting technology help reduce the effects of sitting pressure on bony prominences of the buttocks.
- Periodic re-education: postural management, positioning, and pressure-redistributing movements are central to PU/PI prevention. Initial good habits can deteriorate over time; periodic re-education is beneficial. [7]
|
Mobility, Activity
Limited mobility is one of the most important risk factors for PU/PI development and delayed ulcer healing. [50]
-
For individuals at risk for PU/PI, guidelines recommend early implementation of a mobility and/or activity program so that the patient can increase mobility and activity as rapidly as tolerated.
[13]
- Depending on the level of immobility, PT/OT should be included if possible. Therapists will evaluate patients' range of motion and individual needs, and develop a plan for sitting and ambulation as rapidly as patients can tolerate. [13]
[26]
mobility/activity care ACROSS DIFFERENT CARE SETTINGS
The general recommendations/best practices described above apply to all care settings. Below we highlight how these general recommendations/best practices are adapted to some specific care settings:
Home health
For all patients at risk for PU/PI
[35]:
- Collaborate with patient and caregivers to establish, monitor and encourage patients to engage in a program for improving patient activity/mobility.
- Offer PT referral to review plan and improve activity level and/or mobility
Community
For individuals with mobility impairment (e.g. spinal cord injury)
[7]
-
Mobility assessment and training sessions conducted by PT/OT are recommended:
- A comprehensive assessment of mobility includes: evaluation of physical impairments, gross motor skills, and movement quality, and additional risk for PU/PI. This assessment should be repeated every time gross motor skills decline or if a PU/PI develops
- Gross motor skills training includes: bed mobility, transfers, wheelchair mobility, and ambulation as appropriate
-
Exercises for PU/PI prevention: a PT/OT can guide in the development of a regular exercise program to optimize muscle strength and endurance, encourage postural alignment, improve cardiovascular endurance, and prevent fatigue and deconditioning.
- Periodic re-education: postural management, positioning, and pressure-redistributing movements are central to PU/PI prevention. Initial good habits can deteriorate over time; periodic re-education is beneficial. [7]
Nutrition
Nutritional optimization is critical in healing and prevention of PUs/PIs.
-
For all patients with PU/PI or at risk for PU/PI, clinical guidelines recommend screening of nutritional status upon admission to a healthcare setting, at each significant change in clinical condition and/or if progress towards healing of PU/PI is not observed. [13]
[7]
[6]
- Screening of nutritional status may be performed by any healthcare team member upon admission to a healthcare facility or at first visit in community settings. Its goal is to identify individuals at risk for malnutrition so that they can undergo a comprehensive nutrition assessment by a registered dietitian. [13]
-
Validated tools such as the "
Nestlé MNA" and "Self-MNA®" can be used to facilitate initial screening and follow up.
-
Medicare Quality Payment Program, Quality Measure:
- "Process Measure: Nutritional Screening and Intervention Plan in Patients with Chronic Wounds and Ulcers"
- "Patient Reported Nutritional Assessment and Intervention Plan in Patients with Wounds and Ulcers"
- "Preventative Care and Screening: Body Mass Index (BMI) Screening and Follow-Up"
-
For individuals at risk for malnutrition, referral to a registered dietitian is recommended. Care plan should be individualized to each person. See nutritional optimization plan for individuals at risk for PU/PI and malnutrition in section ' Nutrition' in topic "Pressure Ulcers/Injuries - Treatment".
nutrition ACROSS DIFFERENT CARE SETTINGS
The general recommendations/best practices described above apply to all care settings. Below we highlight how these general recommendations/best practices have been adapted to some specific care settings:
Acute care, long-term care facilities:
- Dehydration is a common problem predisposing patients to PU/PI. Care plans may suggest offering a sip of a beverage each time a clinician enters the room. [12]
Health care and community
For individuals at risk for PU/PI
[35]:
- Assess nutritional risk using a validated screening tool. If patient is at risk for malnutrition, consult dietitian/nutritionist (a phone/ home visit may be a viable option).
- Teach/monitor patient and caregivers regarding daily dietary needs and fluid intake.
- Secure provider order for nutrition supplements/support as needed and assist patient in obtaining supplements. Of note, oral nutrition supplements are not typically covered by Medicare.
Management of moisture and shear
Excessive moisture is a risk factor for development of PU/PI and for infection of existing PU/PI. [26]
Moisture and shear can lead to the superficial breakdown of fragile skin of older individuals, contributing to the development of PU/PI.
Excess moisture in the sacral area may occur due to sweat (i.e. non-breathable support surfaces), but most frequently is a result of fecal or urinary incontinen
ce.
[26]
Microclimate management:
-
For all patients at risk for PU/PI, clinical guideline recommends keeping the skin clean and appropriately hydrated.
