The DFU classification systems do not provide some of the details needed by medical coders for billing purposes. For instance, coders need to know the severity of tissue damage as described by the ICD-10. As a result, ulcer depth needs to be documented as: "limited to breakdown of skin", "with fat layer exposed", "with necrosis of muscle", etc. Otherwise the severity might be classified as “unspecified”, which will delay claim processing and reimbursement.[9]
The American Medical Association (AMA) recommends that ulcers such as DFU be properly documented for adequate code (ICD-10) assignment. That means that in addition to classifying the ulcer with one of the DFU classification systems, clinicians should clearly describe etiology, anatomical location with laterality and severity of tissue damage in a way that coders can easily match descriptions of existing ICD-10 codes to the medical record.
Tables 1A, 1B and 2 below correlate the Wagner and UT classification systems with the specific terminology medical coders need in order to correctly code the encounter.
WAGNER CLASSIFICATION
Table 1A. Wagner Classification for Diabetic Foot Ulcers [1][2][10] and terms for proper documentation on Medical Records
|
Image
|
Wagner Grade and description
|
Medical Records Documentation to facilitate ICD-10 coding
|
|

|
The GRADE 0 foot has intact skin. It has been found that this is the greatest protection to the diabetic foot. There may be bony deformities such as bunions, claw toes, depressed metatarsal heads and Charcot breakdown with bony prominences. There may be hyperkeratotic lesions around or under bony deformities
|
Conditions:
- Type 1, Type 2 or other type of diabetes (specify)
- peripheral neuropathy
- peripheral angiopathy
- neuropathic arthropathy
|
|

|
The Grade 1 foot has a superficial ulcer without penetration to deeper layers. The base may be necrotic or may be viable with early granulation tissue
|
Conditions:
- Type 1, Type 2 or other type of diabetes (specify)
- Diabetic Foot Ulcer
Ulcer location in foot:
- left or right foot
- heel or midfoot
- other part of the foot (specify)
Ulcer depth:
- limited to breakdown of skin
- with fat layer exposed
|
|

|
The Grade 2 foot has a lesion that is deeper and extends to the bone, ligament, tendon, joint capsule or deep fascia. There is yet no abscess or osteomyelitis
|
Conditions:
- Type 1, Type 2 or other type of diabetes (specify)
- Diabetic Foot Ulcer
Ulcer location in foot:
- left or right foot
- heel or midfoot
- other part of the foot (specify)
Ulcer depth:
- with necrosis of muscle
- with muscle involvement without evidence of necrosis
|
|

|
The Grade 3 foot has ulcer with deep abscess, osteitis or osteomyelitis, pyarthrosis, plantar space abscess, or infection of the tendon and tendon sheaths. The exact extent of the lesion is frequently difficult to determine from superficial examination (*) |
Conditions:
- Type 1, Type 2 or other type of diabetes (specify)
- Diabetic Foot Ulcer
Ulcer location in foot:
- left or right foot
- heel or midfoot
- other part of the foot (specify)
Ulcer depth:
- with necrosis of muscle
- with muscle involvement without evidence of necrosis
- with necrosis of bone
- with bone involvement without evidence of necrosis
Type of infection:
- cellulitis
- abscess
- osteomyelitis
|
|

|
The Grade 4 foot has some portion of the toes or forefoot that is gangrenous. Gangrene may be moist or dry |
Conditions:
- Diabetic peripheral angiopathy with gangrene
- Diabetic Foot Ulcer
Ulcer location in foot:
- left or right foot
- heel or midfoot
- other part of the foot (specify)
Ulcer depth:
|
|

