ABSTRACT
Telehealth has become an important tool in the management of chronic wounds, and its use in wound care is supported by available evidence. [1]
Telehealth modalities
See definitions and details on:
- Store-and-forward (asynchronous)
- Real-time televideo conferencing (synchronous)
- Remote monitoring
- Mobile health (mHealth)
Types of telehealth for reimbursement purposes
See definitions and details on:
- Centers for Medicare and Medicaid Services (CMS) Telehealth Visits
- Brief communication technology-based service (e.g. virtual check-in),
- Remote evaluation of recorded video and/or images (e.g. store-and-forward)
- Interprofessional internet consultation
- Remote monitoring
Indications:
Potential uses of telehealth include [2] :
- Delivery of wound care advice from a remote wound specialist to a non-wound care clinician treating a patient with chronic wound in the community, at a post acute facility, or at the patient’s home
- Wound care specialist seeking evaluation by other specialists (e.g., infectious disease, endocrinology, etc.)
- Wound care specialist providing virtual follow-up care to patients who are not able to attend an in-person visit (e.g., to minimize the spread of infectious diseases)
- Virtual triage of any new or existing patients in order to direct patients to the appropriate clinician and avoid unnecessary referrals
- Virtual follow up of a established patient who is going out of town for vacation, or for an established patient who is out of town and needs urgent advice
- Provision of specialized wound care for patients with COVID-19 in the hospital/intensive care unit/other settings from outside the patient’s room, limiting healthcare workers’ exposure to the virus
Situations in which telehealth is not appropriate:
- Technological barriers (e.g., lack of Internet or cell phone reception, lack of a device that is capable of televisits)
- Patients with suspected critical/severe conditions should receive a thorough in-person evaluation
- Patients or clinicians who are unwilling or unable to conduct a virtual visit should receive an in-person evaluation
- Patient requiring procedures (i.e debridement, skin substitutes etc )
- Other factors may eliminate the telehealth option. See section “How to Determine if Telehealth is Suitable for a Patient”
Evidence and Recommendations:
See evidence on the use telehealth for the populations below:
- Patients with chronic wounds under the care of non-wound care clinicians
- Patients with DFUs who are not in critical/severe conditions and live far from a wound clinic, or for whom in-person visits are not recommended or convenient
- Patients with chronic wounds in guarded or stable conditions
Best Practices and Tips
See summary of best practices and tips on:
- How to Get Started With Telehealth
- How to Choose and Tailor Telehealth Modalities to Your Needs
- How to Choose a Telehealth Software for Wound Care
- How to Determine if Telehealth is Suitable for a Patient
- How to Prepare for a Successful Virtual Encounter
- How to Assess and Measure Wounds
- How to Overcome Technical Obstacles
- How to Meet Documentation Requirements
In 2020, the U.S. experienced rapid telehealth adoption, with an 11,718% increase in services among Medicare beneficiaries from March to April.[3] Although the magnitude of this uptake is largely attributable to the need for remote care delivery during the COVID-19 pandemic, telehealth is not new, with its first use dating to the 19th century.[4]
An analysis of 950 studies published prior to the pandemic concluded that telehealth is beneficial for specific uses and patient populations.[5] In certain instances, the use of telehealth produces equal or better results than in-person care only, with improved intermediate clinical outcomes and patient satisfaction.[1] Chronic wound management is one of the specific uses for which evidence supports use of telehealth.[1]
The 2020 pandemic brought regulatory and reimbursement flexibilities that provided an opportunity for clinicians in the United States to implement telehealth in the real world and address outstanding questions on how to offer telehealth (rather than whether to offer it).
This topic summarizes evidence and provides a collection of best practices on the use of telehealth in wound care.
Definitions
Relevance
The use of telehealth in wound care offers health and economic benefits for patients, providers, and institutions (Figure 2):
- With respect to clinical outcomes, the use of telehealth services in specific cases has been shown to result in faster healing rates [12][13],[14], fewer adverse events [13], and decreased risk of amputation.[15][16]
- From the patient perspective, telehealth offers the benefits of reduced wait times [8], greater access to specialty care [8], and facilitated delivery of education materials. A study found that a 12-week educational intervention improved foot self-care behavior among patients with diabetic retinopathy.[17][18]
- From the provider and institutional perspective, the use of telehealth presents important additional advantages:
-
- Greater scheduling flexibility for providers: providers can conduct virtual visits from home, which opens up possibilities for scheduling virtual visits on evenings or weekends.[19][20]
- Ability for clinicians to more easily provide follow-up care to patients
- Opportunity to fulfill CMS quality measures requirements (e.g. expanded practice access and better care coordination). See section ‘CMS Quality Measures’ below
- Telehealth can help providers ensure continuity of care and avoid lost income when an in-person encounter is not possible or recommended (e.g., lack of transportation to the clinic, immunocompromised patients amidst a pandemic, etc),
- A hybrid approach that employs a combination of in-person care and adjunctive telehealth may translate into 30% cost savings to the institution when compared to an in-person only model.[21]
The U.S. healthcare spending is projected to continue to shift towards telehealth post-COVID [22], which affords wound care patients and clinicians the opportunity to realize these health and economic benefits moving forward (Figure 2). 
