CLINICAL
Overview
Background
DefinitionS
- Debridement is derived from the French word débridement, which means to remove a constraint.[1] The clinical definition of debridement relates to the process of removing necrotic, nonviable, dead tissue, and biofilm from pressure ulcers, burns, and other acute and chronic wounds to expose healthy tissue.[2][3] Removal of necrotic tissue may be conducted through several methods: selective (e.g. conservative sharp), non-selective (e.g. mechanical, enzymatic, autolytic or larval), or surgical.[2][3][4] Removal of biofilm is usually achieved through a combination of methods, which should include mechanical and/or sharp debridement and another method (e.g., antimicrobial agents). For clarification on each debridement method, see section below 'Types of Debridement'.
- Necrotic tissue varies in appearance and form, and often presents as slough or eschar [3]:
- Slough: brown, yellow, green or gray devitalized tissue that is moist, soft or fibrous, firmly or loosely adhered to the underlying tissue.
- Eschar: leathery brown or black dry crust on the wound
- Biofilm is a bacterial life form in which bacteria are organized into sessile aggregates, as opposed to as single, independent cells (planktonic form). Biofilm facilitates development of chronic infections that are often resistant to antibiotics and other conventional antimicrobial agents, and easily evades host defenses.[5] Biofilm may be present in almost 80% of chronic wounds.[6] Presence of extensive fibrinous slough may suggest the presence of biofilm, but in many cases, biofilms are located in deeper tissue layers in the wound, leading to difficulties in diagnosis and suboptimal care.[7]
Relevance
- Clinical perspective: debridement is one of the 3 main components of local wound care to prepare the wound bed for functional healing, together with inflammation/ infection control and moisture balance management.[8] Necrotic tissue poses a barrier to wound healing: it provides a potential nutrient source for bacteria, fostering inflammation and infection, it acts as a physical barrier to wound contraction and epithelialization, and it may prevent clinicians from making an accurate assessment of the wound.[3] Debridement (mechanical, sharp or surgical) is also required for biofilm removal, as bacteria is entrenched in deeper tissue layers.[7]
- Reimbursement perspective: several Medicare coverage determinations cite debridement as a pre-requisite for reimbursement. For instance:
- Dressings will only be covered when a qualifying wound is present. A qualifying wound is defined as :
- A wound caused by, or treated by, a surgical procedure; or,
- After debridement of the wound, regardless of the debridement technique.
- Hyperbaric oxygen therapy (HBOT) is covered as an adjunctive therapy for non-healing ulcers that have been treated with standard wound therapy for at least 30 days. Standard wound therapy includes debridement by any means to remove devitalized tissue.[9]
How it works
Debridement promotes normal healing by reducing bioburden, and removing biofilm and senescent cells.[1] At the cellular level, debridement interrupts the cycle of chronic inflammation and resets the level of proteases and cytokines to a level similar to that of an acute wound.[1][3]
General indications and contraindications
Indications
- Debridement may be indicated whenever necrotic tissue as well as cellular or proteinaceous debris are present on an open wound in order to keep the wound in an active state of healing.[10][4]
- Debridement may also be indicated in cases of abnormal wound healing or repair.[10][4]
Contraindications
Contraindications include:
- Dry, stable eschar on heels or in non-infected wounds, or dry gangrene. In such cases, it may be better to leave hardened eschar in place rather than remove it and create an open wound which might not heal. [3]
- Other contraindications are specific to each particular method of debridement.
Relative contraindications include:
- Bleeding disorders, use of anticoagulants
- Pyoderma gangrenosum: if debridement of pyoderma gangrenosum lesions is needed to reduce bacterial load or excessive necrotic debris, it should be limited to obvious nonviable tissue, in order to minimize trauma to the ulcer bed and minimize chances of pathergy (exarcerbation of pyoderma gangrenosum upon tissue injury).[11][12] See section on 'Local wound care' in "Pyoderma Gangrenosum - Treatment".
