Lesser toe diabetic foot ulcers (DFU) are common and typically secondary to shear and pressure forces on a neuropathic and hammered or clawed toe (Figures 1 and 2). This case demonstrates a classic presentation of a lesser toe diabetic foot ulcer which resolved quickly with percutaneous surgical release of the hammertoe deformity (see video). For a review and updates on offloading devices for DFUs, see topic "Offloading Devices". For decision support on offloading interventions see topic "How to Select Offloading Devices".
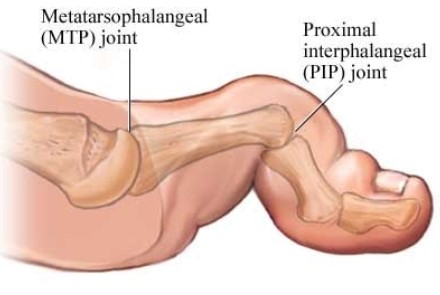
Fig. 1. Hammer toe (distal phalangeal extension)
| 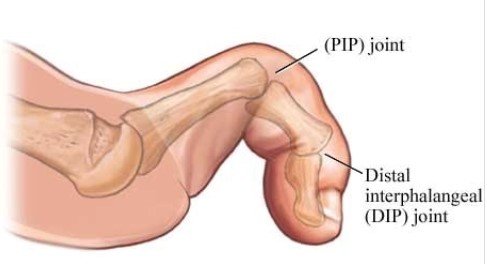
Fig. 2. Claw toe (metatarsophalangeal joint hyperextension with interphalangeal flexion) |
Pathophysiology of the hammer toe
The hammering of the toe occurs as a result of intrinsic minus foot (i.e., a muscle atrophy due to neuropathy), in combination with the accumulation of advanced glycation end-products (AGE) from chronic hyperglycemia.[1][2] AGEs accumulation leads to soft tissue dysfunction, collagen stiffening, and decreased ankle joint mobility. Decreased ankle joint mobility increases stress to the forefoot and metatarsophalangeal (MTP) joints during weight bearing activities.[1][2] This process leads to high pressure points often at the very tip of the toe in the form of hyperkeratosis and ulceration (Figure 3).
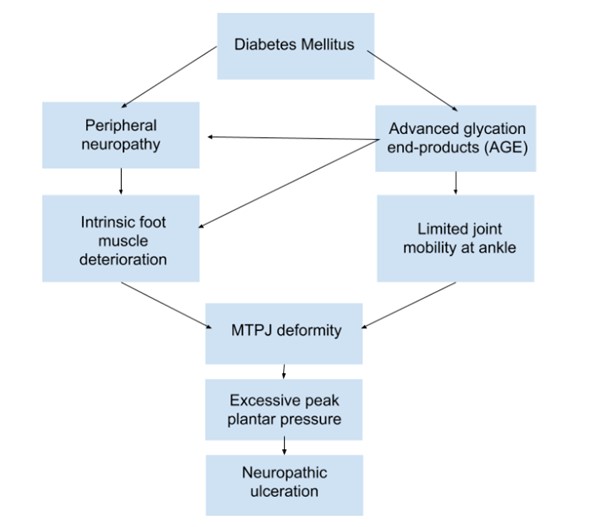
Figure 3. Pathophysiology of the hammer toe (distal phalangeal extension) deformity. Adapted from Cheuy et al.[2]
It is important to note that these lesser toe DFUs are neuropathic ulcers, caused by mechanical forces. These ulcers are distinct from lesions with an eschar or duskiness, which indicate more of an arterial etiology (Figure 4).

Figure 4. Example of arterial ulcer to tip of toe
Ulcers due to neuropathy and hammer toes may be successfully offloaded with multi-density inserts, felt pads, and offloading sandals. However if these conservative methods fail, a flexor tenotomy should be considered.
CASE PRESENTATION
Recurrent lesser toe diabetic foot ulcer (DFU)
An 80-year old female presented with a left third toe ulcer at the tip, secondary to diabetic neuropathy and hammertoe (Figure 5). She had it debrided multiple times over several years, and she had several bouts of cellulitis that were treated with oral antibiotics. The ulcer dimensions waxed and waned. The ulcer healed a few times but kept on recurring despite felt pad offloading and attempts at wearing different types of shoes and insoles.
Physical examination
Upon physical exam, the patient had palpable pedal pulses, frail skin with varicosities, and a contracture of her left third toe that was reducible when an extension force was applied to the toe. Her insoles also demonstrated a deep indentation corresponding to the toe ulcer.