|
A Grade 5 foot represents such complete involvement of gangrene that no foot healing or local procedure are possible. Amputation of the gangrenous area is indicated. |
Conditions:
- Diabetic peripheral angiopathy with gangrene
- Diabetic Foot Ulcer
Ulcer location in foot:
- left or right foot
- heel or midfoot and other part of the foot. Entire foot
Ulcer depth:
|
- Among other requirements listed on Medicare determinations, a diabetic foot ulcer needs to be classified as Wagner 3 or above to justify treatment with hyperbaric oxygen therapy. For details, refer to section 'Wagner Classification' in topic " Diabetic Foot Ulcer - Hyperbaric Oxygen Therapy".
- Diabetic foot infections may not display classic signs of soft tissue infection and nevertheless may have underlying osteomyelitis. Probe-to-bone test, serum inflammatory markers, imaging tests (e.g., X-rays, MRI) or bone biopsy are usually needed for diagnosis of osteomyelitis. For more on diagnosis of soft tissue infection and osteomyelitis refer to "Diabetic Foot Ulcer - Introduction and Assessment".
Quick Reference Tool
See the 'Quick Reference Tool: Diabetic Foot Ulcer - Wagner Classification System' below (Table 1B)
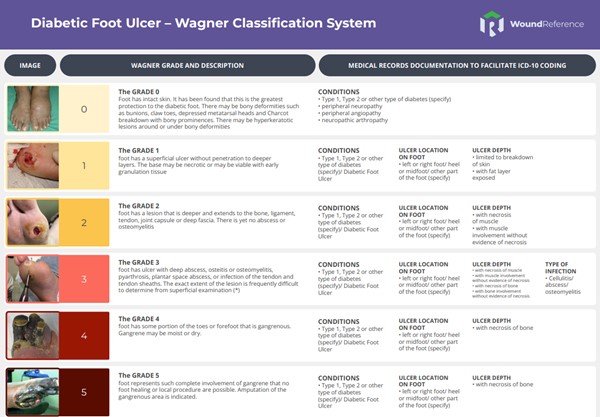
Table 1B. Quick Reference Tool: Diabetic Foot Ulcer - Wagner Classification System
UNIVERSITY OF TEXAS CLASSIFICATION
Table 2. University of Texas Classification for Diabetic Foot Ulcers [3] and terms for proper documentation on Medical Records
|
Grade/
Stage
|
Grade 0 |
Grade 1 |
Grade 2 |
Grade 3 |
Medical Records Documentation to facilitate ICD-10 coding |
| A |
Pre- or postulcerative, completely epithelialized
|
Superficial ulcer (partial or full thickness) not involving tendon, capsule, or bone
|
Tendon or capsular involvement without palpable bone
|
Ulcer probes to bone

|
- Type 1, Type 2 or other type of diabetes (specify)
|
| B |
With infection

|
With infection

|
With infection

|
With infection

|
- cellulitis
- abscess
- osteomyelitis
- location (foot, toe, left or right)
|
| C |
With ischemia

|
With ischemia

|
With ischemia

|
With ischemia
|
- diabetic peripheral angiopathy with or without gangrene
|
| D |
With infection and ischemia