- Calciphylaxis: in this potentially fatal condition, often marked by ischemic ulcerations, the decision to debride depends on the goals of treatment. For wounds covered with dry, noninfected eschars, debridement is contraindicated. However, for healable wounds, or for exudative wounds, debridement associated with multidisciplinary interventions (e.g, parathyroidectomy, appropriate skin grafting or revascularization) can result in improved wound healing and limb salvage.[13][14]
Other considerations
- Timing of debridement: in certain conditions, debridement is indicated but timing plays an important role. For instance, for noninfected wounds caused by brown recluse spider bites, sharp conservative debridement is indicated once margins between necrotic and healthy tissue have been well defined, but not before that. If infection is present however, debridement should be performed immediately to prevent development of infection, which in worse cases may present as necrotizing fasciitis.[15] For acute burns, early surgical debridement (as early as 1 day post-injury) and skin grafting may improve outcomes. See section 'Surgical excision' in topic " Acute Burns - Treatment".
- Extrinsic boundaries influencing debridement-related decisions:
- Healthcare professionals' scope of practice: each clinician's scope of practice (as established by state licensure boards and facility policies) dictate which debridement methods can be performed by each clinician
- Skills and experience: each clinician has a duty to provide services that are safe and appropriate for each patient. Thus, debridement should only be performed if competency in the particular debridement method has been achieved.
- Collaboration with other care settings: for patients who will be referred to other care settings, consideration should be given in regards to the ability of the receiving care setting to continue care after a wound has been debrided, especially if multiple debridements are expected.
Types of debridement
Different debridement classification methods exist in literature (Video 1); this topic follows the classification adopted by Medicare coverage determinations. As such, debridement may be categorized as selective, non-selective or surgical (excisional).[16][10][17][18][19][20] Current Procedural Terminology (CPT) codes are listed in parentheses below. For more information on documentation requirements, see sections 'Documentation' and 'Medicare Administrative Contractors and Local Coverage Determinations' below.
Selective Debridement (CPTs 97597 and 97598, also known as conservative sharp wound debridement) includes:
- Removal of specific, targeted areas of devitalized or necrotic tissue from a wound along the margin of viable tissue by high-pressure waterjet with/without suction, sharp debridement/dissection utilizing scissors, scalpel, curettes, and/or tweezers/forceps. This procedure typically requires no anesthesia and generally has no or minimal associated bleeding. Debridement with Pulsed Lavage Irrigation (e.g.,Versajet* II Hydrosurgery System, Jetox-ND, etc) is included in this modality. See topics "How to Perform Conservative Sharp Wound Debridement" and "State-by-State Regulations on Conservative Sharp Debridement by Nurses in the United States".
Non-Selective Debridement (CPT 97602) is usually a bundled code and includes:
- Mechanical Debridement: this type of debridement is the removal of necrotic tissue by cleansing, or application of a wet-to-dry or dry-to-dry dressing technique. Wet-to-dry dressings should be used judiciously as maceration of surrounding tissue may hinder healing. Generally, dressing changes are not considered a skilled service. Mechanical debridement is also accomplished through products with monofilament fiber (e.g., pads, lolly). Low-frequency ultrasound (e.g., UltraMIST) is also used for mechanical debridement, but this modality has its own CPT code (97610).
- Enzymatic Debridement: in the U.S., clostridial collagenase ointment (CCO) is the only FDA-approved enzymatic debriding agent. CCO cleaves denatured collagen in seven different areas of the collagen strand that anchors devitalized tissue to the wound bed and breaks down necrotic tissue. The manufacturer’s product insert contains indications, contraindications, precautions, dosage and administration guidelines; it is the clinician’s responsibility to comply with those guidelines.
- Autolytic Debridement: this type of debridement is indicated where manageable amounts of necrotic tissue are present, and there is no infection. Clinically, autolytic debridement is regarded as the most selective debridement method and the method that takes the longest to work.[21] From a medical coding standpoint however, autolytic debridement is considered a non-selective debridement (CPT 97602).[22] Autolytic debridement can be achieved with hypertonic saline, Manuka honey, hydrogel, hydrocolloids, and transparent film, and occurs when the enzymes that are naturally found in wound fluids are sequestered under occlusive or semi-occlusive synthetic dressings. Autolytic debridement depends on enzymes from the patient, but patients with comorbidities and poor nutrition may have lower levels of enzymes, delaying the autolytic process. Autolytic debridement is contraindicated for infected wounds. For information on which dressings can promote autolytic debridement, see topic "Dressing Essentials".
