ABSTRACT
Incontinence‐associated dermatitis (IAD) is an irritant contact dermatitis from prolonged contact with urine or feces, which can significantly impact patient comfort and quality of life. [1][2][3] IAD is one of the four clinical types of moisture-associated skin damage (MASD) and is considered preventable. [4] IAD is a common and significant condition in individuals with incontinence, negatively impacting their health and quality of life. IAD causes discomfort, skin damage, psychological stress and increases the risk of infection. [1]
History: All patients with urinary and/or fecal incontinence should undergo regular skin assessments for signs of IAD - at least once daily, and more often if incontinence episodes are frequent. [4][5] Initial patient assessment should include a comprehensive clinical history and physical examination, with visual inspection of the perineal area to rule out other pathologies (e.g., allergies, atrophic vaginitis). Assessment should also cover mobility, dexterity, and cognitive function, along with urinalysis, a frequency–volume chart, and bowel diary, a post-void residual urine test and a review of the patient’s medication history. [6] Clinicians might opt to utilize risk assessment scales as tools (e.g. Perineal Assessment Tool) for the early recognition of risks and complications related to IAD. [7]
Physical Examination: IAD typically occurs in the perianal and buttocks, thighs, external genitalia, and supra-pubic regions. These lesions are superficial, diffuse, with irregular borders, and there is no presence of dry necrosis; however, slough may be observed. This damage is characterized by hyperemia, edema, burning, itching, pain, and abrasions, and may be complicated by opportunistic infections.[2][3]
Diagnosis of IAD: The diagnosis of IAD is based on the clinical and visual assessment of the skin in the entire diaper/brief area and adjacent regions, including the suprapubic region, abdominal folds, inguinal region, and gluteal folds, followed by classification. [5][8]
Differential diagnoses : It may be challenging to correctly differentiate IAD from other conditions, including pressure ulcers/injuries (PUs/PIs), contact dermatitis (e.g., from textiles or skin products), infectious lesions (e.g., herpes simplex), or moisture-related skin damage such as intertrigo. [5] See topic "Pressure Ulcers/Injuries - Is it Really a Stage 2?"
Classification systems for IAD: Clinicians might opt to utilize the Ghent Global IAD Categorization Tool (GLOBIAD) for assessing and classifying IAD into categories. Although not routinely used in nursing practice, several IAD assessment tools are all reliable, valid, and suitable for use in clinical practice (see Appendix, ' IAD Assessment Instruments')
Ulcer prognosis (healability) assessment: IAD is generally healable with early intervention and appropriate care, more severe cases or those with complicating factors may require more intensive and prolonged treatment.
Documentation: Assessment and documentation of continence status should also include deviations from normal bladder and/or bowel function and any follow-up actions. See ' IAD Documentation Checklist'
Treatment, Prevention: See "Incontinence Associated Dermatitis - Prevention and Management in Adults and Older Adults" and "Incontinence Associated Dermatitis - Prevention and Management in Infants"
When to refer to specialists:
- Nurse specialized in continence for assessment and recommendations on how to manage incontinence.
- Wound care specialist if IAD does not show signs of improvement after 3-5 days of a structured skin care regimen and continence management or if skin condition deteriorates
- Infectious disease specialist if bacterial infection (e.g., spreading erythema, increasing exudate, odor) or fungal infection (e.g. satellite lesions, etc) is suspected
- Nutritionist if malnutrition.
- Social work for economic and social support.
- Psychologist/ mental health professional for depression and other psychological issues.
- Primary care team or specialist if other complex comorbidities (e.g., diabetes, immunosuppression, severe diarrhea)
ICD-10 Coding: See ' 'ICD-10 Coding'
INTRODUCTION
Overview
This topic provides an introduction and framework for assessment of incontinence associated dermatitis (IAD), including epidemiology, risk factors, etiology, pathophysiology, history, physical examination, diagnosis, differential diagnoses, documentation and ICD-10 coding. For management of pressure ulcers/injuries see "Incontinence Associated Dermatitis - Prevention and Management in Adults and Older Adults" and "Incontinence Associated Dermatitis - Prevention and Management in Newborns and Infants". For differential diagnoses, see topic "Pressure Ulcers/Injuries - Is it Really a Stage 2?
Background
Definition
-
Incontinence‐associated dermatitis (IAD) is an irritant contact dermatitis from prolonged contact with urine or feces, which can significantly impact patient comfort and quality of life. [1][2][3]
-
- IAD is one of the four clinical types of moisture-associated skin damage (MASD) and is considered preventable.[4]
-
- Moisture-associated skin damage occurs as a result of long-term exposure to a source of moisture, such as urine, stool, sweat, wound drainage, saliva, or mucus.[4] The four types of MASD are:
-
- Incontinence-associated dermatitis: caused by urine or feces
- Intertriginous dermatitis: occurs in skin folds, such as the groin, armpits, and toes
- Periwound moisture-associated dermatitis
- Peristomal moisture-associated dermatitis
- IAD typically occurs in the perianal and buttocks, thighs, external genitalia, and supra-pubic regions. These lesions are superficial, diffuse, with irregular borders, and there is no presence of dry necrosis; however, slough may be observed. This damage is characterized by hyperemia, edema, burning, itching, pain, and abrasions, and may be complicated by opportunistic infections.[2][3]
- IAD may be also known by other terms described in Table 1.