|
With infection and ischemia

|
With infection and ischemia

|
With infection and ischemia

|
See B and C above |
|
*
|
Conditions:
- peripheral neuropathy
- neuropathic arthropathy
|
Conditions:
Ulcer location in foot:
- left or right foot
- heel or midfoot
- other part of the foot (specify)
Ulcer depth:
- limited to breakdown of skin
- with fat layer exposed
|
Conditions:
Ulcer location in foot:
- left or right foot
- heel or midfoot
- other part of the foot (specify)
Ulcer depth:
- with necrosis of muscle
- with muscle involvement without evidence of necrosis
|
Conditions:
Ulcer location in foot:
- left or right foot
- heel or midfoot
- other part of the foot (specify)
Ulcer depth:
- with necrosis of bone
- with bone involvement without evidence of necrosis
|
|
* Medical Records Documentation
INFECTIOUS DISEASES SOCIETY OF AMERICA (IDSA) CLASSIFICATION
Table 3. Classification of severity of diabetic foot infections, by the Infectious Diseases Society of America (IDSA) [4]
| CLINICAL CRITERIA |
GRADE/SEVERITY |
|
No clinical signs of infection
|
Grade 1/ uninfected
|
|
Local infection (skin and/or subcutaneous tissue), with at least two of the items below:
- Local swelling or induration
- Erythema > 0.5 cm and ≤2 cm around the ulcer. Excluded other causes of an inflammatory response of the skin (eg, trauma, gout, acute Charcot neuro-osteoarthropathy, fracture, thrombosis, venous stasis)around the wound
- Local tenderness or pain
- Local warmth
- Purulent discharge
|
Grade 2/ mild
|
|
Local infection (as described above) with erythema > 2 cm, or involving structures deeper than skin and subcutaneous tissues (eg, abscess, osteomyelitis, septic arthritis, fasciitis), and no systemic inflammatory response signs (as described below)
|
Grade 3/ moderate
|
|
Local infection (as described above) with the signs of systemic inflammatory response syndrome, as manifested by ≥2 of the following:
- Temperature > 38 °C or < 36 °C
- Heart rate > 90 beats/min
- Respiratory rate > 20 breaths/min or PaCO2 < 4.3 kPa (32 mmHg)
- White blood cell count > 12 000/mm3 or < 4000/mm3, or > 10% immature (band) forms
|
Grade 4/ severe
|
THE SOCIETY FOR VASCULAR SURGERY LOWER EXTREMITY THREATENED LIMB WOUND/ISCHEMIA/FOOT INFECTION (WIfI)
Table 4. The WIfI Classification System [5]: a) W=Wound, b) I=Ischemia, c) fI=Infection
Table 4.a W=Wound
| GRADE |
ULCER |
GANGRENE |
CLINICAL DESCRIPTION |
| 0 |
No ulcer |
No gangrene |
Ischemic rest pain (requires typical symptoms of ischemia grade 3); no wound. |
| 1 |
Mild:
Small, shallow ulcer(s) on distal leg
or foot; no exposed bone, unless limited to distal phalanx
|
No gangrene |
Minor tissue loss. Salvageable with simple digital amputation (1 or 2 digits) or skin coverage |
| 2 |
Moderate:
Deeper ulcer with exposed bone, joint or tendon; generally not involving the heel; shallow heel ulcer, without calcaneal involvement
|
Gangrenous changes limited to digits |
Major tissue loss salvageable with multiple (more than 3) digital amputations or standard TMA +/- skin coverage |
| 3 |
Severe:
Extensive, deep ulcer involving forefoot and/or midfoot; deep, full thickness heel ulcer +/- calcaneal involvement
|
Extensive gangrene involving forefoot and /or midfoot; full thickness
heel necrosis +/- calcaneal involvement |
Extensive tissue loss salvageable only with a complex foot reconstruction or nontraditional TMA (Chopart or Lisfranc);
flap coverage or complex wound management needed for large soft tissue defect
|
TMA: transmetatarsal amputation
Table 4.b: I=Ischemia
| GRADE |
ABI |
ANKLE SYSTOLIC PRESSURE |
TP, TcPO2 |
| 0 |
> or =0.80
|
>100 mmHg |
> or =60 mm Hg |
| 1 |
0.6-0.79 |
70-100 mmHg |
40-59 mmHg |
| 2 |
0.4-0.59 |
50-70 mmHg |
30-39 mmHg |
| 3 |
< or =0.39 |
<50 mmHg |
<30 mmHg |
ABI, Ankle-brachial index; PVR, pulse volume recording; SPP, skin perfusion pressure; TP, toe pressure; TcPO2, transcutaneous oximetry.
Hemodynamics/perfusion: Measure TP or TcPO2 if ABI incompressible (>1.3).
Patients with diabetes should have TP measurements. If arterial calcification precludes reliable ABI or TP measurements, ischemia should be documented by TcPO2, SPP, or PVR. If TP and ABI measurements result in different grades, TP will be the primary determinant of ischemia grade. Flat or minimally pulsatile forefoot PVR = grade 3.