- Maggot / larvae therapy (biological) : debridement with medical-grade maggots in wounds
Surgical (Excisional) Debridements (CPT codes 11000-11012 and 11042-11047)
- Surgical debridement occurs only if material has been excised, and tissue has been removed at the wound margin or at the wound base until viable tissue is exposed. Indications include presence of large amounts of necrosis, eschar, slough, infected tissue, biofilm, abnormal granulation tissue. Surgical (excisional) debridement may be complex in nature and may require use of anesthesia.
- For billing purposes, medical coders report surgical debridement codes based on the deepest layer of viable tissue removed (e.g., skin, subcutaneous tissue, muscle, etc) and not extent, depth, or grade of the ulcer or wound.[10][23]
- For example, CPT code 11042 defined as “debridement, subcutaneous tissue” should be used if only necrotic subcutaneous tissue is debrided, even though the ulcer or wound might extend to the bone. In addition, if only fibrin is removed, this code would not be billed.[10]
- As another example, when only biofilm on the surface of a muscular ulceration is debrided, then codes 97597-97598 would be appropriate. If muscle substance was debrided, then the 11043-11046 series would be appropriate, depending on the area.[10]
- Specific documentation must mention either:
- Bleeding tissue
- Removal/exposure of viable tissue at margin or wound base or
- Increasing wound size by width, length, or depth
- Place of service: For certain Medicare Administrative Contractors (MAC), CPT code 11043, 11046 and 11044, 11047 may only be billed in place of service inpatient hospital, outpatient hospital or ambulatory surgical center (ASC), as those describe deep debridement of bone and muscle.[17] For others, those CPT codes can be performed in a variety of settings (e.g. physicians’ offices, outpatient facilities, nursing facilities or skilled nursing facilities, inpatient hospitals and custodial care facilities).[24]
Video 1. Debridement Types - Overview (excerpt from Webinar "Wound Care Basics Part 2. Managing Chronic Wounds")
Evidence and Recommendations
- 1CIn general, for healable chronic wounds without contraindications, we recommend debridement as opposed to no debridement to promote wound healing (Grade 1C)
- Rationale: There is consensus in the wound care literature that debridement is necessary to promote wound healing [25][26][27], however current evidence is limited due to the lack of randomized controlled trials (RCTs) comparing debridement versus no debridement to promote wound healing.[28][29][30] Nevertheless, historic clinical experience and other studies suggest that active debridement removes obvious necrotic tissue and excessive bacterial burden that can slow down the healing process and increase the risk of osteomyelitis and sepsis.[31][32] Undertaking RCTs comparing debridement with no debridement could represent a step backward in wound management and could be interpreted as unethical, given clinically proven benefits of debridement.[28]
A summary of condition-specific evidence-based recommendations is provided below. Please refer to their respective topics for rationale, summary of evidence and considerations on each debridement method.
Venous Ulcers
Please see section on ‘Debridement' in "Venous Ulcers - Treatment" for rationales and summary of evidence supporting the recommendations below.
- 1CFor healable venous ulcers (VLUs) without contraindications, we recommend debridement (vs. no debridement) at initial assessment and during subsequent visits as needed (Grade 1C).
2C
When choosing debridement methods for VLU patients, we suggest clinicians consider factors such as status of the wound, health care provider's familiarity with each technique, overall condition of the patient, professional licensing restrictions, patient preference and insurance coverage (Grade 2C). For considerations when selecting debridement methods for VLUs, see ‘Debridement' in "Venous Ulcers - Treatment" .
Diabetic Foot Ulcers
Please see section on ‘Debridement' in "Diabetic Foot Ulcers - Treatment" for rationales and summary of evidence supporting the recommendations below.
