This topic provides decision support on identification of skin failure, pressure ulcer/injury (PU/PI) and other conditions. For a practical perspective on differentiating Stage 2 PU/PI on the gluteal region from selected common conditions see topic "Pressure Ulcers/Injuries - Is it Really a Stage 2?". For a list of guidelines and quality measures related to PU/PI, see topic "Pressure Ulcers/Injuries - Overview". For an introduction and assessment of PU/PI including epidemiology, risk factors, etiology, pathophysiology, history, physical examination, diagnosis, differential diagnoses, documentation and ICD-10 coding, see "Pressure Ulcers/Injuries - Introduction and Assessment". For management of PU/PI, see topic "Pressure Ulcers/Injuries - Treatment". For a systematic approach to identifying patients at risk for developing pressure ulcers/injuries (PUs/PIs) and developing specific care plans, see topic "Pressure Ulcers/Injuries - Prevention". For best practices in care coordination, see topic "Pressure Ulcers/Injuries -Coordination of Care".
This topic provides decision support on differentiation among skin failure, PU/PI and other conditions.
Definitions
- Skin failure: this topic uses the following definition of skin failure proposed by Levine [11]: "Skin failure is the state in which tissue tolerance is so compromised that cells can no longer survive in zones of physiologic impairment such as hypoxia, local mechanical stresses, impaired delivery of nutrients, and buildup of toxic metabolic by products". This definition builds upon the original definition by Langemo and Brown [1], in which skin failure is “an event in which the skin and underlying tissue die due to hypoperfusion that occurs concurrent with severe dysfunction or failure of other organ systems.”[3]
- The use of the term 'skin failure' as described above represents an attempt to provide a common term for skin changes at the end-of-life (e.g. KTU, SCALE, TB-TTI) and other acute states that compromise skin integrity.[3] According to Levine, skin failure is the underlying pathophysiology of wounds occurring in “patients close to death, unavoidable pressure injuries, and skin impairment related to tissue ischemia.”[10][12] In this proposed concept, the etiology of skin failure is different than that of [an avoidable] PU/PI, although PU/PI and skin failure can occur concomitantly.[3]
- Although this classification is subjective and not based on any clearly objective criteria, three types of skin failure have been described and accepted: acute, chronic, and end-stage.[1][3][5][10]
- Acute skin failure occurs concurrently with an acute illness such as septic shock or myocardial infarction; it has been defined as the "hypoperfusion state that leads to tissue death that occurs simultaneously to a critical illness.”[1][3][5][10]
- A retrospective study showed that among critically ill patients, peripheral arterial disease, mechanical ventilation for more than 72 hours, respiratory failure, liver failure, and severe sepsis/septic shock are statistically significant and independent predictors of acute skin failure (low certainty evidence, level C). [13]
- Chronic skin failure occurs concurrently with a chronic condition such as multiple sclerosis or a malignancy.[1][3][5][10]
- End-stage skin failure occurs concurrently with end-of-life issues such as renal failure, pulmonary fibrosis, and so on.[1][3][5][10]
- For instance, a KTU is believed to be a manifestation of skin failure in patients at end-of-life.[7][10][14]
- TB-TTI is considered a manifestation of skin failure at the end-of-life.[15]
- Of note, currently there is no agreed-upon definition of skin failure.[3][9] Multiple consensus documents recognize the phenomenon of skin failure.[5][9] However, a recent comprehensive review of 180 papers using the term "skin failure", found no consistent definition of the term.[9] Among the multiple definitions found by the review authors, three clear themes were identified [9]:
- 1) The most common definition of skin failure in literature is used primarily in the dermatology field, where skin failure relates to "failure of skin, as an organ, to function as required". Conditions described in this context include Steven Johnson syndrome and toxic epidermal necrolysis.
- 2) The second most common definition of skin failure is employed primarily in the skin integrity/wound care literature and focuses on "hypoperfusion and hemodynamic instability" as described above and adopted in this topic.
- In a terminology survey, most wound care clinicians agreed that "skin failure is an event in which the skin and underlying tissue dies because of hypoperfusion and occurs concurrently with severe failure of other organ systems (two or more)".[5]
- 3) And the least common definition relates to "tissue tolerance".