[13]
-
Rationale: Changes in the skin microclimate (temperature, humidity and airflow next to the skin surface) can alter tissue deformation response upon pressure and indirectly increase risk for PU/PI development. [51]
- Manage/address excessive skin moisture [13]:
- Limit layers under the patient to only one and keep it wrinkle free. More layers can alter properties of the support surface, increase interface pressure and/or cause skin to sweat. Check with manufacturers for individual recommendations.
- Protect the skin from exposure to excessive moisture with moisture barrier products in order to reduce the risk of pressure damage. Current evidence suggests that creams with fatty acid (e.g. Mepentol, not available in the U.S.) versus a control compound (a cream that does not include fatty acid) may reduce the incidence of PU/PI. [52]
- If possible, select support surfaces and support surface covers that allow control of skin temperature and moisture (microclimate control).
- Avoid skin contact with heated surfaces (e.g. heating pads, bed warmers, hot water bottles, heated car seats). Heat increases the skin metabolic rate, induces sweating and decreases the tolerance of the tissue for pressure. [13]
- Avoiding use of alkaline soaps and cleansers. [13]
For individuals with fecal and urinary incontinence:
- Cleanse the skin promptly [13], apply moisture barrier products with emollients and skin protectants (e.g., made with zinc, silicone, dimethicone, cyanoacrylate) on perineal skin to protect skin from excessive moisture. Use high absorbency incontinence products to protect the skin. Fecal/urine containment devices/garments may be used. See management of fecal and urinary incontinence in section ' Excessive moisture and shear' in topic "Pressure Ulcers/Injuries - Treatment".
Prophylactic dressings:
-
2C
For individuals at risk for PU/PI, clinical guidelines suggest use of prophylactic dressings to minimize skin shear on areas subject to higher pressure (e.g., bony prominences such as sacrum, heels) and prevent PU/PI (Grade 2C) [13]
[6]
-
Rationale: Current evidence (level C, low certainty) indicates that compared with no dressing, prophylactic silicone/polyurethane 5-layer foam dressings (e.g., Mepilex Border, Allevyn Life), may reduce PU/PI incidence among patients at risk for PU/PI when used with other preventative measures. Other types of dressings have not been shown to reduce PU/PI incidence. [52] Use of prophylactic polyurethane 5 layer foam dressings has been shown to be cost-effective in preventing PU/PI in Australian acute care settings, but this result may not be applicable to other settings/countries. [53]
-
Coverage: for Medicare beneficiaries in acute care, home health, long-term care facilities, cost of prophylactic dressings are included in the reimbursement for episode of care. For patients at home (outpatient) without home health services, prophylactic dressings are not a covered benefit. [54]
- When selecting prophylactic dressings, clinicians might opt to consider the following factors [13]:
- Ability of the dressing to manage microclimate
- Ease of application and removal
- Ability to regularly assess the skin: design should facilitate regular skin assessment (e.g. soft silicone borders that are easy to lift and place back)
- Anatomical location where the dressing will be applied
- The correct dressing size
- It is important to follow manufacturers' recommendations. A prophylactic dressing should be replaced if it becomes damaged, displaced, loosened or excessively moist.
Transfers and transitions to various surfaces:
- For individuals with limited mobility, ensure transfers at the patient's environment are smooth and free of harmful pressure and shear. [26][17]
- Consider using textiles with low friction coefficients. [13]
Moisture and shear management ACROSS DIFFERENT CARE SETTINGS
The general recommendations/best practices described above apply to all care settings. Below we highlight how these general recommendations/best practices have been adapted to some specific care settings:
Acute care setting
- In operating rooms, if patients need to be in prone position during surgery, consider placing prophylactic dressings on areas subject to increased pressure (e.g. face, chin, and chest) to protect and minimize skin shear.
Home health and community settings:
To manage moisture excess among patients at risk for PU/PI:
-
Skin care
[13]
[35]:
- Educate patients and caregivers on the importance to keep skin clean and dry, and how to cleanse the skin using plain warm water and mild, non-deodorant, non-scented soap.
- Teach how to apply a moisture barrier to protect skin from moisture, assist patients and caregivers with purchase of skin care products.
- Encourage use of absorbent underpads and adult diapers to keep moisture away from skin.
To minimize skin and tissue shear among patients at risk for PU/PI:
-
Transfers:
- Teach patient and caregivers the use of draw sheets and other transfer techniques.
- Assist patient to obtain a transfer device.
-
A PT/OT can help select and train individuals in transfer techniques from/to different surfaces to ensure safe repositioning and minimize skin shear during transfer. Path/objects between transfer surfaces should also be assessed for barriers impeding safe transfer.