- 1BTo promote diabetic foot ulcer (DFU) healing, we recommend debridement over no debridement of devitalized tissue and surrounding callus for healable DFUs without contraindications at initial assessment and for maintenance, at intervals dependent on the production rate of exudate and devitalized tissue (usually 1-4 weeks) (Grade 1B)
- For non-healable or maintenance wounds, expert opinion suggests against active aggressive debridement.[33]
- 22CAs for debridement techniques for healable DFUs, given the lack of sufficient evidence for superiority of any specific method, we suggest initial sharp debridement, followed by debridement method(s) that encourage patient adherence to the care plan (Grade 2C). For considerations when selecting debridement methods for DFUs, see ‘Debridement' in "Diabetic Foot Ulcers - Treatment" .
Pressure Ulcers/ Injuries
Please see section on ‘Debridement' in "Pressure Ulcers/ Injuries - Treatment" for rationales and summary of evidence supporting the recommendations below.
- 1CFor healable, Stage 2 - 4 pressure ulcers/ injuries (PUs/PIs), we recommend debridement over no debridement of devitalized tissue to promote wound healing, when aligned with goals of therapy and not contraindicated (Grade 1C)
- For PU/PI on lower extremities: do not debride ulcer if blood supply to the wound is not adequate enough to support healing post debridement.[34]
- For non-healable or maintenance wounds, guidelines recommend against active aggressive debridement.[35][34]
- 2CAs for choice of debridement for healable PUs/PIs, clinicians can opt from several methods (e.g., surgical, sharp, mechanical - including ultrasound and hydrosurgical, enzymatic, autolytic, biologic) according to patient's condition, wound bed, resources and clinical setting (Grade 2C).[34][36] For considerations when selecting debridement methods for PUs/PIs, see ‘Debridement' in "Pressure Ulcers/ Injuries - Treatment".
Acute Burns
Please see section on ‘Debridement' in "Acute Burns - Treatment".
Risks
Each debridement method has its own associated risks, but in general, risks include bleeding, infection, pain, unintentional injury of underlying structures (e.g., tendons, nerves, vessels).
How to select debridement methods
In light of the paucity of high certainty RCTs supporting superiority of any specific debridement method, clinicians should consider factors such as the patient's condition, wound bed characteristics, available resources, cost-effectiveness, clinical setting, clinical competency, scope of practice, and experience with each method.[37][29] To guide decision making for specific conditions, see topics listed above in "Evidence and Recommendations". A separate topic with indications, pros and cons for each method will be available soon.
How to perform debridement
See topic " How to Perform Conservative Sharp Wound Debridement". Other topics with protocols and step-by-step instructions and videos will be available soon.
Prescribing/ ordering
Ordering requirements for each debridement method vary according to the payor's or MAC's determinations and policies. In general, selective debridement and surgical (excisional) debridement require a specific order of a physician and/or qualified healthcare professional.[17] Some agents used for other non-selective debridement methods require a prescription (e.g., collagenase).
Documentation requirements
To ensure optimal patient care coordination, smooth insurance reimbursement process and audit readiness, clinicians should strive for optimal documentation on medical records. For Medicare beneficiaries, clinicians should follow Local Coverage Determinations (LCD) provided by their state’s Medicare Administrative Contractor (MAC) and/or National Coverage Determinations. See section ‘Coding, Coverage, Reimbursement’.