- Avoidable versus unavoidable lesions: The differential diagnosis between an avoidable and unavoidable injury is key in diagnosing skin failure or pressure injuries.[8] The Centers for Medicare and Medicaid (CMS)'s definition of avoidable and unavoidable pressure injuries is accepted by most wound care clinicians.[5]
- According to CMS [16]:
- “Avoidable” means that the individual developed a pressure ulcer/injury and that the facility did not do one or more of the following: evaluate the individual’s clinical condition and risk factors; define and implement interventions that are consistent with individual needs, goals, and professional standards of practice; monitor and evaluate the impact of the interventions; or revise the interventions as appropriate.
- “Unavoidable” means that the individual developed a pressure ulcer/injury even though the facility had evaluated the individual’s clinical condition and risk factors; defined and implemented interventions that are consistent with individual needs, goals, and professional standards of practice; monitored and evaluated the impact of the interventions; and revised the approaches as appropriate.
- The National Pressure Injury Advisory Panel (NPIAP) provides examples of situations in which PU/PI may be unavoidable (e.g. when an individual is repositioned and alterations in hemodynamic stability require ongoing vasopressor support). See section 'Background in topic "Pressure Ulcers/Injuries - Introduction and Assessment".[17]
- Many clinicians believe that KTUs, SCALE, or TB-TTIs should not be considered PUs/PIs, but the literature on this subject remains unclear.[3] However, there is consensus that KTU, TB-TTI, SCALE, and skin failure at the end-of-life are unavoidable and not attributable to substandard care.[3][5]
Relevance
Inaccurately labeling skin changes at the end-of-life as avoidable pressure injuries (or the other way around), not only has clinical implications but also legal, financial and psychological repercussions. On the other hand, an accurate diagnosis leads to more appropriate treatment interventions, improved care, less wasted resources, and reduced financial penalties and medicolegal claims.[7] For instance:
- Misdiagnosis of skin failure as a facility-acquired Stage 3 or Stage 4 PU/PI can have a substantial financial impact.[4]
- Along the many CMS “value-based purchasing” initiatives, in 2008 the CMS decided not to reimburse hospitals for Stage 3 and 4 PU/PI that were not present on admission.[18] As a result, mislabeling skin failure as facility-acquired PU/PI can result in undesirable financial consequences to the hospital.
- Misdiagnosis of avoidable facility-acquired Stage 3 or Stage 4 PU/PI or other lesions as skin failure may lead to quality, medicolegal and psychological implications.
- Patients and families may be subject to additional confusion and emotional distress[11], increasing legal risks.
- If indeed a facility-acquired lesion develops, mislabeling it as skin failure may obscure the opportunity for professional education on PU/PI prevention, quality of care improvement and further prevention initiatives of facility-acquired PUs/PIs.
Epidemiology
Caution is needed in interpretation of epidemiological data on skin failure and related manifestations. Inconsistent terminology, lack of criteria for diagnosis or incomplete chart documentation impact data accuracy.[10][14]
Prevalence
- KTU: a KTU prevalence of 6.1% was reported by a retrospective study that included 363 charts of hospice patients.[19] Due to lack of detailed chart documentation, authors adopted a loose definition for KTU: the presence of sacral and coccyx ulcers after hospice admission. Thus, caution is needed in interpretation as not all sacral and coccyx ulcers are KTUs.[14]
- TB-TTI: a TBTTI prevalence of 5% was reported by Brennan and Trombley after a 12-month observational study in their palliative care unit.[20]
Risk Factors
Skin failure seems to be multifactorial and due to comorbidities that can reduce angiosome perfusion (low certainty evidence, level C).[7]
Most influential factors that increase the risk of developing skin failure (e.g. acute skin failure, KTU, TB-TTI, SCALE) include:
- Hypotension/shock [7]
- Mean arterial pressure less than 60 [7]
- Presence of sepsis or multiorgan dysfunction syndrome [4][21]:
- Vasopressor/inotrope use [4][7]
- Hypoalbuminemia [21][22]: serum albumin level less than 3.5 mg/dL [4]
- Primary diagnosis related to alteration of blood flow (e.g. cardiovascular/ vascular /dyscrasias such as disseminated intravascular coagulopathy, clotting abnormalities / other related) [4][21][23]
- Respiratory insufficiency [21][23]: mechanical ventilation (any length of time on mechanical ventilation)[4]
- Renal insufficiency [22][21]
- Others: obesity [23], low weight, loss of appetite, cachexia, reduced mobility, poor or inadequate nutrition [22]
Etiology
- The wound care/skin integrity literature on skin failure agree that their etiology and pathophysiology is still unknown. It is theorized that skin failure manifestations result from hypoperfusion that occurs concurrently with severe dysfunction or failure of other organ systems.[3][7][12]
- For anatomical locations subject to pressure (e.g. sacrum, heels), pressure and shear may play a role despite not being direct causes.[4][8][5]
Pathophysiology
Skin failure is a complex phenomenon that occurs as a result of multiple pre-existing acute and chronic conditions, comorbidities, and cellular interactions.[6] These include hypoperfusion, hypoxia, inflammation, vascular permeability and edema.[6]
- As an example of how these factors interact, when blood flow of a specific artery is impaired due to a pre-existing chronic condition such as atherosclerosis, the areas of skin perfused by that artery will be more prone to skin failure than other areas. If additional comorbidities such as diabetes mellitus microvascular disease or anemia are present, the susceptibility of these areas to hypoperfusion and hypoxia will be further increased.[6]
To better understand the proposed pathophysiology of skin failure, it is important review the skin anatomy and understand the angiosome concept.[7] For details on skin anatomy and function, see topic "The Skin".
Angiosomes
- Angiosomes are a concept described by Taylor and Palmer in 1987.[24] These authors defined angiosome as a three-dimensional block of tissue composed of skin, fat, muscle and bone (or any combination of these tissues) that is supplied by a single source vessel.[24] According to this concept, the location of an ulcer may offer a hint on which arteries are affected by stenosis or occlusion, in light of the corresponding angiosome.
- Angiosomes are connected to each other by two different types of vessels: choke vessels and true anastomoses.[25] Thus, an angiosome is a three-dimensional block of tissue supplied by a source vessel with its boundary outlined either by an anastomotic perimeter of reduced-caliber choke vessels or by true anastomoses with no reduction of vessel caliber.[25]
- Choke vessels are smaller caliber vessels that are subject to spasm. However, it is still unknown what “triggers” these vessels to go into spasm (e.g. critical perfusion pressure, oxygen tension, reaction to toxin, or other).[25]
- True anastomoses are not subject to spasm and allow free flow between angiosomes, effectively linking them together as one.[25]
- Functional angiosome: a functional angiosome has been defined as the block of tissue that clinically can be captured safely on a single source vessel (e.g. when planning for a flap reconstruction) (Figure 1). That is, it is a three-dimensional block of tissue, the size and shape of which are intimately dependent on the vessels (choke or true) that interconnect the source vessel’s anatomical angiosome with its neighboring anatomical territories.[25]
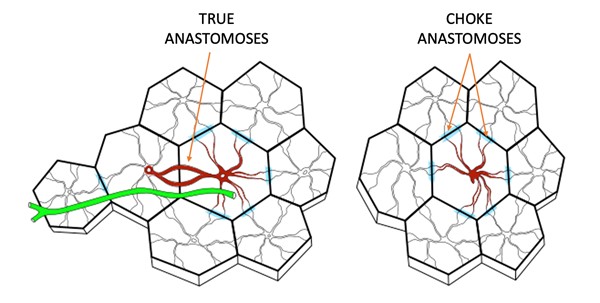
Figure 1. Schematic diagram of functional angiosomes. Left: longer skin flap where several perforator angiosomes are connected by true anastomoses with the central angiosome that is nurtured by a single perforator. A nerve is shown in green. Right: adjacent perforator angiosomes that are viable thanks to blood flowing from choke anastomoses that connect the adjacent angiosomes with the angiosome at the center, nurtured by a single perforator [25]