Table 1: Terms that have been used for IAD
| Other terms that have been used for incontinence-associated dermatitis |
- Diaper/ brief / napkin / nappy dermatitis
- Diaper / brief/ napkin / nappy rash
- Irritant dermatitis
- Moisture lesions
- Perineal dermatitis
- Perineal rash
|
Relevance
- IAD is a common and significant condition in individuals with incontinence, negatively impacting their health and quality of life. IAD causes discomfort, skin damage, psychological stress and increases the risk of infection.[1]
-
- Patients with IAD experience discomfort, pain, itching, and tingling, which negatively impacts their daily lives, independence, and overall quality of life.
- The psychological consequences of IAD for adults managing incontinence can be significant. Individuals may experience shame, embarrassment, and social isolation due to odor, leakage, and the need for frequent hygiene measures.
- Skin affected by incontinence also place patients at a higher risk for pressure ulcers/injuries (PU/PI). [1] PU/PI and secondary infection cause longer lengths of stay and higher costs of care. [1]
- Proactive prevention and management, including proper skin care and protective barriers, are vital for improved patient outcomes. Emphasizing preventative strategies is essential to reduce the burden of IAD and ensure better care for affected individuals.[5]
Epidemiology
Reported prevalence and incidence rates of IAD vary widely.
Incidence
- IAD incidence rates range from 3.4% to 30% depending on the care setting. [3][4][9]
Prevalence
- IAD prevalence ranges from 5.6% to 56.2% depending on care settings. [3][4][9]
- In acute care settings [10]:
- In a large U.S. study, 46.6% of patients evaluated (n=5342) were incontinent of urine, stool, or both.
- The overall prevalence rate of IAD among all patients was 21.3%.
- The prevalence of IAD among patients with incontinence was 45.7%.
- The prevalence of pressure injury in the sacral area among individuals with incontinence was 17.1%.
- The presence of IAD and immobility was associated with a significantly increased likelihood of developing a sacral pressure injury.
- Higher prevalence is observed at the extremes of age: in newborns, children, and the elderly. However, individuals of any age can be affected if their skin is in a vulnerable state and in constant contact with moisture.[11]
-
-
Pediatric population: IAD affects around 16% of children. It is estimated that 7% to 35% of the pediatric population will experience this condition at some point during childhood, with higher prevalence among children aged 9 to 12 months. Only 7% of families with affected children seek medical treatment.[12][13]
Risk Factors
Risk factors for the development of IAD include increased stool frequency, urinary and/or fecal incontinence, limited mobility, friction/shear problems, deteriorating skin conditions (e.g., due to aging, steroid use, or diabetes), decreased cognitive awareness, an inability to perform personal hygiene, pain, elevated body temperature (pyrexia), medication use (e.g., antibiotics, immunosuppressants) and critical illness. [1][3][14][15][16]
Details on risk factors and protective factors for IAD are listed below and in Table 2 .
Risk factors increasing the likelihood of IAD include [17][18] :
- Fecal incontinence: 5.79 times more likely
- Stool characteristics indicative of increased risk: 5.28 times more likely
- Increased stool frequency: 5.76 times more likely
- Fever: 4.23 times more likely
- Hypoproteinemia: 3.30 times more susceptible
- Impaired consciousness: 2.43 times more likely
- Each day of antibiotic use: 4.13 times more likely
- Diabetes mellitus: 2.90 times more likely
- Higher overall Perineal Assessment Tool (PAT) score: 2.56 times greater likelihood
Protective factors that reduce the likelihood of IAD include [17]:
- Higher serum albumin level: likelihood reduced by a factor of 0.88
- Higher Braden Scale score: likelihood reduced by a factor of 0.66
Table 2. Incontinence-Associated Dermatitis (IAD) Risk by Setting and Type of Incontinence Among Adults
| Incontinence-Associated Dermatitis (IAD) Risk by Setting and Type of Incontinence Among Adults |
|
Individuals with incontinence are at significantly higher risk for developing incontinence-associated dermatitis (IAD).
- Nursing Home Residents [9]:
-
- Urinary and/or fecal incontinence affects approximately 59.8% of residents
-
- Urinary incontinence: Prevalence ranges from 30% to 65.6%.
- Fecal incontinence: Affects 22.4% to 55.5% of residents.
- Community-Dwelling Adults [2]:
-
- Urinary incontinence:
-
- Women: affects 19% of women aged 45 or younger. Increases to 29% in women aged 80 or older.
- Men: in men, rates range from 5% to 15%.
- Fecal incontinence:
-
- Affects an estimated 8.9% of women and 7.7% of men.
|
For the pediatric population:
- In addition to the risk factors described above, the occurrence of IAD is associated with increased intestinal motility, such as in infants receiving phototherapy, experiencing withdrawal symptoms, ingesting protein-rich diets, or undergoing infections or treatments with antibiotics or immunosuppressive agents, among other factors.[19]
Etiology
IAD results from prolonged skin exposure to urine, feces, or both. While incontinence is a necessary condition, not all incontinent individuals develop IAD - highlighting the role of additional contributing factors and individual susceptibility. [18]
Pathophysiology
The occurrence of IAD is significantly associated with tissue tolerance to injury, a weakened epidermal barrier, and a reduced ability for skin regeneration and repair, as well as changes in the perineal region’s microclimate and altered urinary and fecal control.[20] These factors are closely related to the variation in skin condition according to the patient’s age group.[20]
-
Tissue tolerance to injury: factors affecting tissue tolerance include age, overall health status, nutrition, oxygenation, blood perfusion, exposure to friction or shear, and core body temperature. [21]
-
Perineal microclimate: the perineal microclimate is influenced by [21]:
-
- The frequency and type of eliminations (urinary, fecal, or both),
- Skin condition (erythematous and/or edematous), and
- Factors that impair perineal skin (hydration, urine and fecal pH, pathogens present in feces or on the skin, increased skin permeability, and mechanical friction)
Adults
Characteristics of the skin
- The skin, the body’s largest organ, has multiple functions, including protection from external trauma, UV light, bacteria, and toxins; thermoregulation; sensation; excretion; and non-verbal communication. [22] For an overview on the skin and its function, refer to the topic "The Skin".