[7]
[35]
Lifestyle/psychosocial Interventions
-
For individuals at risk for PU/PI, guidelines suggest clinicians confirm presence of healthy lifestyle choices and a supportive social network prior to discharging the individual from a facility. [13]
[7]
- Daily life after discharge from a healthcare facility may pose additional risk factors for development of a new/recurrent PU/PI. Major depression can lead to recurrence of PU/PI, as it has been associated with inactivity, self-neglect and poor adherence to care plan. [17] For any change in the patient’s routine, patients, caregivers, and clinicians should assess presence of increased risk for pressure injuries (see case " How 20 minutes of fun can turn into 4 months of disruption"). If potential lifestyle/psychological factors that increase risk of PU/PI are identified, clinicians should consider referring the individual to appropriate resources for problem resolution including PT, OT, rehabilitation services, peer counseling and support groups, formal psychotherapy/counseling. [7]
[20]
Preventative Measures for Medical Device-related PU/PI
- The NPIAP clinical guideline recommend clinicians consider patients with medical devices to be at risk for development of PU/PI. [13]
- The pressure and shear caused by medical devices can result in the development or aggravation of an existing PU/PI. Thus, it is important that clinicians follow manufacturer's safety recommendations, choose devices with proper fit and size, and ensure devices are properly secured to prevent dislodgment. [13]
- Medical-device related PI should be staged using the International NPIAP/EPUAP Pressure Ulcer Classification System, unless the injury is on mucosa. [13] See topic " Pressure Ulcers/Injuries - Classification/Staging"
- Retrospective analysis of a large group of patients showed that [55]:
- Medical device-related PU/PI forms faster than non-medical device related PU/PI, thus timely proactive assessment and prevention interventions are critical
- Most medical device-related PU/PI occur on the ears (e.g, oxygen tubing secured over the ears), and feet
- By stage, most medical device-related PU/PI are superficial (58% were Stage 1 or 2)
- The most common devices linked with medical device-related PU/PI were oxygen tubing and masks, and casts/splints
- The NPIAP has created posters based on the best practices below to prevent medical device-related PU/PI [13]:
-
Choose the correct size of medical device(s) to fit the individual
- ✔ Cushion and protect the skin with prophylactic dressings in high risk areas (e.g., nasal bridge)
- ✔ Remove or move removable devices to assess skin at least daily
- ✔ Avoid placement of device(s) over sites of prior, or existing pressure injury
- ✔ Educate staff on correct application, use and securement of devices and prevention of skin breakdown
- ✔ Be aware of edema under device(s) and potential for skin breakdown
- ✔ Confirm that devices are not placed directly under an individual who is bedridden or immobile
- Table 8 below illustrates examples of medical devices, and specific best practices to prevent PU/PI. [56]
Table 8. Prevention of Medical Device-related Pressure Injuries
|
Medical device
|
Areas subject to pressure
|
Best practices to prevent pressure injury
|
Oxygen tubing and masks
|
Ear, nose, face
|
- When using oxygen tubing that are secured over the ears, consider padding ears or tubbing in contact with ear with foam or gel pads to prevent skin breakdown.
- If appropriate and safe, alternate the oxygen delivery device between correctly fitting mask and nasal prongs to reduce the severity of nasal and facial pressure injuries
|
Endotracheal tube
|
Lips, tongue |
Reposition tube every 2 hours, careful not to dislodge tube
|
| Cervical collar |
Chin, shoulder, ear
|
- Minimize length of use of collars if possible. Risk of skin breakdown increases by 66% for every 1-day increase of collar time [57]
- Use padded collars (e.g., Aspen, Miami) instead of rigid collars and order an extra set of pads to allow one pad to completely dry after cleansing neck
- Inspect skin under the collar at every skin assessment. If erythema is detected, check collar for proper fit
|
Tracheostomy tube
|
Peristomal skin
|
- Risk for PI is higher when tracheostomy tube is still sutured, as it is difficult to insert tracheostomy dressing as a cushion to protect skin. After removal of sutures, preferably within 7 days of the tracheostomy procedure, foam dressing may be inserted under the faceplate to help relieve pressure [58]
- Consider placing a rolled towel under ventilator tubing near the connection to the tracheostomy tube so that the tubing does not deflect downward, causing tension and thus deflecting the faceplate downward
- Keep head in a neutral position [58]
|
Bilevel positive airway pressure (BIPAP) and continuous positive airway pressure (CPAP) masks
|
Facial areas in contact with mask
|
- Ensure mask is not too tight
- Consider alternating masks (partial face and full face)
- Consider use of prophylactic dressings to decrease pressure. There is some evidence that hydrocolloid dressings on the forehead and nasal bridge may prevent PU/PI over the nasal bridge [59]
[60]
|
| Rigid Transfer Boards |