Table 4.c. fI=Foot Infection
| CLINICAL MANIFESTATION OF INFECTION |
SVS WIfi |
IDSA/PEDIS
infection severity |
|
No symptoms or signs of infection
Local infection is defined by the presence of at least 2 of the following
items:
- Local swelling or induration
- Erythema >0.5 to < or=2 cm around the ulcer
- Local tenderness or pain
- Local warmth
- Purulent discharge (thick, opaque to white, or sanguineous secretion)
|
0 |
Uninfected |
Local infection involving only the skin and the subcutaneous tissue (without involvement of deeper tissues and without systemic signs as described below).
Exclude other causes of an inflammatory response of the skin (eg, trauma, gout, acute Charcot neuro-osteoarthropathy, fracture, thrombosis, venous stasis) |
1 |
Mild |
|
Local infection (as described above) with erythema >2 cm, or involving structures deeper than skin and subcutaneous tissues (eg, abscess, osteomyelitis, septic arthritis, fasciitis), and
No systemic inflammatory response signs (as described below)
|
2 |
Moderate |
|
Local infection (as described above) with the signs of systemic inflammatory response syndrome, as manifested by ≥2 of the following:
- Temperature > 38 °C or < 36 °C
- Heart rate > 90 beats/min
- Respiratory rate > 20 breaths/min or PaCO2 < 4.3 kPa (32 mmHg)
- White blood cell count > 12 000/mm3 or < 4000/mm3,or > 10% immature (band) forms
|
3 |
Severe |
PaCO2, Partial pressure of arterial carbon dioxide; SIRS, systemic inflammatory response syndrome.
Ischemia may complicate and increase the severity of any infection. Systemic infection may sometimes manifest with other clinical findings, such as hypotension, confusion, vomiting, or evidence of metabolic disturbances, such as acidosis, severe hyperglycemia, new-onset azotemia. From Lipsky et al. [4]
Key summary points for use of Society for Vascular Surgery Lower Extremity Threatened Limb (SVS WIfI) classification system
- The full system above is to be used for initial, baseline classification of all patients with ischemic rest pain or wounds within the spectrum of chronic lower limb ischemia when reporting outcomes, regardless of form of therapy. The system is not to be employed for patients with vasospastic and collagen vascular disease, vasculitis, Buerger’s disease, acute limb ischemia, or acute trauma (mangled extremity)
- Patients with and without diabetes mellitus should be differentiated into separate categories for subsequent outcomes analysis.
-
- Presence or absence of neuropathy should be noted when possible in patients with diabetes in long-term studies of wound healing, ulcer recurrence, and amputation, since the presence of neuropathy (loss of protective sensation and motor neuropathic deformity) influences recurrence rate
- In the Wound (W) classification, depth takes priority over size. Although WIfI recommends that a wound, if present, be measured, a shallow, 8-cm2 ulcer with no exposed tendon or bone would be classified as grade 1
- Toe pressures (TPs) are preferred for classification of ischemia (I) in patients with diabetes mellitus, since ABI is often falsely elevated. TcPO2, SPP, and flat forefoot PVRs are also acceptable alternatives if TP is unavailable. All reports of outcomes with or without revascularization therapy require measurement and classification of baseline perfusion.
- In reporting the outcomes of revascularization procedures, patients should be restaged after control of infection, if present, and/or after any debridement, if performed, prior to revascularization
-
- Group a patients: no infection within 30 days, or simple infection controlled with antibiotics alone
- Group b patients: had infection that required incision and drainage or debridement/partial amputation to control
FREQUENTLY ASKED QUESTIONS
What is the best classification system for DFU?
There is no single “best” classification system for DFU. Each system has advantages and limitations, and their use often depends on clinical goals, available resources, and regulatory requirements. However the WIfI system is the most comprehensive and modern, correlating with key clinical outcomes, while Wagner remains the most widely used for regulatory and reimbursement purposes.
Why is Wagner classification still used today?