- Acid mantle as a barrier: the skin’s surface normally maintains an acidic environment (pH 4–6), which is essential for preserving the integrity of the barrier known as the acid mantle. This acidic pH not only regulates the skin microbiome by controlling resident bacteria, but also promotes optimal cohesion of the stratum corneum, thereby supporting barrier strength and function.[5]
- Biomechanical barrier: the stratum corneum, the outermost layer of the epidermis, serves as the skin’s biomechanical barrier to prevent microorganism invasion. It is composed of 70% protein, 15% lipids, and 15% water, with lipids and water being essential components of the skin barrier function.[23]
-
- The stratum corneum is continuously renewed and consists of 15 to 20 layers of flattened cells known as corneocytes (Figure 1).
-
- Corneocytes maintain approximately 15% water content, which helps preserve skin hydration and supports a flexible, effective barrier.[11][24]
- Corneocytes are embedded in a lipid matrix that forms a semi-permeable barrier and comprises the natural moisturizing factor.[11][24]
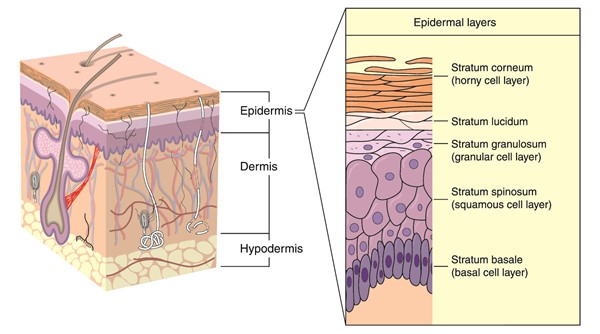
Figure 1. Layers of the epidermis
Older Adults (Geriatric Population)
Age-Related Skin Changes Increasing the Risk of IAD
- Elderly skin, which is drier, thinner, and less elastic, becomes more prone to damage, especially when combined with incontinence (Figure 2). To reduce this risk, increased personal hygiene and skin care are essential. [25]
-
- Skin changes:
-
-
Reduced skin moisture : in elderly skin, the stratum corneum consists of 70% proteins, 15% lipids, and 10% water, indicating a loss of moisture compared to adult skin. Lipids and water are crucial for maintaining the skin's barrier function and elasticity. [23]
-
- Throughout life, the "natural moisturizing factor" (NMF) changes due to a reduction in intercellular lipids with age, leading to a lower number of corneocytes and a a thinner lipid matrix that surrounds the corneocytes (Figure 3).[11][24]
-
Structural fragility: aging skin is characterized by reduced collagen and elastin replenishment, flattening of the dermoepidermal junction, thinning of the dermis, and loss of subcutaneous fat - causing stretching and a wrinkled appearance. [26]
-
- The fragility of the dermoepidermal junction increases the likelihood of friction injuries during skin cleansing.
- A thinner dermis results in decreased blood vessels, nerve endings, and collagen, leading to diminished sensation, temperature regulation, elasticity, and moisture retention. [25]
-
Glandular changes: glandular changes include reduced sweat gland activity, sebaceous gland hyperplasia with decreased sebum production, increased skin surface pH, greater transepidermal water loss, and reduced skin moisture.[26] Dryness due to lower sebum production results in cracks, itching, and prolonged healing time. [25]
- Urinary changes:
-
- Incomplete bladder emptying is another common alteration in the elderly due to reduced bladder elasticity. In women, weakened pelvic floor muscles further exacerbate the problem. These physiological changes in skin and bladder function, coupled with comorbidities and limited mobility, heighten the risk of incontinence and skin damage. [2]
|
Figure 2. Aging Skin
|
Figure 3. Stratum corneum structure, with corneocytes surrounded by intercellular lipid layers
|
Moisture exposure-related skin changes increasing the risk of IAD
Moisture exposure - particularly prolonged or repeated - significantly increases the risk of skin damage and IAD in adults, with older adults being especially vulnerable due to age-related changes in skin structure and physiology.