Figure 2. Telehealth adoption, benefits and growth [23][13][12][21][22]
Telehealth Modalities
Telehealth modalities are generally classified as [24][25][26] :
- Store-and-forward (asynchronous): e.g. digital photographs and clinical data sent over the internet to a wound care specialist, who analyzes the data, and sends back written recommendations
- Real-time televideo conferencing (synchronous): e.g. live interaction/communication with a wound care specialist via a webcam
- Remote monitoring: e.g. a provider continually monitors vital signs, glucose, etc. of a patient who is at home or remote care facility
- Mobile health (mHealth): health care and public health information provided through mobile device applications with the goal of improving health services and outcomes [27]
Types of Telehealth According to CMS and Private Insurers
In the U.S., CMS and private insurers generally classify virtual services as [28][29]:
- CMS Telehealth Visits
- Brief communication technology-based service (e.g. virtual check-in),
- Remote evaluation of recorded video and/or images (e.g. store-and-forward)
- Interprofessional internet consultation
- Remote monitoring
Table 1 below summarizes the telehealth modalities covered by CMS.
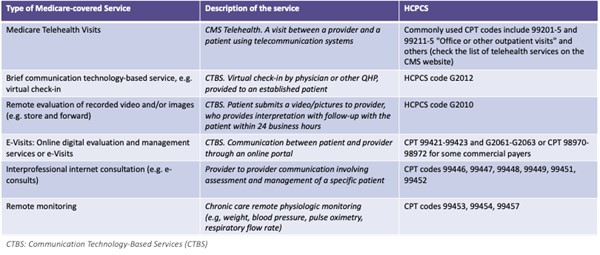
Table 1. CMS-billable Virtual Services [28][30][29]
Indications and Contraindications for Telehealth
Not all patients are suitable for telehealth consultations. Therefore, it is important to develop and implement a wound care triage system to identify which patients are candidates for virtual services, which patients require in-person evaluation, or which patients would benefit from a combination of services.
Two examples of telehealth triaging models are:
- Virtual-First Triaging [31]: NHS England and NHS Improvement developed the “Total Digital Triage” model in order to reduce avoidable risk of infection for both patients and providers during the COVID-19 pandemic. In this model, institutions utilize an online consultation system to asynchronously collect a patient’s history, symptoms, and relevant images. A patient calls or submits an inquiry through the practice website, administrative staff filters and directs queries to an appropriate clinician, and the clinician responds to the patient using the most suitable method for their needs (i.e. online, phone, video, or face-to-face).

Figure 3. Total Digital Triage model [31]
- Status-Dependent Triaging Preventing hospitalizations in an overburdened healthcare system, reducing amputation and death in people with diabetes. | Rogers LC, Lavery LA, Joseph WS, Armstrong DG et al. | 2020" target="_blank">[32]: Rogers’ “Pandemic Diabetic Foot Triage System” recommends that providers determine appropriateness of telehealth based on the classification of patients’ conditions as critical, serious, guarded, or stable (Figure 4). Specifically:
- Patients with critical or serious conditions should be seen in hospitals or outpatient clinics,
- Patients with guarded conditions (i.e. improving foot ulcer, inactive Charcot foot, or simple venous leg ulcer) can be treated using a mixed model of outpatient, home, and telehealth services.
- Patients with stable conditions (i.e. recently healed foot ulcer, inactive Charcot foot in stable footwear, healed amputation, or diabetic foot ulcer in remission) may benefit from the sole use of telehealth.