Pathophysiology of acute skin failure
- It is hypothesized that manifestations of acute skin failure result from decreased perfusion within a functional angiosome, inability of arterial anastomotic connections to augment flow, and lack of time for choke vessels to respond and vasodilate followed by tissue ischemia.[7]
Pathophysiology of end-stage skin failure
- Terminal ulcers such as KTU may be caused by a decrease in blood flow to the affected area (hypoperfusion), produced in turn by severe organ dysfunction or failure. In the presence of hypotension, blood is shunted from the periphery and gastrointestinal tract to the head, neck and other major areas.[7][14] Vasopressor medications for certain diseases at the end-of-life may further divert blood flow to other vital organs.[8] For anatomical locations subject to pressure (e.g. sacrum, heels), pressure and shear may play a role in the development of skin breakdown despite not being direct causes.[4][8][5]
- Figure 2 illustrates a KTU whose location appears to correlate with the sacral angiosome.[7][26]

Figure 2. Kennedy terminal ulcer on the sacral area, which appears to correlate with the sacral angiosome
- Figure 3 illustrates a lesion characteristic of the "3:30 syndrome", a type of KTU. Its pathophysiology is compatible with superior gluteal artery compromise for which the corresponding anatomy is also shown. [7]

Figure 3. 3:30 syndrome, a type of Kennedy Terminal Ulcer. The area of the lesion appears to correlate with compromise of the superior gluteal artery
Pathophysiology of unavoidable pressure ulcer/injury
- The angiosomal hypothesis may also help explain the pathophysiology of unavoidable PUs/PIs.[27]
ASSESSMENT
Patients with skin failure frequently are severely ill and/or present with multiple comorbidities leading to tissue hypoperfusion. Thus, it is recommended that a qualified professional multidisciplinary team evaluate and perform a complete assessment of the patient. It is important to obtain a comprehensive history of the patient’s current condition, past medical and surgical history, medications, and other risk factors related to skin failure. Differentiating between avoidable and unavoidable injuries is key.[8]
See Algorithm for Assessment of Skin Failure below (Algorithm 1).
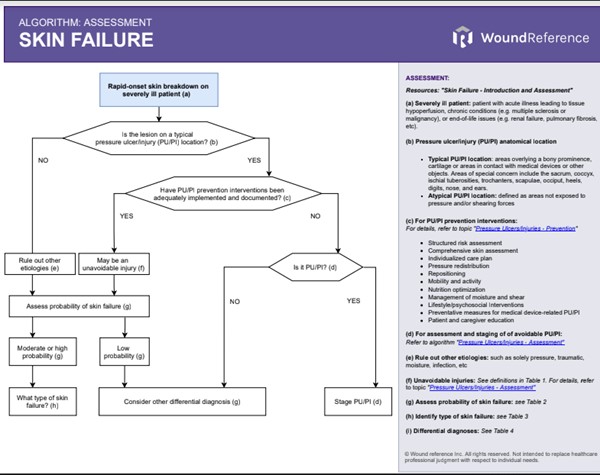
Algorithm 1. Algorithm for Assessment of Skin Failure (click this link to enlarge)
History
The non-exhaustive checklist below highlights relevant factors that should be assessed when suspicion of skin failure exists. Risk factors for development of skin failure are indicated with the icon
Chief Complaint and History of Present Illness
- Onset: rapid onset of skin breakdown
- Location: lesion on areas not subject to pressure and shear could be indicative of skin failure.[4] For areas subject to pressure and shear, pressure as a causative factor should be ruled out.[4]
- History of acute illness leading to tissue hypoperfusion (e.g. septic shock or myocardial infarction), chronic condition (e.g. multiple sclerosis or malignancy), or end-of-life issues (e.g. renal failure, pulmonary fibrosis, etc) [13][3][10]
Medications
- Vasopressor/inotrope use [4][7]
Review of Systems
- General:
- Hypotension/shock [7]
- Mean arterial pressure less than 60 [7]
- Presence of sepsis or multiorgan dysfunction syndrome [4][21]:
- Cardiovascular:
- Primary diagnosis related to alteration of blood flow (e.g. cardiovascular/ vascular /dyscrasias such as disseminated intravascular coagulopathy/ other related) [4][21][23]
- Respiratory:
- Respiratory insufficiency [21][23]: mechanical ventilation (any length of time on mechanical ventilation) [4]
- Gastro-intestinal/ Genito-urinary
- Renal insufficiency [21][22]
- Musculoskeletal
- Impaired mobility and interventions in place to prevent PU/PI [28]
Nutritional Assessment
- Hypoalbuminemia [21][22]: serum albumin level less than 3.5 mg/dL [4]
- Obesity [23], low weight, loss of appetite, cachexia, reduced mobility, poor or inadequate nutrition [22]
Physical Examination
Table 1 summarizes the clinical characteristics of KTU, TB-TTI and SCALE.