-
Moisture exposure and skin barrier breakdown: excess moisture causes overhydration of keratinocytes and lipid layer disruption, resulting in corneocyte swelling and increased stratum corneum thickness.[11] These changes reduce barrier function and increase permeability to irritants such as urine, feces, and microorganisms like Candida albicans and Staphylococcus aureus. [2] [11][27][28] The consequences include [11][27][28]:
-
- Accelerated transepidermal water loss (TEWL)
- Reduced skin elasticity and resilience
- Increased microbial colonization
- Greater susceptibility to friction injuries and mechanical damage
- Effects of urine and feces on the skin:
-
-
Feces: contain enzymes (i.e. proteases and lipases) that break down proteins and lipids in the stratum corneum, increasing the risk of IAD. Liquid stool is particularly damaging, especially in hospitalized or immobile patients.[21][11]
-
Urine: contains urea, which is converted into ammonia by urease-producing bacteria. Ammonia raises skin pH, leading to lipid barrier damage, increased TEWL, and higher susceptibility to irritants and microorganisms. [11]
-
Combined exposure: urine and feces together have a synergistically harmful effect, intensifying skin irritation, maceration, and inflammation. [3]
- Patients with incontinence experience alterations in the perineal microclimate (Figure 4), predisposing the skin to damage caused by pressure, friction from the diaper/brief, and shear forces during the cleaning process. Frequent washing with soaps that disrupt the skin’s natural pH, prolonged diaper/brief use, and the layering of bed covers or skin protectants can impair the diaper/brief’s ability to absorb moisture. [29]
-
Maceration and acid mantle disruption: skin maceration occurs with prolonged moisture exposure, resulting in soft, whitish, swollen skin with weakened structural integrity. This environment damages the intercellular lipid layers within the stratum corneum, and fosters increased pH, loss of barrier function, and increased friction injury risk. However, the exact duration of exposure needed to cause maceration has not been clearly established. [27][28] The inflammatory response triggered by the invasion of irritants and microorganisms (e.g., Candida albicans ) leaves the skin vulnerable to skin breakdown.[30]
-
- Disruption of the acid mantle compromises the skin’s defenses, leading to erythema, pain, and increased susceptibility to breakdown from friction, shear, and prolonged exposure to urine or feces (Figure 5). Elevated pH accelerates barrier damage by activating enzymes that degrade protective lipids and impair repair processes, which are essential for maintaining the integrity of the skin barrier and repairing damage caused by prolonged exposure to urine or feces. [11][31]
|
Figure 4. Elderly Patient Wearing a Diaper/Brief
|
Figure 5. Skin with erythema in the perineal and gluteal region.
|
Newborns
Skin Characteristics in Newborns and Their Susceptibility to IAD
-
Skin development by gestational age: the development of the skin is closely linked to gestational age. As pregnancy progresses, both the thickness and number of epidermal layers increase. Structural changes, such as an increasingly wavy dermoepidermal junction, also occur. By approximately 34 weeks of gestation, a well-developed epidermis is typically present, though complete maturation of the stratum corneum varies between 30 and 37 weeks.[32] Characteristics include:
-
- Full-term newborns (born between 37–41 weeks of gestation): skin is thin, fragile, and sensitive.
- Preterm newborns (born before 37 weeks of gestation): skin is even thinner, often transparent, with visible superficial veins and reduced resistance to mechanical stress (Figure 6).[33] Preterm skin exhibits functional immaturity and barrier deficits [33][34] :
-
- Weaker dermoepidermal cohesion, with fewer anchoring fibers
- Reduced collagen and elastin content
- Immature skin appendages
- Underdeveloped hypodermis
- Increased transepidermal water loss and i ncreased permeability, reducing its ability to protect against irritants and microbes
- Higher risk of percutaneous absorption, colonization, and infection
- Impaired thermoregulation
- Greater susceptibility to trauma

Figure 6: Newborn with IAD in the genital region showing signs of infection. Source: Nurse Simone Vidal
-
Barrier function of the skin: the stratum corneum is composed of corneocytes, which regulate water loss through the skin. This layer also contains lipids, mainly free fatty acids, cholesterol, and ceramides, which combine with water to form an endogenous emollient. Lipids and proteins protect the stratum corneum by forming an impermeable barrier that regulates natural water loss and provides an acidic, xeric environment that prevents microbial invasion. [11][34]
-
- The physiological regulation of the skin depends on the skin's pH, which can be compromised in an alkaline environment.