Figure 4. Status-dependent triaging Preventing hospitalizations in an overburdened healthcare system, reducing amputation and death in people with diabetes. | Rogers LC, Lavery LA, Joseph WS, Armstrong DG et al. | 2020" target="_blank">[32]
Indications
Potential uses of telehealth include [2]:
- Delivery of wound care advice from a remote wound specialist to a non-wound care clinician treating a patient with chronic wound in the community, post acute facility or at the patient’s home
- Wound care specialist seeking evaluation by other specialists (e.g. infectious disease, endocrinology, etc)
- Wound care specialist providing virtual follow up care to patients who are not allowed to complete an in-person visit (e.g. to minimize the spread of infectious diseases)
- Virtual triage of any new or existing patients, to direct patient to the appropriate clinician and avoid unnecessary referrals
- Virtual follow up of a established patient who is going out of town for vacation, or for an established patient who is out of town and needs urgent advice
- Provision of specialized wound care for patients with COVID-19 in the hospital/intensive care unit from outside the patient’s room, limiting healthcare workers’ exposure to the virus
Situations in which telehealth is not appropriate
Potential limitations of telehealth include [2]:
- Technological barriers (e.g., lack of internet or cell phone reception, lack of devices that are capable of televisits)
- Patients with suspected critical or severe conditions should receive a thorough evaluation in-person
- Patients or clinicians who are unwilling or unable to conduct a virtual visit
- Other factors that may eliminate the telehealth option. See section ‘How to Determine if Telehealth is Suitable for a Patient’
- Patient requiring procedures (i.e debridement, skin substitutes etc )
EVIDENCE AND RECOMMENDATIONS
Telehealth Services Between Wound Care Specialists and Non-Wound Care Clinicians
- 2BFor patients with chronic wounds under in-person care of non-wound care clinicians, we suggest that non-wound care clinicians consider receiving advice from a remote wound care specialist via telehealth, in order to improve wound healing outcomes and decrease amputation rates.(Grade 2B).
- Rationale: Expert advice delivered to non-wound care clinicians via telehealth (i.e., store-and-forward and/or real time video conferencing) has been shown to improve wound healing outcomes (i.e, wound healing rate, amputation rate) compared to care by non-wound care clinicians alone, as evidenced by moderate certainty evidence derived from several randomized controlled trials (RCTs).[8][12][13][14][15]
- So far, evidence is concentrated on telehealth between a remote expert clinician and a non-wound care clinician treating a patient (for instance, a treating clinician submits clinical information along with images of a patient’s wounds to a remote wound care specialist, who in turn provides wound care recommendations to the treating clinician). Current literature lacks RCTs that focus solely on direct telehealth services between clinicians and patients.
- From a patient perspective, patients have reported appreciation for the greater access to specialized care and savings in time, costs, and time off work that traveling for care would require.[8]
- Use of resources: compared to in-person visits, studies report lower costs with telehealth. In most cases, savings are attributable to reductions in transfers or less transportation.[8]
- 2BFor patients with lower extremity ulcers (e.g. DFUs) in guarded or stable conditions, who live far from a wound clinic or for whom an in-person visit is not recommended, wound care specialists might opt to provide follow-up care via telehealth as an alternative to the standard of care (i.e. in-person visits at the wound clinic) (Grade 2B).
- Rationale: There is moderate certainty evidence supporting follow up of patients with more superficial DFUs in the community, where community clinicians provide care under weekly supervision of a remote wound care specialist. It has been shown that such an arrangement leads to similar healing outcomes and quality of life as the standard of care, in which patients are followed up directly by wound specialists at a wound clinic.[33][16][34]
- This option is particularly attractive to patients who live far from wound clinics, or for whom in-person visits to the clinic/hospital are not recommended or convenient. Furthermore, studies have shown that telemedicine may significantly improve patient engagement and quality of care.[34]
Telehealth Services Between Wound Care Specialists and Patients
- 2CFor patients with chronic wounds in guarded or stable conditions, we suggest a hybrid model of telehealth combined with in-person visits to promote wound healing and detect potential complications, as opposed to in-person visits only (Grade 2C).
-
- Rationale: Current literature lacks RCTs assessing telehealth interventions between wound care clinicians and patients at home; so far RCTs have focused on telehealth between treating non-wound care clinicians and remote wound care specialists. However, the COVID-19 pandemic created the need for wound clinicians to schedule virtual visits directly with patients at their homes, in an effort to minimize spread of the virus. As a result, several recent cases reported successful management of chronic wounds via telehealth between providers and patients.[35][36]
- It is important for clinicians to identify what constitutes a good balance between in-person and telehealth care. Factors contributing to successful virtual visits include patient selection (not all are good candidates for telehealth), availability of family members or caregivers to assist with dressing changes, wound measurement, technical and connectivity difficulties, etc, and ease of use of the telehealth platform.[35][36][37]
- From a patient’s perspective, studies have reported a high level of satisfaction with telehealth interventions, due to convenience, increased access to care, decreased transportation costs.[37]
- Use of resources: CMS and many private insurers continue to provide widespread coverage to telehealth services during the pandemic. Several telehealth modalities will continue to be covered after the public health emergency ends. See topic “Reimbursement for Telemedicine Services in Wound Care”. A cost analysis study indicated that a hybrid model with a combination of in-person and telehealth visits can be less costly to the wound care institution when compared to an in-person only model.[21]
BEST PRACTICES AND TIPS
The best practices and tips in this section are specific to telehealth in wound care and were compiled from multiple sources, including publications, webinars, and expert opinions (See Infographic)
Infographic: Telehealth in Wound Care - Best Practices and Tips for Success (click to enlarge)
How to Get Started with Telehealth
- Ensure that your malpractice insurance covers telehealth services, especially across state lines, and provide your carrier with an effective date.Preventing hospitalizations in an overburdened healthcare system, reducing amputation and death in people with diabetes. | Rogers LC, Lavery LA, Joseph WS, Armstrong DG et al. | 2020" target="_blank" style="background-color: rgb(255, 255, 255);">[32][38][39]
- Review State Practice Acts.[38]
- Conduct an early meeting with your team to identify:
-
- Potential barriers [38]
- Patient demographic limitations (e.g., communication barriers, access to technology) [19][38]
- Ways to cultivate a positive patient experience, which should be a top priority when considering telehealth implementation [38]
- Nursing staff needs [19]
- Insurers’ coverage determinations related to telehealth; documentation and billing requirements
- Coding updates in the chargemaster, needed for proper billing of telehealth services
- Information technology (IT) needs (e.g., technology risk assessment, minimum requirements, etc)
- Telehealth modalities that will meet your needs. See the “How to Choose and Tailor Telehealth Modalities to your Needs” section below.