The Wagner classification is still used today because, despite its limitations, it remains the system required by Medicare and other payors in the United States to determine eligibility for hyperbaric oxygen therapy (HBOT) in patients with diabetic foot ulcers (DFUs). Specifically, Medicare coverage for HBOT requires that a DFU be classified as Wagner Grade 3 or higher and that it has failed to respond to at least 30 days of standard wound care. Additionally, the Wagner system is well established and widely recognized, providing a simple, visual method to describe the depth and severity of diabetic foot ulcers. Its continued use is also tied to documentation and coding requirements—clinicians must record the Wagner grade to justify medical necessity and facilitate proper ICD-10 coding and reimbursement.
What characterizes a Wagner Grade 3 DFU?
A Wagner Grade 3 diabetic foot ulcer (DFU) is characterized by deep tissue involvement with infection. Specifically, it includes:
- Ulcer with deep abscess, osteitis or osteomyelitis, pyarthrosis, plantar space abscess, or infection of the tendon and tendon sheaths.
- The lesion extends into deeper structures such as bone, joint, or tendon, and the exact extent of the lesion is often difficult to determine from superficial examination.
- It represents a neuropathic ulcer complicated by infection, corresponding to University of Texas grades IIB, IID, IIIB, or IIID.
Clinically, these ulcers are infected but not yet gangrenous (gangrene would correspond to Wagner Grades 4 or 5).
In summary, a Wagner Grade 3 DFU involves deep infection with abscess or bone involvement (osteomyelitis) and marks the threshold at which hyperbaric oxygen therapy (HBOT) may be considered if the ulcer fails to heal after 30 days of standard wound care.
Can I backstage Wagner classification?
No, you should not backstage or reverse the classification of an ulcer using the Wagner classification. According to the provided context, while Wagner’s original article allowed for bidirectional progression and regression between grades (except Grade 5), in clinical documentation practice, “reverse grading” is not commonly done. The context explicitly states that if a diabetic foot ulcer (DFU) originally identified as a Wagner Grade 3 shows improvement, clinicians typically document the healing progress (e.g., reduced size, depth, and infection) rather than formally reclassifying it to a lower grade. It would be referred to as a “healing Wagner Grade 3” DFU instead. Therefore, although the original system conceptually allowed regression, current documentation standards do not support backstaging or reverse grading of ulcers.
The implications of backstaging include:
- Documentation inconsistency: It may obscure the ulcer’s original severity, making it harder to track clinical progress accurately.
- Insurance and reimbursement issues: Many third-party payors, including Medicare, tie coverage (e.g., for hyperbaric oxygen therapy) to the Wagner grade. Reversing the grade could affect eligibility or justification for treatments.
- Loss of clinical context: The original grade helps clinicians understand the ulcer’s initial complications and guides treatment decisions. Changing it could misrepresent the patient’s clinical course.
Why does documentation still need ICD-10 severity terminology in addition to DFU classification?
Because the DFU classification systems alone do not provide all the details required by medical coders for accurate billing and reimbursement. According to the context, coders must know the severity of tissue damage as described by ICD-10 - specifically whether the ulcer is limited to breakdown of skin, has fat layer exposed, has necrosis of muscle, or has necrosis of bone. The DFU classification systems (such as Wagner or University of Texas) describe ulcer depth and infection but do not always align directly with ICD-10 terminology. Therefore, clinicians must document both the DFU classification and the ICD-10 severity descriptors so that coders can correctly match the medical record to the appropriate ICD-10 code. Without this additional ICD-10-specific documentation, the ulcer’s severity might be classified as “unspecified,” which can delay claim processing and reimbursement.