TABLE 1. Summary of clinical characteristics of Kennedy Terminal Ulcer, Trombley-Brennan terminal tissue injuries and Skin Changes At Life’s End
Term (abbreviation, year published)
| Kennedy Terminal Ulcer (KTU, 1989)
| Trombley-Brennan terminal tissue injuries (TB-TTI, 2010)
| Skin changes at the end of life (SCALE, 2008)
|
| Pictures | 
Fig. 4. Butterly-shaped KTU | 
Fig. 5. TB-TTI on the left leg | 
Fig. 6. SCALE (e.g. livedo reticularis) |
Definition
| The KTU was one of the first terminal ulcers reported in modern literature.[29][5] KTU is defined as a red, yellow, and/or black pear-shaped lesion that appears suddenly. It may be on intact skin or form an erosion (ie, loss of epidermis with an epidermal base) or an ulcer (ie, loss of epidermis with a dermal or deeper base).[29] In a terminology survey, most wound clinicians agreed that [5]: - KTUs are prognostic of impending death (within a 6-wk period and up to 55.7% as documented in Karen Lou Kennedy data)
- KTUs are attributable to local ischemia and are less likely to be a primary pressure injury
| - Spontaneously appearing skin alterations (rapid evolution, speed of enlargement and progression, appearance in areas of little to no pressure such as shins and thighs, and mirror imaging found in patients at the end of life).[30][15]
- Unavoidable occurrence - one that is related to organ failure at the end of life.[3][5][30]
| - A mnemonic used to describe a group of clinical phenomena [22]
- "Physiological changes that occur as a result of the dying process may affect the skin and soft tissues and may manifest as observable (objective) changes in skin color, turgor, or integrity, or as subjective symptoms such as localized pain".[22]
- The changes can be unavoidable and may occur with the application of appropriate interventions that meet or exceed the standard of care.[22]
- The changes outlined in the SCALE statements can occur in the absence of skin failure.[5]
|
Characteristics
| KTUs appear suddenly and within hours. There are 2 agreed presentations: bilateral and unilateral [14][29]: - Bilateral KTU is a butterfly-, horseshoe-, or pear-shaped lesion, with irregular margins. The lesion suddenly appears on the patient’s sacrum or coccyx, 2 weeks to several months prior to their death. First appearing as erythematous and/or purpuric, bilateral KTUs then progress to a yellow and/or black color, with the presence or absence of epidermal erosion.
- Unilateral KTU, also known as ‘‘3:30 syndrome,’’ is a macular lesion of less than 1cm2, which is either purpuric or has irregular black margins and appears on only 1 buttock. This rapidly developing lesion is seen 8 to 24 hours prior to death, with the absence of epidermal erosion. The term ‘‘3:30 syndrome’’ was coined for unilateral KTU because this was often the time of day when staff observed these rapid skin changes.[3][14]
| Sudden onset, appears hours or days before death, never weeks.[8] Consensus has been reached that Trombley-Brennan terminal tissue injuries may represent hypoperfusion and leaky superficial vessels resulting in three of the following [5]: - a) Pink purple maroon bruise like butterfly skin alterations.
- b) Vertical-linear striations particularly on the legs or horizontal striations with purpura on the abdomen.
