Last updated on 10/29/24 | First published on 3/2/18 | Literature review current through Jun. 2026
[cite]
Authors:
Tiffany Hamm BSN, RN, CWS, ACHRN, UHMSADS,
Jeff Mize RRT, CHT, UHMSADS,
Elaine Horibe Song MD, PhD, MBA,
Topic editors:
Mike White MD, UHM, MMM, CWS,
Jeff Althoff MD, FACEP/UHM,
more...
Coauthor(s)
Tiffany Hamm, BSN, RN, CWS, ACHRN, UHMSADS
Chief Nursing Officer, Wound Reference, IncDisclosures: Nothing to disclose
Jeff Mize, RRT, CHT, UHMSADS
Disclosures: Nothing to disclose
Elaine Horibe Song, MD, PhD, MBACo-Founder and Editor, Wound Reference, Inc;
Professor (Affiliate), Division of Plastic Surgery, Federal University of Sao Paulo;
Volunteer, Association for the Advancement of Wound Care;
Google Scholar Profile
Disclosures: Nothing to disclose
Editors
Mike White, MD, UHM, MMM, CWS
Disclosures: Nothing to disclose
Jeff Althoff, MD, FACEP/UHM
Disclosures: Nothing to disclose
INTRODUCTION
The most common type of barotrauma experienced by patients receiving HBOT is middle-ear barotrauma (MEB). Normally, the middle ear is a closed, vascular lined space and therefore subject to pressure change. Then normal means by which the middle ear remains at an equal pressure with the surrounding tissue is through the opening of the Eustachian tube. During descent, the increasing pressure of the surrounding water leads to “middle-ear squeeze.” If a patient is suffering from Eustachian tube dysfunction, he or she likely will be unable to equalize and will subsequently develop middle-ear barotrauma.[1]
Etiology
There are numerous etiologies for Eustachian tube dysfunction including:
- Otitis media
- Mastoiditis
- Seasonal allergies
- Upper respiratory infections
- Large adenoids/tonsils
- Nasal septum deviation
ASSESSMENT
Who should evaluate otic barotrauma?
Typically, the nurse or physician should evaluate for middle-ear barotrauma. The nurse may note signs and symptoms and communicate with the provider who should perform an exam of the tympanic membrane and provide diagnosis, intervention and treatment. Only properly trained staff working within their scope of practice should evaluate otic barotrauma.
History
The most notable initial symptom is middle-ear barotrauma is ear pain during descent. If descent is not stopped, and MEB occurs, patients may experience transient conductive hearing loss, vertigo or tinnitus. In severe cases, tympanic membrane perforation may occur and is often described as severe pain followed by instant relief upon rupture.
Symptoms of middle-ear barotrauma are recognizable. A sensation of pressure and pain initially develops. As the pressure differential increases, the severity of symptoms increases as well. Otoscopic findings can be seen fairly quickly after the onset of injury and may progress over minutes to hours.
Physical Examination
In 1944, Reed Wallace Teed developed a scale for describing the clinical appearance and severity of injury from otic barotrauma.[2] The table below shows the modified TEED Scale for examination of tympanic membrane barotrauma.[3][4][5][6]
| LEVEL |
DESCRIPTION |
PICTURE |
| TEED 0 |
Normal tympanic membrane. No evidence of injury despite the presence of symptoms. |
|
| TEED 1 |
Diffuse redness and retraction of tympanic membrane. Erythema over part of the tympanic membrane due to inflammation, particularly around the manubrium. |

|
| TEED 2 |
Diffuse redness and retraction of tympanic membrane, plus slight hemorrhage within the tympanic membrane. |

|
| TEED 3 |
Diffuse redness and retraction of tympanic membrane, plus gross hemorrhage within the tympanic membrane. |

|
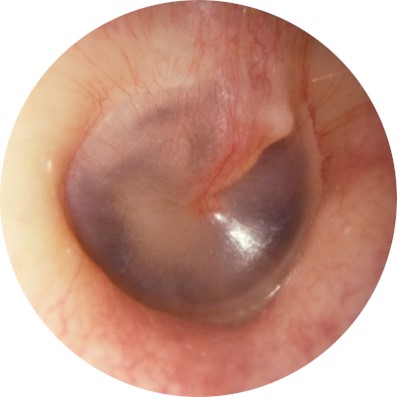
| TEED 4 |
Dark and slightly bulging tympanic membrane due to free blood in the middle ear (a fluid level may also be present). |