- Understand your electronic health record system (EHR) workflow and how telehealth can be integrated into the existing EHR workflow
-
- Some EHRs have telehealth capabilities. Generic EHR telehealth solutions may be sufficient for clinicians who do not need to evaluate patients with wounds. Specialized solutions might be desirable for specific needs. For a list of telehealth capabilities that are ideal for patients with wounds see the “How to Choose a Telehealth Software” section.
- If you choose to utilize an external vendor, execute a Business Associate Agreement (BAA) and obtain evaluation of your contract.[39]
- Prepare for implementation:
-
- Identify workflows tailored to the practice’s needs.[39] See workflows in the “Telehealth Modalities” section above.
- Create professional remote visit templates with smart phrases to standardize documentation for patient care and billing.[35]
- Incorporate a triage pathway to determine which patients are appropriate for telehealth.[39]
- Begin training sessions:
-
- Prior to beginning training sessions, ensure that workflow integration is in place.[38]
- To ensure a seamless experience and assist in workflow memorization, conduct multiple training sessions, manually rehearse steps, and incorporate clinician feedback.[38]
Figure 5. Summarizes the points above.
Figure 5. How to Get Started with Telehealth Preventing hospitalizations in an overburdened healthcare system, reducing amputation and death in people with diabetes. | Rogers LC, Lavery LA, Joseph WS, Armstrong DG et al. | 2020" target="_blank">[32][39][19][35]
How to Choose and Tailor Telehealth Modalities to Your Needs
- Telehealth modalities include real-time audio and video, store-and-forward, remote monitoring, etc. See the “Telehealth Modalities” section above.
- To identify the telehealth modalities that fit your needs, refer to the “The Wound Telemedicine Wizard” algorithm.
How to Choose a Telehealth Software for Wound Care
- Key characteristics of an optimal telehealth software may include:
-
- Secure, encrypted, and HIPAA-compliant [35][39][40]
- Easy-to-use [35][40]
- Interoperable [40]
- Cost-efficient [40]
- Accessible from desktop computers, tablets, and smartphones [35]
- Patient-centered [41]
-
- This is essential for individualization, fostering greater autonomy in the healing process, and promoting telehealth adoption.[41]
- Compliant with the Open Notes Provision of the 21st Century Cures Act [41]
- Key features of an optimal telehealth software may include:
-
- Ability for mobile device users to switch from the front to the rear-facing camera in order to show their wound to a remote provider during a video visit [41]
- A portal that allows patients to request consultations, submit photos, access medical history, and receive educational materials [41]
- Ability for patients/requesting clinicians to receive video visit links via SMS and/or email [41]
- Provision of real-time instructional materials for patients (e.g., how-to video tours) [41]
- Integration with clinic scheduling software [38]
- Documentation capabilities:
-
- Photo and wound documentation [40]
- Automatic time-tracking for CPT code selection [38]
- Smart/dot phrases with predefined, modifiable snippets, which allow for standardization and time saving [35]
- EMR workflow integration, which enables clinicians to link patients’ photos in the hospital information system and encourages providers to utilize the technology [19][40]
- Patient progress management to view patient’s development over time [40]
- Ability to obtain a second opinion from a colleague [40]
Figure 6 summarizes the points above.