- c) These changes do not ulcer or breakdown, in contrast with KTU
Most (60%) wounds exhibit a linear pattern, followed by a butterfly pattern, and a few present with a white center.[15] | - Diminished tissue perfusion, impaired skin oxygenation, decreased local skin temperature, mottled discoloration, and skin necrosis.[22]
- The SCALE concept represents the loss of skin integrity from any of a number of factors, including but not limited to equipment or devices, incontinence, chemical irritants, chronic exposure to body fluids, skin tears, pressure, shear, friction, and/or infections.[3][22]
|
Diagnosis
Specialized clinician knowledge and skills are required when diagnosing manifestations of skin failure.[14] The information below offers some guidance on this process:
- For lesions on anatomical areas subject to pressure and shear (e.g. sacrum, heels), it is essential that clinicians demonstrate that appropriate measures were in place to prevent PU/PI before labeling the lesion as a clinical manifestation of skin failure.[6] Clinical manifestations of skin failure are considered unavoidable despite preventative measures.[3][5] Wounds resulting from inadequate prevention strategies should not be labeled as skin failure or acute skin failure.[6]
- PU/PI and skin failure may occur simultaneously, and it can be difficult to distinguish PU/PI from skin failure. One differentiating factor is that PU/PI can develop in otherwise healthy individuals, because of unrelieved pressure resulting in tissue ischemia and necrosis.[9] In contrast, skin failure occurs in individuals with acute illness leading to tissue hypoperfusion, chronic conditions (e.g. multiple sclerosis or malignancy), or end-of-life issues (e.g. renal failure, pulmonary fibrosis, etc).[9] See Figures 7, 8 and 9.
- To date, no validated assessment tools are available that can help definitively distinguish skin failure from a PU/PI.[4] Algorithm 1 was developed based on the Skin Failure Clinical Indicator Scale (SFCIS) proposed by Hill et al.[4] This scale has yet to be validated, but it may help recognize and diagnose skin failure, initiate appropriate interventions, and decrease potential reimbursement penalties to facilities.[4]
- The SFCIS tool uses readily available variables to assess the probability that a given lesion occurred due to skin failure.[4] SFCIS authors found that patient age, Braden score, and BMI were not significant predictors of skin failure. On the other hand, factors found to help distinguish between skin failure and PU/PI included a serum albumin level less than 3.5 mg/dL (P= .07), impaired blood flow (P= .05), presence of sepsis/ multiorgan dysfunction syndrome (P = .001), vasopressor/inotrope use (P< .001), and mechanical ventilation (P= .06), which ultimately correctly identified 83.7% as cases of probable skin failure in that retrospective series.[4]
 Fig. 7. Skin failure of the sacral angiosome in a critically ill patient who expired 2 weeks after onset Fig. 7. Skin failure of the sacral angiosome in a critically ill patient who expired 2 weeks after onset
|  Fig. 8. The necrotic area shown in Figure 7 ended up being debrided. Hypoperfused tissue is shown in the wound bed Fig. 8. The necrotic area shown in Figure 7 ended up being debrided. Hypoperfused tissue is shown in the wound bed
|  Fig. 9. A few days after debridement, the wound bed showed progressive necrosis. Other areas also suffered skin breakdown Fig. 9. A few days after debridement, the wound bed showed progressive necrosis. Other areas also suffered skin breakdown
|
Differential Diagnosis
Differential diagnosis of skin failure include:
- PU/PI (e.g. deep tissue injury): as mentioned previously, the main difference from PU/PI is in the etiology. PU/PI are formed due to pressure and shear. PU/PI and skin failure may occur simultaneously in areas subject to pressure. However, skin damage resulting from skin failure alone may appear in areas that are not subject to pressure.[10] See topic "Pressure Ulcers/Injuries - Introduction and Assessment"
- Incontinence associated dermatitis: caused by exposure of the skin to urine and/or feces, most often found in the perianal area, buttocks, inner thighs and perineum. Appears as an inflamed area with an erythematous appearance, has irregular and diffuse edges, is shallow in depth and there is no eschar or granulation tissue.[8] See topic "Pressure Ulcers/Injuries - Is it Really a Stage 2?"
- Gluteal compartment syndrome: may be caused by hypogastric artery compression, prolonged immobilization, drug addiction, alcoholism or surgery. It is purple and is rarely caused by pressure.[8]
- Traumatic wounds (skin tears, burns, abrasions)
Documentation
Currently, CMS does not provide statements guiding documentation of terminal skin injuries in acute care or in the Resident Assessment Instrument manual for LTC, long-term acute-care hospitals, or inpatient rehabilitation facilities.[3] However, CMS provides statements in the CMS' State Operations Manual: Guidance to Surveyors for Long Term Care Facilities, more specifically on KTUs (see section 'Documentation: Kennedy Terminal Ulcer (KTU)' below.