-
- At birth, newborn skin is neutral in pH
- Within days, it acidifies to pH<5.5, forming the acid mantle, which strengthens barrier integrity
- In preterm infants, this acidification may take several weeks, delaying acid mantle formation and increasing susceptibility to microbial invasion, topical agent absorption, and injury. [35][36]
- Interestingly, despite their skin immaturity, preterm newborns may experience fewer perineal skin lesions compared to full-term infants. This is attributed to[36]:
-
- Lower intestinal transit, resulting in reduced fecal exposure
- Fewer baths and less frequent use of cleansers that alter skin pH and increase permeability
Moisture exposure-related skin changes increasing the risk of IAD in Newborns:
- Newborn skin is structurally and functionally immature, making it particularly susceptible to environmental and behavioral stressors after birth. Factors that may affect skin integrity include fluctuations in ambient temperature, inconsistent hydration, and prolonged contact with astringent substances or surfaces, such as diapers/briefs.[37]
-
-
In the first two weeks of life of full-term infants, the epidermal barrier function is still incomplete, resulting in increased skin permeability. This immaturity makes the skin more vulnerable to mechanical damage, especially in areas exposed to moisture and friction, such as the diaper/brief region. Over time, the skin gradually develops greater impermeability and resilience.[38]
-
In preterm infants, the stratum corneum is notably thinner and less effective than in full-term infants or adults. This increases the risk of infection and systemic toxicity due to enhanced percutaneous absorption of substances, placing preterm neonates at greater risk for IAD.[39]
-
Diapers: in neonates, IAD commonly arises from diaper occlusion, which prolongs skin contact with urine and feces. Urine contains urea, which is metabolized by urease-producing bacteria into ammonia, disrupting the skin’s acid mantle and increasing skin pH. The resulting alkaline environment activates fecal enzymes (proteases and lipases) that degrade the proteins and lipids of the stratum corneum, weakening the barrier and promoting skin breakdown.[40] Increased skin pH leads to [11]:
-
- Overhydration of the stratum corneum
- Excessive permeability to irritants and pathogens
- Increased bacterial colonization
- Damage to lipid structures, further compromising barrier function
- Additional contributors to IAD in newborns include:
-
- Antibiotic use, which alters stool consistency and increases the risk of dermatitis when combined with diaper/brief use.[35]
- Friction during hygiene, which combined with maceration significantly increases skin permeability and susceptibility to irritants and pathogens. [27][28][41]
Microbial Colonization and Secondary Infection in IAD
-
Common microorganisms associated with IAD include C. albicans, Escherichia coli, Clostridioides difficile, Pseudomonas aeruginosa, and Staphylococcus aureus (Figure 7). [8]
- Microbiological confirmation of fungal involvement - most commonly Candida albicans - has been reported in up to 75% of IAD cases, although only 18% of patients present with visible clinical signs of fungal infection. [42]
-
- Routine testing for C. albicans is not standard practice and typically requires 48–72 hours for reliable culture results. As a result, clinical diagnosis and empirical antifungal treatment are commonly employed. This approach, however, may lead to unnecessary treatment in patients without clinical symptoms or delayed management in those with occult fungal involvement.
- Clinical presentation [43]:
-
- Fungal infections often present as erythematous areas or whitish patches with macerated, irregular, white lesion margins.
- Bacterial infections may be suspected in the presence of pain, redness, odor, increased exudate, or wound enlargement.
- Without proper identification, fungal or bacterial infections can spread locally or, in rare cases, lead to systemic involvement. Therefore, microbiological testing is especially valuable in progressive or unresponsive cases to guide targeted therapy. [43]
Figure 7. Common Microorganisms Associated with IAD
ASSESSMENT
This section focuses on elements that need to be included in a comprehensive assessment of patients with IAD.
- All patients with urinary and/or fecal incontinence should undergo regular skin assessments for signs of IAD - at least once daily, and more often if incontinence episodes are frequent.[4][5]
- Assessment for IAD should be integrated into routine skin assessments and carried out within the framework of a pressure injury prevention and continence care program. [5]
- Initial patient assessment should include a comprehensive clinical history and physical examination, with visual inspection of the perineal area to rule out other pathologies (e.g., allergies, atrophic vaginitis). Assessment should also cover mobility, dexterity, and cognitive function, along with urinalysis, a frequency–volume chart, and bowel diary, a post-void residual urine test and a review of the patient’s medication history. [6]
- Primary goals of assessment are:
-
- To identify risk factors for development of IAD or that may impede healing
- To rule out other types of lesions, which may require different treatments.
- To identify pertinent patient's/caregivers' concerns
- To develop a comprehensive care plan
History
The non-exhaustive checklist below highlights relevant factors that should be assessed when taking history of a patient at risk or with IAD. Risk factors for development of IAD are indicated with the icon
Chief Complaint and History of Present Illness
- Age: higher prevalence is observed at the extremes of age: in newborns, children, and the elderly. However, individuals of any age can be affected. [44]
- History/type of incontinence: urinary, fecal, or both
- Location of the lesions: the area affected by IAD can vary significantly, extending beyond the perineum, depending on the skin's exposure to urine and/or feces. [5][39]
-
- In urinary incontinence, IAD typically affects the folds of the labia majora in women, the scrotal area in men, and the inguinal region. In bedbound patients, it also can affect the buttocks. It may also extend to the pubic region and thighs.
- Fecal IAD originates in the perianal area, usually involves the buttocks, and can spread to the genital/inguinal area, the sacrococcygeal area and the posterior thighs.