|
| TEED 5 |
Free hemorrhage into the middle ear, tympanic membrane perforation; blood may be visible outside or within the external auditory canal. |

|
TREATMENT
MEB is usually avoidable with simple preventative measures for pressure equalization and include:
- Yawning
- Swallowing fluids
- Toynbee maneuver: the patient closes the mouth and nose and swallows
- Modified Valsalva: performed by forcefully blowing against a closed nose and mouth while maintaining an open glottis. This maneuver is less favorable as it increases intracranial pressure that is transmitted though the inner ear, resulting in round-window rupture
- Tilting the head to place the affected ear in an up position may provide added benefit by stretching the involved muscles and Eustachian tube opening
For patients with Eustachian tube dysfunction who do not respond to decongestant therapy, experience significant pain, and are unable to equalize middle ear pressure due to altered airway anatomy, tympanostomy tubes (also known as ventilation tubes, myringotomy tubes or pressure equalization tubes) should be considered.[3]
Nursing Interventions
Ear, Sinus, Tooth Barotraumas
- Screen patient for history of sinus, tooth, and ear problems, especially with situations involving pressure changes.
- If patient has history of dental caries, explain that problems may occur. Compress slowly, observing patient for signs of tooth pain. Notify hyperbaric physician if dental pain occurs. Document on patient record.
- Hyperbaric staff to examine patient’s ears prior to and following first treatment, then PRN/part-time to decrease possibility of pressure discomfort during treatment;
- Instruct patients in the use of techniques to equalize pressure in the ears. The methods include jaw movement, Toynbee maneuver, modified Valsalva maneuver, and yawn;
- If indicated, hyperbaric physician will consult with ENT service to evaluate Eustachian tube function and determine possible need for tympanostomy tubes;
- Administer prophylactic agents (decongestant nasal spray or oral antihistamines) per physician order.
- Compress patients at a rate (1-2 psi) that is comfortable for ear equalization. Remind patient to equilibrate ears during compression. Maintain direct visual contact with patient during all changes in pressures.
- Staff may hold or decrease pressure if patient is having mild to moderate pain in ears, resume pressurization when pain subsides.
- If ear pain or discomfort becomes severe and pain does not subside when pressurization is held or decreased, interrupt treatment, decompress chamber. At surface pressure, hyperbaric physician to examine patient’s ears for evidence of barotrauma. Document findings and any management.
Ear/Sinus Equalization During Compression
- Immediately halt compression, by adjusting set pressure gauge to read present chamber pressure.
- Instruct the patient not to attempt further equalization unless instructed.
- Inform the patient that you plan to reduce the chamber pressure slightly.
- Reduce pressure 1 psi below existing chamber pressure. Rate can be increased as indicated.
- At reduced pressure ask the patient to reattempt equalization, with light pressure.
- If equalization occurs, resume normal compression procedure, note difficulty on patient record.
- If equalization does not occur after 2-3 attempts, advise patient of further pressure reduction.
- If equalization is still incomplete, inform patient they will be returned to surface pressure.
- Reduce pressure to zero, set rate at 1 psi/min. (Refer to S.O.P. Decompression.)
- At the surface, remove patient from chamber, have ears examined. Consult with hyperbaric physician on-call as necessary. Nasal decongestants may be indicated if barotrauma is not severe.
- Myringotomy tubes may be indicated if barotrauma is severe. Prevention of middle-ear barotrauma is clearly the best management technique. Prevention involves appropriate patient instruction, evaluation of risk factors, and rapid recognition of patients who experience difficulty with middle-ear pressure equalization.
Official reprint from WoundReference® woundreference.com ©2026 Wound Reference, Inc. All Rights Reserved
Use of WoundReference is subject to the
Subscription and License Agreement.
NOTE: This is a controlled document. This document is not a substitute for proper training, experience, and exercising of professional judgment. While every effort has been made to ensure the accuracy of the contents, neither the authors nor the Wound Reference, Inc. give any guarantee as to the accuracy of the information contained in them nor accept any liability, with respect to loss, damage, injury or expense arising from any such errors or omissions in the contents of the work.