For all manifestations of skin failure, it is important that medical documentation supports reasons why lesions are considered "unavoidable" and includes findings that support their etiology.
Documentation of "unavoidability"
To support the classification of a lesion as resulting from skin failure, documentation that appropriate preventative measures were in place to prevent PU/PI is essential. That is, documentation should state that the individual developed skin breakdown even though the facility had evaluated the individual’s clinical condition and risk factors; defined and implemented interventions that are consistent with individual needs, goals, and professional standards of practice; monitored and evaluated the impact of the interventions; and revised the approaches as appropriate.[3]
Hospital-acquired pressure injuries unavoidability rests with the documentation of appropriate interventions and not necessarily with the identification of clinical risk factors.[28]
Documentation of findings supporting etiology
Documentation should include a comprehensive patient assessment including observed risk factors and underlying illnesses.[6] Findings that support skin failure should be documented:
- See sections 'Risk factors', 'History' and 'Physical Exam' above
Kennedy Terminal Ulcers (KTUs)
According to the CMS's State Operations Manual: Guidance to Surveyors (F686), KTU is a PU/PI that occurs at the end-of-life.[16] Regarding PU/PI that occurs at the end-of-life, CMS states that if the facility has implemented adequate preventative measures but a PU/PI developed despite those measures, then the PU/PI many be considered unavoidable and the facility will not be subject to penalties.
AUTHORS' comments
- As stated previously in this topic, many clinicians and researchers believe that KTUs, SCALE, or TB-TTIs are not PUs/PIs and can be unavoidable as part of the dying process.[3][15]
- Those skin injuries occur as a result of skin failure due to the dying process or during multi-organ failure. Skin is the largest organ in the body, and like any other organ, skin can fail.[1][2]
- If clinicians document accordingly (i.e. why lesions are considered "unavoidable", findings that support the skin failure etiology), at least those lesions can be documented as unavoidable PUs/PIs
Relevant excerpts of the CMS' State Operations Manual: Guidance to Surveyors (F686) are shown below [16]:
Regarding PU/PI at the end-of-life
"It is important for surveyors to understand that when a facility has implemented individualized approaches for end-of-life care in accordance with the resident’s wishes, the development, continuation, or worsening of a PU/PI may be considered unavoidable. If the facility has implemented appropriate efforts to stabilize the resident’s condition (or indicted why the condition cannot or should not be stabilized) and has provided care to prevent or treat existing PU/PIs (including pertinent, routine, lesser aggressive approaches, such as, cleaning, turning, repositioning), the PU/PI may be considered unavoidable and consistent with regulatory requirements." [16]
Regarding KTUs
"Kennedy Terminal Ulcers are considered to be pressure ulcers that generally occur at the end of life. For concerns related to Kennedy Terminal Ulcers, refer to F686, §483.25(b) Pressure Ulcers." [16]
"The Kennedy Terminal Ulcer (KTU) The facility is responsible for accurately assessing and classifying an ulcer as a KTU or other type of PU/PI and demonstrate that appropriate preventative measures were in place to prevent non-KTU pressure ulcers. KTUs have certain characteristics which differentiate them from pressure ulcers such as the following [16]:
- KTUs appear suddenly and within hours;
- Usually appear on the sacrum and coccyx but can appear on the heels, posterior calf muscles, arms and elbows;
- Edges are usually irregular and are red, yellow, and black as the ulcer progresses, often described as pear, butterfly or horseshoe shaped; and
- Often appear as an abrasion, blister, or darkened area and may develop rapidly to a Stage 2, Stage 3, or Stage 4 injury"
CODING
ICD-10
Coding for Kennedy Terminal Ulcer (KTU)
- Currently, there is no ICD-10 code for KTU
- According to the CMS's State Operations Manual: Guidance to Surveyors (F686), KTU is considered a PU/PI. Thus, a KTU would be reported as (an unavoidable) PU/PI on the Minimum Data Set (MDS) [16]
Coding for skin failure
- L98.9: Disorder of the skin and subcutaneous tissue, unspecified [4]
CURATED ARTICLES