- Pain: patients with IAD may experience physical discomfort due to pain, itching, burning, or tingling. [45]
- History of prior treatment/prevention
Medications
- Steroids, antibiotic therapy, immunosuppressants [5][17][18]
- Laxatives
Social History
- Caregiver availability
- Inability to perform personal hygiene [5]
Review of Systems
- General:
-
- Critical illness [5]
- Nutrition status: poor nutrition status, hypoproteneinemia [5][17][18]
- Fever [17]
- Endocrine: diabetes mellitus [17]
- Gastro-intestinal/Genito-urinary
-
- Fecal/urine incontinence [5][17][18]
-
- Frequency of evacuation, stool characteristics, use of containment/collection supplies (e.g., incontinence underwear, etc)
- Use of urine collection devices (e.g, catheters)
- Higher overall Perineal Assessment Tool (PAT) score
- Urinary tract infections
- Neurological:
-
- Musculoskeletal:
-
- Skin: poor skin condition (e.g due to aging/steroid use/diabetes). [5]
Structured Risk Assessment
Risk Factors for the Development of Incontinence Associated Dermatitis
- Clinicians might opt to utilize risk assessment scales as tools (e.g. Perineal Assessment Tool) for the early recognition of risks and complications related to IAD.[7]
-
-
Perineal Assessment Tool (PAT): this validated tool can help identify at-risk patients and encourage proactive nursing interventions for IAD prevention (see Table 3). [46]
-
- Each risk factor is scored between 1 (least risk) and 3 (most risk), with one option selected per factor. Total PAD scores can range from a score of 4-6 (low risk) to a score of 7-12 (high risk). [46][47]
Table 3: Risk Assessment Tool for the Development of Incontinence-Associated Dermatitis with the Perineal Assessment Tool (PAT) [46]
| Intensity of the irritant |
Score: 3 |
Score: 2 |
Score: 1 |
| Irritant type and consistency |
Liquid stool with or without urine |
Soft stool with or without urine |
Formed stool and/or urine |
| Duration of exposure: Time of skin exposure to the irritant |
Need for change of sheets or diaper/brief at least every 2 hours |
Need for change of sheets or diaper/brief at least every 4 hours |
Need for change of sheets or diaper/brief at least every 8 hours |
| Perineal skin condition: Integrity of perineal skin |
Denuded/erosions, with or without dermatitis |
Erythema/dermatitis with or without candidiasis |
Clear and intact |
| Contributing factors: Low serum albumin, antibiotic use, feeding catheters, or Clostridioides difficile infection, among others |
Three or more contributing factors |
Two contributing factors |
One or no contributing factor |
Patients'and caregivers' concerns
- Ability to transfer/ turn and reposition assist
- Affordability of care and products
- Psychological and social functioning. [45]
Physical Examination
A focused physical examination that includes the following is recommended:
Skin Assessment
- Assess skin that may be affected: perineum, inner thighs, buttocks, peri-genital region, under pannus, lower back, lower abdomen, and gluteal folds, for the items below (Figure 8) [5][45]:
-
- Maceration
- Erythema
- Presence of lesions (vesicles, papules, pustules, etc)
- Erosion or denudation
- Signs of fungal or bacterial skin infection
- The assessment of the region affected by IAD does not vary by age group but requires expertise in evaluating lesions based on skin color variations.
-
- In individuals with lighter skin tones, IAD initially presents as erythema, which can range from pink to red.
- For patients with darker skin tones, skin color changes may not be visible, making it difficult to identify and differentiate the affected area. The borders of the erosive areas are often hard to delineate and can be irregular. The skin may appear pale or darker, purple, dark red, or yellow (Figure 8). [5][11]
-
- In dark-colored skin, the affected area is harder to visualize, but the presence of maceration is a key indicator of injury. Maceration is directly linked to these lesions and is characterized by skin whitening after prolonged contact with moisture. [2][3]

Figure 8. Incontinence-Associated Dermatitis in the scrotal region and adjacent areas.
Infection
- Assess for signs and symptoms of infection, including:
-
- Fever
- Erythema
- Drainage
- Odor
- Increase in wound size or depth
- Signs of fungal or bacterial skin infection
Diagnosis
- The diagnosis of IAD is based on the clinical and visual assessment of the skin in the entire diaper/brief area and adjacent regions, including the suprapubic region, abdominal folds, inguinal region, and gluteal folds, followed by classification. [5][8]
Differential Diagnosis
- It may be challenging to correctly differentiate IAD from other conditions, including pressure ulcers/injuries (PUs/PIs), contact dermatitis (e.g., from textiles or skin products), infectious lesions (e.g., herpes simplex), or moisture-related skin damage such as intertrigo (see Table 4). [5]
-
- To help distinguish IAD from other conditions, it is important to note that if the patient is not incontinent, the condition is not IAD. [5]
-
Pressure Ulcers/Injuries: IAD is frequently associated with PU/PI in patients with dual incontinence. The damaged skin and excessive moisture exposure increase vulnerability to prolonged pressure (Figures 9 and 10). Misdiagnosing IAD as stage 1 or 2 PU/PI delays appropriate treatment. [29] See topic " Pressure Ulcers/Injuries - Introduction and Assessment".
-
Intertrigo dermatitis: although ITD and IAD share similar precipitating factors, ITD may occur in areas not directly affected by incontinence. ITD typically presents with erythema and scaling, and secondary Candida intertrigo may be suspected when satellite lesions are present. [22]
-
Periwound skin damage: may present with a varying degree of skin maceration, erythema, edema, inflammation, blistering, excoriation, and erosion, caused by prolonged skin contact with wound exudate. [22]
-
Peristomal moisture-associated skin damage: peristomal MASD is inflammation and erosion of the skin related to moisture that begins at the stoma/skin junction and may extend outward. [22]
|
Figure 9. Association of IAD and Stage 2 Pressure Injury
Source: Courtesy of Nurse Sabrina Andrade
|
Figure 10. Association of IAD and Unstageable Pressure Injury
|
Table 4: Differential Diagnosis of Perineal/Perianal Skin Conditions [48]
|
Incontinence Associated Dermatitis |
Intertrigo Candidiasis |
Herpes Zoster |
Pressure ulcer/injury |
| Sample pictures | 
Figure 11. Incontinence associated dermatitis | 
Figure 12. Intertrigo candidiasis, inframmamary fold | 
Figure 13. Herpes zoster on the back | 
Figure 14. Stage 2 pressure ulcer/injury, gluteal region |
| Location |
Perineum
Buttocks
Inner Thighs
Groin
Low abdominal skin folds
|
Perineum
Buttocks
Inner Thighs
Groin
Low abdominal skin folds
|
Perianal
Buttock (unilateral)
Genitals
|
Near bony prominences
Coccyx
Sacrum
Ischium
Under device or tube
|
| Confirmed Risk Factors |
Urinary and/or fecal incontinence |
Moisture
Antibiotics
Immunosuppression
|
Immunosuppression
Elderly
Stress
|
Limited mobility or activity
Dependent on others for repositioning, transferring, etc.