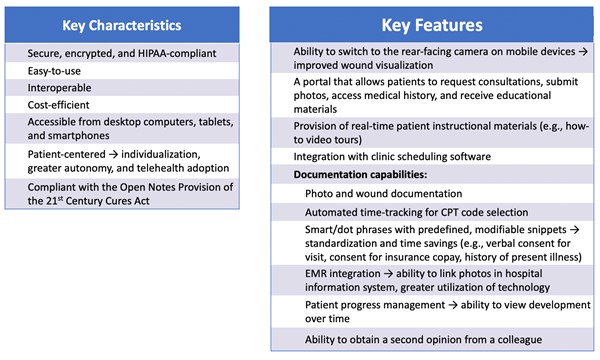
Figure 6. How to Choose a Telehealth Software for Wound Care [39][19][35][40]
How to Determine if Telehealth is Suitable for a Patient
- Screen patients during in-person appointments and identify patient-level factors that may eliminate the telehealth option.[38]
-
- Does the patient have a smartphone, computer, or tablet? [38]
- Does the patient have a strong Internet connection? [38]
- Does the patient have someone to assist you during the visit? [38]
- Does the patient have experience using technology? [38][40]
- Does the patient have visual or hearing impairment? [38]
- Does the patient have difficulty with manual dexterity? [38]
- Does the patient display a favorable attitude toward technology and telehealth visits? [38][40]
- Is the patient concerned about their condition? [38]
- Do you have a positive working relationship with the patient? [38]
- Establish the goal of each visit and identify clinical factors that may eliminate the telehealth option.
-
- Do you need to communicate bad news or test results? [38]
- Do you need to obtain diagnostics (e.g., collect wound culture)? [38]
- Are you or a family member worried about the patient? [38]
- Does the complexity of the patient’s condition necessitate an in-person appointment? [38]
-
- For example, while some pressure ulcers and injuries are suitable to be treated via telehealth, complex and deep wounds such as a Wagner 3 diabetic foot ulcer require in-person assessment.[38]
- Do you feel the need to “trust but verify” to ensure that the patient is telling the truth? [38]
- Will a telehealth visit satisfy your paperwork requirements? [38]
Figure 7 summarizes the points above.
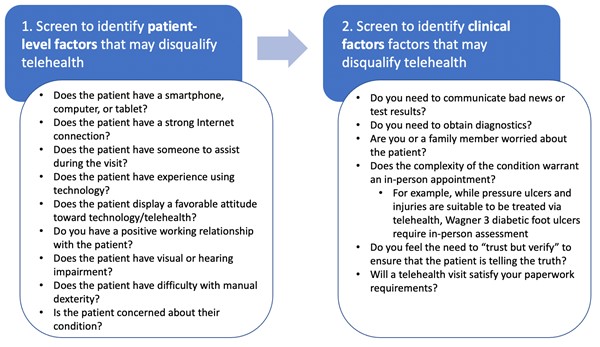
Figure 7. How to Determine if Telehealth is Suitable for a Patient
How to Prepare for a Successful Virtual Encounter
- Nursing/administrative staff perspective
- During the in-person visit:
-
- Educate patients on the telehealth option.[38]
- Demonstrate how to join a televisit.[38]
- Before the telehealth visit:
-
- Contact patients to determine device suitability, assess Internet connection, and encourage patient portal activation.[35]
- Allow for a similar visit length as in-person appointments when scheduling.[38]
- Communicate to ensure that the visit time accommodates both the provider and facilitating clinician’s schedule.[19][41]
-
- Oftentimes, practices may prefer to schedule telehealth visits after the in-person appointments
- For home health patients, clinicians may consider scheduling telehealth visits at the time of the home visit.[39]
-
- NOTE: If scheduling telehealth visits at the time of the home visit, ensure reimbursement requirements for both telehealth and the home health episode of care are met. See blog post “Reimbursement for Telemedicine Services in Wound Care”.
- Prepare the encounter and add documentation templates.[38]
- During the telehealth visit:
-
- Complete rooming as if the patient was on site (e.g., guide the patient so that the wound is exposed).[38]
- Document using a standardized template to establish efficient workflow.[38]
Figure 8 illustrates the points above.
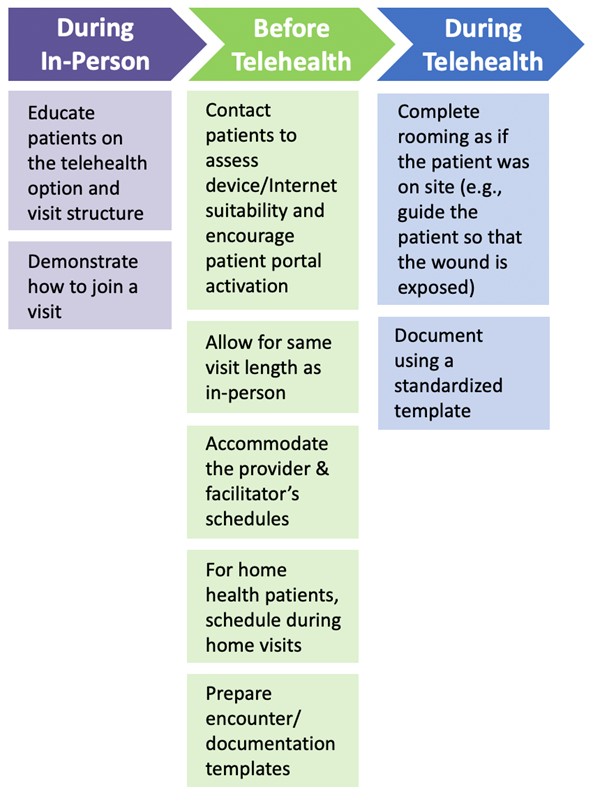
Figure 8. How to Prepare for a Successful Virtual Encounter - Nursing/administrative staff perspective
- Prior to implementing telehealth visits, develop relationships with facilitating clinicians and understand what resources are available at their organization (i.e., staff, dressings, adjunctive therapies).[38] See Figure 9.