Fig. 5. Diabetic foot ulcer at the tip of the left third toe
Management
Risks and benefits of a percutaneous flexor tenotomy of the toe ulcer were discussed:
- Benefits: The benefit would entail immediate correction of the flexion contracture that could lead to healing and prevention of further episodes of toe tip ulceration.
- Risks: Complication risk is low, with a small chance of infection and continued ulceration to the same toe or the toe next to it. The same toe can ulcerate at the tip because once the flexor tendon is released, the toe will be longer than the others, so although it will no longer cause friction against the ground, if shoes are not worn properly it can then cause pressure against the toe box.
Surgical procedure
Upon discussion of risks and benefits, the patient opted to proceed with the surgical procedure, which was conducted as follows:
- Anesthesia: The procedure was performed under local anesthesia in the clinic room. The toe was anesthetized with a digital block injection.
- Surgical technique (see Video 1):
- The foot was appropriately prepped, and sterile gloves were donned. An 18-gauge needle was inserted into the proximal crease of the toe.
- Using only the tip of the beveled needle edge, multiple careful and superficial passes were made while holding the toe in extension in order to provide tension to the flexor tendons. It is normal to hear a "celery crunch" noise during this part of the procedure. The swiping motion was repeated until all fibers were felt to be freed and the needle tip touched the underlying bone. Transecting part of the plantar capsule of the proximal interphalangeal joint (PIPJ) might be beneficial, in order to facilitate a complete functional release.
- After transection, the patient was asked to attempt to push the surgeon’s hand with the toe(s). Inability to push the surgeon’s hand with the hammered toe confirms successful tendon transection. With this percutaneous technique, everything is done by feel, and sometimes there are a few slips of tendon that is not fully transected yet. By asking the patient to flex her toes, the muscle activation will apply tension to the remaining slips of tendon, thereby completing the transection, sometimes with an audible “pop”. After a complete transection, the toe usually will appear noticeably extended and longer than before surgery.
Video 1. Flexor Tenotomy
- Postoperative care: Ulcers may be dressed with gauze and bandage (e.g. Coban™), and patients are sent home in the shoes they wore to the appointment that day. The patient is advised to keep the dressing dry, but can remove the dressing in 3-4 days and shower as usual. Typically pain is very minimal and will require only paracetamol or nonsteroidal anti-inflammatory drugs. The patient is usually asked to return for follow up in 1 week.
- The puncture site is typically healed in a few days. Regular weekly visits are continued with debridement of the ulcer until healing. Most ulcers are healed within a month (Figures 6 and 7).

Fig. 6. Eleven days after surgical offloading | 
Fig. 7. One month after surgical offloading |
DISCUSSION
This case demonstrates a classic presentation of a lesser toe DFU which resolved quickly with percutaneous surgical release of the hammertoe deformity. The procedure is safe and effective. Usually, for patients with lesser toe DFUs, the author will initially attempt conservative treatment, but if the ulcer size expands or stays the same for 2 consecutive weeks, surgical release will be discussed. Even with completely rigid hammertoes, releasing the tendon promotes ulcer healing because the release removes the active plantar flexion force of the toe.
This procedure has been reported to be safely performed in patients with active cellulitis or osteomyelitis localized to the tip of the toe. However, for these patients with active infection and/or uncontrolled diabetes, clinicians should discuss the risk of spreading and seeding infection beyond the local affected tissue.
Key Takeaways
Some of the main takeaways from this case study are: - For lesser toe DFUs secondary to a hammer toe, conservative treatment with local wound care, adequate offloading, and glucose control may be attempted. However, if the ulcer does not show signs of improvement within 2 weeks, flexor tenotomy may be a safe and effective procedure to surgically correct the hammertoe deformity and promote DFU healing.
|