|
| Blisters |
Yes (however, absence does not exclude IAD as a diagnosis) |
No |
Initially vesicles then pustules |
Sometimes (Stage 2 or deep tissue injury) |
| Distribution Pattern |
Confluent or patchy
Irregular edges with erythema
Shallow
denudement and/or maceration
Fleshy part of buttocks
|
Confluent or patchy rash
Small round pustules, plaques, and/or satellite lesions
|
Grouped unilateral distribution of rash or ulcerations along dermatome
Pustules erode into ulcerations
Clusters or isolated individual shallow lesions or blisters
|
Isolated individual lesions on or near bony prominence or pressure causing device
Damage ranges from intact discoloration to partial or full-thickness wounds
|
| Color |
Pink/red |
Pink/red |
Initial: Pink/red
Ulcer may have yellow slough
Later: Crust
Severe cases: Necrosis
|
Pink, red, yellow, tan, gray, brown, black |
| Discomfort |
Pain may be mild to severe |
Itching, burning |
Tingling sometimes noted initially
Often very painful
|
Pain may be absent to severe |
| Diagnostic Tests |
None |
Potassium hydroxide preparation scraping (KOH) |
DNA polymerase chain reaction assay and direct immunofluorescent stain of skin scraping for VZV antigen
Tzanck preparation
Tissue culture
|
None |
Classification Systems
Correct evaluation and classification of IAD require a thorough understanding of its pathophysiology, signs, and symptoms. For this reason, a simple, direct, and easily applicable assessment tool is necessary to standardize IAD evaluations.
- Clinicians might opt to utilize the Ghent Global IAD Categorization Tool (GLOBIAD) for assessing and classifying IAD into categories (See Table 5, Figures 11-14) [4][11][8]:
-
-
Rationale: Multiple instruments have been developed to assess risk factors and aid in the diagnosis of IAD. Although several have demonstrated validity, they are not routinely used in nursing practice, partly due to limited evidence of their impact on clinical decision-making or nursing care improvement. A systematic review evaluated the competence of existing scales, examining included risk factors, reliability, validity, and patient populations tested. Results indicated that several IAD assessment tools are all reliable, valid, and suitable for use in clinical practice (see Appendix, ' IAD Assessment Instruments'). [4] Among the evaluated scales, the GLOBIAD demonstrated a high level of diagnostic accuracy in discriminating erythematous skin and skin loss.[4]
Table 5. Ghent Global IAD Categorization Tool [8]
| Category 1: Persistent redness |
Category 2: Skin loss |
|
1A - Persistent redness without clinical signs of infection

Figure 15. GLOBIAD Category 1A. Source: Sabrina Andrade, RN
Critical criterion
- Persistent redness
-
- A variety of tones of redness may be present.
- Patients with darker skin tones, the skin may be paler or darker than normal, or purple in color
Additional criteria
- Marked areas or discoloration from a previous (healed) skin defect
- Shiny appearance of the skin
- Macerated skin
- Intact vesicles and/or bullae
- Skin may feel tense or swollen at palpation
- Burning, tingling, itching or pain
|
2A - Skin loss without clinical signs of infection

Figure 16. GLOBIAD Category 2A
Critical criterion
- Skin loss
-
- Skin loss may present as skin erosion (may result from damaged/eroded vesicles or bullae), denudation or excoriation.
- The skin damage pattern may be diffuse.
Additional criteria
- Persistent redness
-
- A variety of tones of redness may be present. Patients with darker skin tones, the skin may be paler or darker than normal, or purple in color
- Marked areas or discoloration from a previous (healed) skin defect
- Shiny appearance of the skin
- Macerated skin
- Intact vesicles and/or bullae
- Skin may feel tense or swollen at palpation
- Burning, tingling, itching or pain
|
|
1B - Persistent redness with clinical signs of infection

Figure 17. GLOBIAD Category 1B. Source: Viviany Soares, RN
Critical criteria
- Persistent redness
-
- A variety of tones of redness may be present.
- Patients with darker skin tones, the skin may be paler or darker than normal, or purple in color.
- Signs of infection
-
- Such as white scaling of the skin (suggesting a fungal infection) or satellite lesions (pustules surrounding the lesion, suggesting a Candida albicans fungal infection).
Additional criteria
- Marked areas or discoloration from a previous (healed) skin defect
- Shiny appearance of the skin
- Macerated skin
- Intact vesicles and/or bullae
- The skin may feel tense or swollen at palpation
- Burning, tingling, itching or pain
|
2B - Skin loss with clinical signs of infection

Figure 18. GLOBIAD Category 2B
Critical criteria
- Skin loss
-
- Skin loss may present as skin erosion (may result from damaged/eroded vesicles or bullae), denudation or excoriation.
- The skin damage pattern may be diffuse.
- Signs of infection
-
- Such as white scaling of the skin (suggesting a fungal infection) or satellite lesions (pustules surrounding the lesion, suggesting a Candida albicans fungal infection), slough visible in the wound bed (yellow/brown/greyish), green appearance within the wound bed (suggesting a bacterial infection with Pseudomonas aeruginosa), excessive exudate levels, purulent exudate (pus) or a shiny appearance of the wound bed.