- Before a telehealth visit with a patient:
-
- Explain and rehearse steps with the patient [38]
- Review paperwork and patient history [41]
- Communicate with facilitating clinicians to identify key topics of discussion [41]
- Before a telehealth visit with a facilitating clinician (e.g. home health, skilled nursing facility):
-
- Set a date and time [38]
- Obtain necessary information prior to the visit to ensure efficiency (e.g., facilitating clinician may be able to send pictures of the wound ahead of time) [38]
- Expect a learning curve [38]

Figure 9. How to Prepare for a Successful Virtual Encounter - Provider' Perspective
- Facilitating clinician perspective
- In home health settings (Figure 10):
- Ensure that telehealth visits are on the patient’s schedule.[41]
- Arrive early to measure the wound, upload images, and take vital signs.[41]
- Ask a family member or aide to assist with positioning the phone and working with the patient.[41]

Figure 10. How to Prepare for a Successful Virtual Encounter - Facilitating Clinician's Perspective
- Provide patients with instructional materials that outline tips for a successful visit.[41] See topic “Patient Education - Successful TeleVisits for People with Wounds”
- Encourage patients to attend telehealth visits with a technically-proficient family member or aide who can assist with submitting images and focusing the camera.[38]
Figure 11 illustrates the points above.

Figure 11. How to Prepare for a Successful Virtual Encounter - Patient's Perspective
How to Assess and Measure Wounds
- Ask the patient to place a device with measurements in centimeters near the wound to provide dimension.[19] Alternatively, if available, may consider an automated app to track wound assessment and measurement.[38]
- Refer to images of the wound submitted in advance or captured during the visit.
-
- TIP: The presence of a technically-proficient family member or aide is helpful in both uploading images and stabilizing the mobile device during the visit.[38]
- TIP: Capturing a quality image is a team effort requiring collaboration and patience from both the provider and patient.[38]
- If assessment of the wound is challenging due to blurred video/photo, use terms such as “appears to” when documenting characteristics of the wound, as it may be difficult to discern details with confidence (other than if the wound is of partial or full thickness).[38]
Figure 12 illustrates the points above.
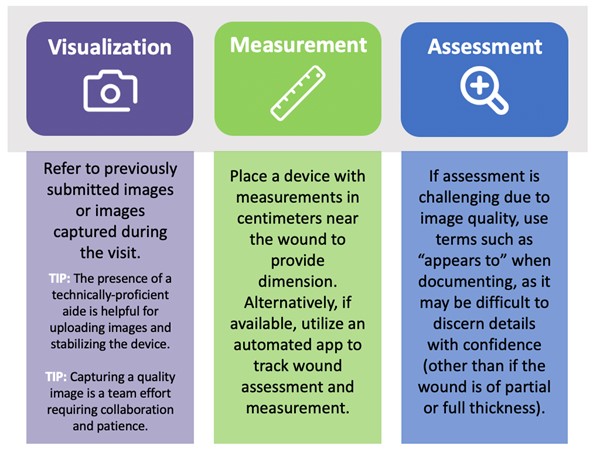
Figure 12. How to Assess and Measure Wounds
How to Overcome Technical Obstacles
- Implement checklists to identify potential limitations and ensure Internet connectivity is stable.[38]
- Troubleshoot in advance and conduct pre-call tests with collaborating organizations to ensure that operating systems, browsers, and mobile devices are suitable.[38]
Figure 13 illustrates the points above.
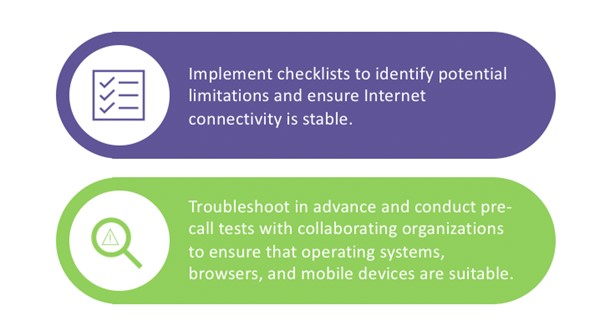
Figure 13. How to Overcome Technical Obstacles
How to Meet Documentation Requirements
- Ensure that documentation meets specific payor requirements.[38]
- Document as if you are being audited.[38]
- Recognize that the documentation requirement for telehealth is the same as for in-person visits.[39]
- To streamline telehealth visits in home health settings, develop a checklist of essential, EMR-specific information for the nurse to collect.[41]
Figure 14 illustrates the points above.
