We would like to start this blog series by emphasizing that we are not recommending HBOT for off-label indications. However, the use of HBOT for certain off-label conditions may be supported by some evidence, as described by case reports, case series, or small randomized controlled trials (RCTs). In this blog series we will provide an overview of off-label indications for HBOT, and review existing evidence for several conditions.
We are going to start with an overview of off-label HBOT. To do so, we must define the boundaries of 'on' and 'off' label HBOT use.

What is an off-label HBOT indication?
For these purposes, we are assuming that the reader lives/resides in the USA. This may not apply to practitioners outside of the USA. In simple terms, only diagnoses that are found in the Undersea and Hyperbaric Medical Society (UHMS) 'approved' list are considered on-label. Using HBOT for any other use is considered 'off-label.'
UHMS Approved Indications
Why is HBOT vulnerable to ‘off-label’ use?
A good colleague once said, "Desperate patients will do/try anything in order to improve their health."
An anecdote so that the reader appreciates the dilemma: I recall being at my desk during a hyperbaric treatment in progress. My nurse (who could answer 95% of questions about HBOT) tells me that she has a potential patient on the line with some questions. Cue the ethereal, dramatic, and meloncholy suspenseful music. When I answered the question, the distraught mother of an adult daughter with Multiple Sclerosis (MS) comes on the line. "I've read where HBOT can stop MS. When can you start treating my daughter?"
I spent the next 10 minutes talking to her about all of the 'evidence' about MS and HBOT. In my opinion, there is a paucity of evidence regarding any benefit whatsoever with HBOT and MS. I told her that we were a hospital-based clinic and could only treat 'on-label' indications for HBOT. We could not provide HBOT for MS, and there were no other "hyperbaric facilities" in our area who treated 'off-label' for HBOT.
The next response was one that I was not prepared for ... and mother let loose a string of words. What I remember was, "You are heartless! If this was your daughter what would you do?" I chose to respond by recognizing how painful this diagnosis was to mother and how difficult it would be for her daughter. I also told her that I didn't have a daughter, so I couldn't put myself in her position. But, even if I did have a daughter with that diagnosis, I would never put her into the hyperbaric chamber. There is no data to suggest that there would be any predictable positive outcome for any of the symptoms of MS. Hence, I admit to being heartless, even to my own family.
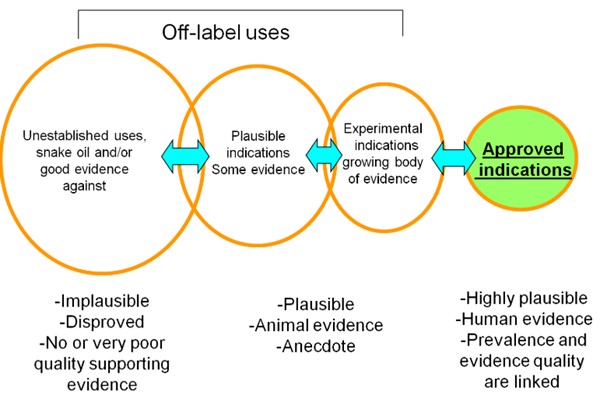
You can see that well-meaning parents/patients, who have been given a particularly bad diagnosis ... like MS, autism, chronic fatigue syndrome, and others ... will do anything to better the condition of self or loved ones. Unfortunately, these diagnoses fit into a category that we will describe below. This category pulls together diagnoses that are implausible, disproved, or have no quality evidence supporting use of HBOT.
In this blog series, we will not talk about any implausible diseases for which HBOT may/may not be in current use. Instead, we will focus on several conditions that have case descriptions, small case series, and/or small randomized controlled trials. These diagnoses may not have enough evidence to be a UHMS-approved condition, but they have enough scientific and physiological basis to be considered useful with hyperbaric medicine.
Off-label uses in HBOT
Types of off-label uses
Off-Label, Not Plausible:
Note that there may be many anecdotal or testimonial publications for the following diagnoses. However, there is no (or little) literature evidence to support HBOT for following conditions. Our position may change for some of these diagnoses in the future, but the science is not present now.
- Anoxic Brain Injury
- Cerebral Palsy
- Multiple Sclerosis
- Parkinson's Disease
- Chronic Fatigue Syndrome
- Lyme Disease
- Near Drowning
- Autism
- Lupus
Off-Label, Less Plausible
- Stroke
- Spinal cord injuries
- Age-Related Macular Degeneration
- Traumatic Brain Injury
Off-Label, Plausible
- Altitude sickness
- Avascular necrosis
- Bisphosphonate Osteonecrosis of the mandible (BRON)
- Brown Recluse/ Black Widow bites
- Complex Regional Pain Syndrome
- Crohn’s Disease
- Interstitial Cystitis
- Frostbite
- Livedoid Vasculopathy
- Tumor sensitization for certain cancers (immediately prior to radiation treatments)
- Elite athlete injuries
- Infertility
Considerations when planning to treat off-label indications
If your facility is not a hospital clinic, and is considered a freestanding clinic, your physician and/or clinical staff may be able to treat any indication for HBOT that they desire. However, if you are part of a hospital clinic, such is frequently not the case. Hospital clinics must maintain a standard that includes not treating off-label. (To do otherwise, puts at risk the ability to treat Medicare/Medicaid patients.)
However, there are exceptions to this. There are occasions where the medical staff may be persuaded to treat a plausible, but off-label condition. We have seen some hospital facilities do so on rare occasion, especially where the outcome without HBOT may be a total colectomy (for treatment refractory Inflammatory Bowel Disease) or some other devastating outcome. These are rare conditions where the HBOT unit frequently approaches the hospital IRB asking for an exception, or they may approach the Chief Medical Officer or Ethics Committee with this request. Unless you are set up to do trial research with a specific protocol, your IRB will likely deny off-label HBOT.
In addition, your facility may not be able to bill for your services since this is an off-label condition and you cannot bill insurance. While we try not to be heartless, there are conditions that we feel have enough scientific evidence to discuss in this blog. So, off we go!
Coming up next...
We plan to focus this blog series on 3 conditions that are off-label and have plausible literature evidence for improvement after HBOT
Resources
About the Authors
Eugene Worth, MD, M.Ed., FABA, ABPM/UHM
Eugene R. Worth, MD, M.Ed., FABA, ABPM/UHM is a board-certified anesthesiologist specialized in cardiac and vascular anesthesia. He is a wound care and hyperbaric physician, and Advisor/Editor of WoundReference, Inc., a clinical and reimbursement decision support platform for wound care and hyperbaric clinicians. Dr Worth is the recipient of a number of awards and distinctions in undersea and hyperbaric medicine. He has been a physician surveyor for the UHMS Accreditation Team and a reviewer for the journal, Undersea and Hyperbaric Medicine. He is a physician member of the UHMS Safety Committee. He has written multiple publications and book chapters for topics in hyperbaric medicine.