Additional criteria
- Persistent redness
-
- A variety of tones of redness may be present. Patients with darker skin tones, the skin may be paler or darker than normal, or purple in color
- Marked areas or discoloration from a previous (healed) skin defect
- Shiny appearance of the skin
- Macerated skin
- Intact vesicles and/or bullae
- Skin may feel tense or swollen at palpation
- Burning, tingling, itching or pain
|
Ulcer Healability
- IAD is generally healable with early intervention and appropriate care, more severe cases or those with complicating factors may require more intensive and prolonged treatment.
- The healability of Incontinence-Associated Dermatitis (IAD) largely depends on the severity of the condition, the timely implementation of appropriate interventions, and the overall health of the patient. In its early stages, IAD is highly treatable and can often be reversed with proper skin care, such as regular cleansing, the use of moisture barriers, and addressing the underlying incontinence. The skin's ability to heal is typically good when these measures are employed promptly, as long as there is no secondary infection.
- In severe cases, where the skin is significantly damaged or compromised, healing may take longer. The presence of infection, poor nutritional status, or other underlying health issues (e.g., immobility, diabetes) can hinder recovery and make the healing process more complicated. In such cases, a multidisciplinary approach involving wound care specialists, proper management of incontinence, and the use of advanced wound care products is essential for promoting healing.
- For details on ulcer healability, refer to topic " How to Determine Healability of a Chronic Wound".
Documentation
Assessment and documentation of continence status should also include deviations from normal bladder and/or bowel function and any follow-up actions.
- Accurate assessment and diagnosis of incontinence-associated dermatitis (IAD) are essential to ensure:
-
- Patients receive appropriate and timely treatment
- Clinical documentation is complete and accurate
- Quality reporting and correct reimbursement are supported
- For all patients with urinary and/or fecal incontinence, regular skin assessments for signs of IAD are recommended at least once daily, and more frequently if incontinence episodes are recurrent.
- Findings and any required interventions should be documented in the patient’s healthcare record. Documentation should also capture continence status, including deviations from normal bladder and/or bowel function, as well as any follow-up actions taken.
Documentation checklist
Subjective
- Patient’s report: patient's level of discomfort and its characteristics (sensitive, burning, etc.). Specific location of affected area(s).
- Incontinence history: presence of urinary incontinence, fecal or dual incontinence and frequency of episodes throughout the day. Factors that worsen the incontinence. Interventions to manage incontinence.
- Other symptoms: Burning, itching sensation if present. Fever or chills. Other skin irritations.
Objective
Physical examination findings:
- Location: affected areas (buttocks, perineum, inner thighs). [49]
- Severity: degree of erythema, maceration, blisters or open sores.
- Appearance: redness, swelling, shiny skin in the affected area. Moisture level of skin.
- Extent: localized to the perineal region or extending toward other regions such as the inner thighs.
- Exudate: amount, color, odor.
- Signs of infection: fever, increased redness or drainage.
Assessment
- Contributing factors: Persistent incontinence, moisture exposure, and possibly prolonged use of absorbent pads that may not be adequately moisture-wicking. Mobility limitations may contribute to prolonged skin exposure to moisture.
- Risk factors: factors that could hinder skin healing such as immobility, poor nutrition, etc.
Plan
1. Treatment:
- Skin cleansing, barrier products, repositioning, absorbent product use
- Incontinence devices
2. Infection control:
- Interventions to manage bioburden and prevent/manage infection
3. Patient and caregiver education:
- Skin care techniques
- Incontinence management strategies to reduce episodes of leakage and improve skin protection.
4. Follow-up:
- Frequency of reassessment
- Referrals
- If there is no improvement or if the condition worsens, referral to a wound care specialist for advanced management.
CODING
ICD-10
- L24.A2 Irritant contact dermatitis due to fecal, urinary or dual incontinence
- L22 Diaper dermatitis (should not be used in conjunction with L24.A2)
APPENDIX
IAD Assessment Instruments
Table 6. IAD Assessment Instruments [4]
| Abbreviation |
Full Name |
Purpose/Description |
| IADS |
Incontinence-Associated Dermatitis and Its Severity |
Rates the severity of IAD based on observable skin changes |
| IADAS |
Incontinence Associated Dermatitis Assessment Scale (Turkish version) |
Assesses both the presence and severity of IAD |
| IASD.D.2 |
Revised Incontinence-Associated Skin Damage Severity Instrument |
Four categories of IAD (normal, light, medium, and dark skin color) |
| IADIT-D |
The inter-rater reliability of the Incontinence Associated Dermatitis Intervention Tool-D |
Five categories: One item for high risk; Three items for IAD severity; One item for IAD complication |
| GLOBIAD |
Ghent Global IAD Categorization Tool |
High level of diagnostic accuracy in discriminating erythematous skin and skin loss. Category 1: Permanent redness without any clinical infection symptoms Category 2: Skin loss without any clinical infection symptoms. |
| GLOBIAD-M |
Ghent Global IAD Monitoring Tool |
IAD classification according to GLOBIAD (four parameters) |
| MDS-IAD |
Minimum Data Set – Incontinence-Associated Dermatitis |
Type, frequency, and date of incontinence - IAD category and location |