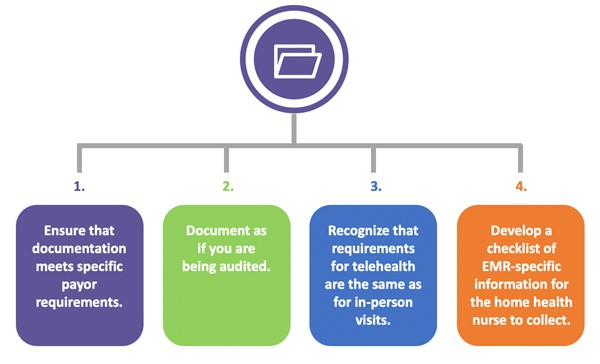
Figure 14. How to Meet Documentation Requirements [39]
PATIENT EDUCATION
- The delivery of patient education materials is a critical component in the provision of telehealth services, as it empowers patients to achieve greater involvement in their care plan and independently navigate telehealth technology. To view examples of patient handouts on subjects such as preparing for a successful visit and completing a self wound check, reference the “Patient Education - Successful TeleVisits for People with Wounds” topic.
CODING, COVERAGE AND REIMBURSEMENT
- Reference the “Reimbursement for Telemedicine Services in Wound Care” blog post for detailed information on CMS coding, coverage and reimbursement for telehealth services relevant to wound care.
CMS QUALITY MEASURES
- The implementation of telehealth services offers practices a unique opportunity to fulfill CMS quality measures requirements. Improvement Activities is one of four categories comprising CMS's Merit-based Incentive Payment System (MIPS), and completion is required for all MIPS-eligible providers who bill Medicare Part B. Telehealth can satisfy 2020 Improvement Activities requirements in two ways:
-
- Use of Telehealth Services that Expand Practice Access (IA_EPA_2): Use of telehealth services that expand practice access and analysis of data for quality improvement, such as participation in remote specialty care consults or teleaudiology pilots that assess ability to still deliver quality care to patients
- Implementation of Use of Specialist Reports Back to Referring Clinician or Group to Close Referral Loop (IA_CC_1): Use of specialist reports back to referring clinician/group to close a referral loop
- For more information, reference the “MIPS in Wound Care and Hyperbaric Medicine - Improvement Activities” blog post.
APPENDIX
Summary of Evidence (SOE)
|
SOE - For patients with chronic wounds under care of non-wound care specialist
Back to text
Systematic reviews and meta-analyses
- A 2020 systematic review and meta-analysis included 14 studies published between 2004 and 2019 (n=1926) that compared clinical outcomes in patients with chronic wounds of several etiologies who received telehealth interventions with patients who received usual care.[13] Most telehealth interventions were conducted between clinicians, utilizing interventions such as web-based systems, teleconsultation, telemonitoring, mobile application, telephone, text messaging, email. Authors found that compared with usual care, telehealth interventions significantly improved wound healing rate and reduced adverse events. No significant differences were found between patients allocated to the telemedicine group or usual care group, in terms of the outcomes of healing time, change in wound size, or mortality. Authors included several types of telehealth interventions in this meta-analysis, resulting in heterogeneity. With respect to the quality of the studies, authors reported publication bias, lack of patient/clinician blinding and allocation concealment.
- A 2020 systematic review and meta-analysis included 12 studies published between 2004 and 2019 (n=3913) that evaluated the efficacy and safety of telehealth for chronic wound management. [15] Telehealth interventions included mobile applications, specialized interactive systems, email, telephone, and videoconferencing. The 6 RCTs included in this systematic review and meta-analysis included patients with chronic wounds of several etiologies. Treating clinicians received advice from a remote wound care specialist via telehealth. Data showed no statistically significant difference in wound healing rates, mortality at 1 year, and a decreased risk of amputation in patients receiving telehealth (p=0.001). The result of cohort studies showed that telehealth was more effective than standard care (p<0.001).
- A 2019 systematic review included 6 studies published between 2000 and 2015 that evaluated the effectiveness of telehealth expert consultations delivered through real time audio and video, or image and/or record review in the treatment of patients with chronic wounds in the outpatient or post-acute settings.[8] RCTs included in this systematic review and meta-analysis included patients with chronic wounds of several etiologies. Authors concluded that there is moderate certainty evidence that telehealth interventions promote similar or better wound healing outcomes (i.e., healing rate, healing time) and result in fewer amputations.