Bony prominences on the back, occiput, heels |
- Ensure appropriate transfer and repositioning systems are employed
|
|
Negative Pressure Wound Therapy
|
Areas in contact with tubing |
If suction tubing may cause excessive pressure on underlying skin, create a bridge to conduct suction to another location which will not cause excessive pressure (e.g. if PU/PI on the hip, create bridge to the abdomen). See topic " How to Select and Apply Negative Pressure Wound Therapy Devices" |
| Splint and casts |
Areas in contact with splint/cast |
Borders of splints/casts should be padded. Remove splint or cast for skin assessment if possible. Notify orthopedics if erythema is seen under the borders of the splint/cast |
| Compression stockings/ TED hoses/ wraps |
Areas in contact with device |
Remove devices once a day for skin assessment. Pay special attention to borders, inspect for areas of circular constriction |
| Foley catheters |
Areas in contact with tubing |
Ensure securement devices are in place to keep the port from sitting in between the patient's leg |
PATIENT EDUCATION (for clinicians)
Patient education
- Clinical guidelines recommend clinicians provide or facilitate access to PU/PI prevention education for the individual and caregivers upon discharge from a healthcare facility, on an ongoing basis, and every time health or lifestyle/psychosocial conditions change. [13]
[7]
- Topics for education should be individualized and at minimum include [7]:
- Potential causes and risks of pressure ulcer development
- Methods of self-monitoring
- Reduction of pressure ulcer risks
- A personalized prevention plan, developed with the patient's input and agreement, needs to be explained and understood by the patient and caregiver. The plan includes interventions for positioning in bed and chair, support surfaces, activity, nutrition, skin care, lifestyle changes
Resources:
- Patient education brochures
- Digital content (websites, web-apps):
- Mobile App: VA Pressure Ulcer Resource (VA PUR) App, designed to help Veterans and their Caregivers learn about preventing and taking care of existing pressure ulcers/injuries. Includes tools such as reminders to move, location of nearby facilities, etc.
APPENDIX
Summary of Evidence (SOE)
SOE - Pressure Redistribution
( back to text)
Clinical Guidelines
[13]
[6]
[8]
[9]
| Intervention |
NPIAP |
American College of Physicians
|
NICE |
WOCN |
High specification reactive foam mattress to prevent PU/PI among individuals at risk
|
Weak B1 |
|
positive recommendation, no level of evidence
|
Class IB |
Advanced static mattresses and overlays to prevent PU/PI among individuals at risk
|
|
Strong recommendation, moderate evidence |
|
|
Systematic reviews/ meta-analyses
- A 2015 systematic review and meta-analysis included 59 trials and compared different types of pressure redistribution support surfaces in prevention of PU/PI. Authors found that foam alternatives to standard hospital foam mattresses reduce the incidence of pressure ulcers in people at risk (RR 0.40 95% CI 0.21 to 0.74). The relative merits of alternating‐ and constant low‐pressure devices were unclear. Pressure‐relieving overlays on the operating table reduce postoperative pressure ulcer incidence, although two trials indicated that foam overlays caused adverse skin changes. Meta‐analysis of three trials suggested that Australian standard medical sheepskins prevent pressure ulcers (RR 0.56 95% CI 0.32 to 0.97). Authors concluded that for people at high risk of developing pressure ulcers, higher‐specification foam mattresses rather than standard hospital foam mattresses should be used, where possible. Also, whenever possible, healthcare facilities should consider the use of selected pressure relief devices for high risk patients in the operating theatre, as this is associated with a reduction in postoperative incidence of pressure ulcers. Medical grade sheepskins are associated with a decrease in pressure ulcer development. [42]
SOE - Prophylactic Dressings
( back to text)
Systematic reviews/ meta-analyses
- A 2018 systematic review and meta-analysis included 6 trials (n = 1247) that compared a silicone dressing with no dressing. Authors concluded that silicone dressings may reduce pressure ulcer incidence (any stage) (RR 0.25, 95% CI 0.16 to 0.41; low-certainty evidence; downgraded for very serious risk of bias). In the one trial (n=77) rated as being at low risk of bias however, there was no clear difference in pressure ulcer incidence between silicone dressing and placebo-treated groups (RR 1.95, 95% CI 0.18 to 20.61; low-certainty evidence, downgraded for very serious imprecision).
[52]
- A 2016 systematic review included 25 studies, and the meta-analysis revealed a statistically significant effect of a silicone foam dressing strategy in reducing hospital acquired PU/PI incidence (effect size = 4.62; 95% CI: 0.05-0.29; p < .00001, effect size = 4.50; 95% CI: 0.05-0.31; p = .00001, respectively) in critically ill patients. Evidence of the effectiveness of nutrition, skin-care regimen, positioning and repositioning schedule, support surfaces, and the role of education in prevention of PU/PI development in the ICU was limited, which precludes strong conclusions. [61]