- A 2017 systematic review and meta-analysis included 4 studies published between 2007 and 2015 (n=274 wounds) that evaluated the effectiveness of telemedicine for distant wound care advice in improving wound outcomes. [12] Interventions included electronic submission of digital images by home care nurses to remote wound care experts weekly or every 2 weeks in order to receive wound management instructions. Authors found that as compared with usual care, the telemedicine intervention significantly improved wound healing (p=0.02) in the combined trial of 3 studies evaluating wound healing rates (n=229). No significant differences were found between patients allocated to the telemedicine group or control group in the combined trial of 2 studies that evaluated change in wound size (n=205). Authors concluded that wound care telemedicine interventions could effectively improve wound healing rate but not change in wound size.
Review
- A 2016 comprehensive review and analysis of patients managed by the Home Hospital Wound Healing Network (CICAT) in Languedoc-Roussillon, France from 2005 to 2015 (n=5795) evaluated the clinical efficacy and efficiency of the “mobile wound healing center” model. [42] The telemedicine model included professional cooperation using teletransmission of data in the form of a store-and-forward system, and having the primary wounds (pressure ulcers, leg ulcers, and diabetic foot ulcers) analyzed by remote experts. Data showed a 72% reduction in hospitalizations and a 56% reduction in ambulance transfers to wound healing centers. Overall, 75% of wounds improved or healed. Authors concluded that The CICAT network is an example of the benefit of employing telemedicine in wound care, but noted that legal constraints and credentialing concerns may complicate implementation in other countries.
|
|
SOE - Telehealth for patients with lower extremity ulcers under the care of wound care specialists
Back to text
Systematic reviews, meta-analyses
- A 2017 systematic review and meta-analysis that included 2 studies published between 2004 and 2015 (n=514) evaluated whether telehealth consultations can be effective in diabetic foot patient care, compared to usual care. [34] Interventions included teleconsultations with patients from their homes. Patients in the telehealth group, as well as in the control group had statistically similar wound healing outcomes (i.e., healing time, unhealed ulcers) and amputations. Authors concluded that care delivered via telehealth consultations is promising for the management of diabetic foot patients as the results were comparable with usual care. The meta-analysis included 2 RCTs by Wilbright (2004) [43] and Rasmussen et al (2015) [44]. The Wilbright RCT was considered at high risk of bias, whereas Rasmussen’s RCT was considered at moderate risk of bias.
- A 2014 systematic review included one non-randomized study published in 2004 (n=140) that compared clinical outcomes in patients with leg ulcers and diabetes-related foot ulcers who received telemedicine follow-up with patients who received traditional follow-up. [45] The telemedicine intervention included real-time interactive video consultation, with or without digital image transfer, with a specialist nurse, physician and physiotherapist. Data showed no statistically significant difference in healing time, adjusted healing ratio and the number of ulcers at 12 weeks, and authors concluded that there is insufficient evidence to determine the efficacy of telemedicine follow-up for leg and foot ulcers. This review included the RCT by Wilbright (2004), considered at high risk of bias.[43]
Randomized Controlled Trials
- A 2020 cluster randomized controlled trial of adults with diabetes-related foot ulcers (DFUs) (n=182) compared ulcer healing time in patients receiving telemedicine follow-up care by a specialist healthcare professional with patients receiving standard outpatient care. [33] The telemedicine intervention included the submission of images by a community nurse to a specialist healthcare professional using a web-based ulcer record system accessible from mobile devices and computers. No significant differences were found in DFU treatment outcomes or patient-reported outcome measures. In both groups, measures of health, well-being and QOL remained relatively stable. Authors concluded that telemedicine was as effective as face-to-face care, and provided a greater reach.
- The Effect of Telemedicine Follow-up Care on Diabetes-Related Foot Ulcers: A Cluster-Randomized Controlled Noninferiority Trial [16]
- A randomized controlled trial comparing telemedical and standard outpatient monitoring of diabetic foot ulcers [44]
Cost analysis
- A 2018 cost minimization analysis evaluated the cost difference between a telemedicine and face-to-face combination model and a face-to-face only model in the treatment of lower extremity ulcers. [21] The telemedicine intervention consisted of consultation via a video conferencing system, with operation of a video camera by a nurse. Medical records were available to both the specialist and nurse throughout the session using an EMR database. Authors found a 7% higher cost per patient in the telemedicine modality compared to the same-room care; however, in a proportion similar to same-room care, the cost of telemedicine was lower. Additionally, compared to the combination model, the face-to-face only model demonstrated 30% higher costs. Authors concluded that the mixed method of treatment was less costly and the telemedicine implementation costs per patient may be lower than the face-to-face method in the case of an equal proportion of telemedicine and face-to-face patients.
|