Medical records documentation requirements may vary across MACs, so make sure to confirm with your MAC or MAC’s LCD. Listed below are documentation requirements compiled from existing LCDs and policies. All documentation must be maintained in the patient’s medical record and made available to the contractor upon request:
The patient’s medical record should include but is not limited to [19]:
- Initial assessment: the assessment of the patient by the ordering provider as it relates to the complaint of the patient for that visit,
- Relevant medical history
- The patient's comorbid medical and mental condition, and all health factors that may influence the patient's ability to heal tissue, such as, but not limited to the following: mental status, mobility, infection, tissue oxygenation, chronic pressure, arterial insufficiency/small vessel ischemia, venous stasis, edema, type of dressing, chronic illness such as diabetes mellitus, uremia, COPD, malnutrition, CHF, anemia, iron deficiency, and immune deficiency disorders.[38]
- Results of pertinent tests/procedures
- Identification of the wound location, size, depth and stage either by description and/or a drawing or photograph. [38][39]
- A description of the type(s) of tissue involvement, the severity of tissue destruction, undermining or tunneling, necrosis, infection or evidence of reduced circulation. If infection has developed, the patient's response to this infection should be described.[38]
- Photographic documentation of wounds either immediately before or immediately after debridement is recommended for prolonged or repetitive debridement services (especially those that exceed five extensive debridements per wound (CPT code 11043 and/or 11044). If the provider is unable to use photographs for documentation purposes, the medical record should contain sufficient detail to determine the extent of the wound and the result of the treatment. [38][17][39]
- Initial treatment plan: to include the expected frequency and duration of the skilled treatment and the potential to heal. Continuation of treatment plan with ongoing evidence of the effectiveness of that plan, including diminishing area and depth of the ulceration, resolution of surrounding erythema and /or wound exudates, decreasing symptomatology, and overall assessment of wound status (such as stable, improved, worsening, etc). Appropriate changes in the ongoing treatment plan to reflect the clinical presentation must be present in the record.[38][17]
- The documentation must include that if indicated, ongoing pressure relief has been prescribed, for example, shoe inserts, modifications, padding, frequent position changes, etc. and monitoring is occurring. [38]
- Operative report for the debridement service (Please note that all services ordered or rendered to Medicare beneficiaries must be signed and dated).[38][17][39][4][40]
- Medical diagnosis.
- Indication(s) and medical necessity for the debridement.
- Type of anesthesia used, if and when used.
- Wound characteristics such as diameter, depth, undermining or tunneling, color, presence of exudates or necrotic tissue.
- Level/depth of tissue debrided and a description of the types(s) of tissue involved and the tissue(s) removed (i.e., skin, full or partial thickness; subcutaneous tissue; muscle and/or bone).
- Vascular status, infection, or evidence of reduced circulation.
- Narrative of the procedure to include the instruments used (i.e. forceps, scalpel, scissors, tweezers, high-pressure water jet, etc.).
- Debridement procedure notes must demonstrate tissue removal (i.e., skin, full or partial thickness; subcutaneous tissue; muscle and/or bone), the method used to debride (i.e., hydrostatic, sharp, abrasion, etc.) and the character of the wound (including dimensions, description of necrotic material present, description of tissue removed, degree of epithelialization, etc.) before and after debridement.
- Documentation must support the use of skilled personnel with the use of jet therapy and wound irrigation for wound debridement. [39]
- Selective debridement (CPTs 97597 and 97598):
- Clear description of instruments used for debridement (i.e. high-pressure waterjet, scissors, scalpel, forceps).
- Thorough objective assessment of the wound including drainage, color, texture, temperature, vascularity, condition of surrounding tissue, and size of the area to be targeted for debridement
- See 'Conservative Sharp Wound Debridement Documentation Checklist and Template' in topic "How to Perform Conservative Sharp Wound Debridement".
- Non-Selective debridement (CPT 97602) :
- Type of technique utilized (i.e., wet-to-moist, enzymatic, abrasion, autolytic
- Thorough objective assessment of the wound as described in Selective debridement above
- Patient specific goals and/or response to treatment.
- Immediate post-op care and follow-up instructions.
- The presence or absence of necrotic, devitalized, fibrotic, or other tissue or foreign matter must be documented in the medical record when wound debridement is performed.
- A pathology report substantiating depth of debridement is encouraged when billing for the debridement procedures involving deep tissue or bone.[39]
- Follow-up visit notes: The patient’s medical record must contain clearly documented evidence of the progress of the wound's response to treatment at each visit. This documentation must include, at a minimum [17][39][4]
- Current wound volume (surface dimensions and depth).
- Presence (and extent of) or absence of obvious signs of infection.
- Presence (and extent of) or absence of necrotic, devitalized or non-viable tissue
- Other material in the wound that is expected to inhibit healing or promote adjacent tissue breakdown.
- With continuation of a treatment plan, there needs to be ongoing evidence of the effectiveness of the plan, including diminishing area and depth of the ulceration, resolution of surrounding erythema and /or wound exudates, decreasing symptomatology, and overall assessment of wound status (such as stable, improved, worsening, etc.) documented.
- Plan reassessment: appropriate modification of treatment plans, when necessitated by failure of wounds to heal, must be demonstrated. A wound that shows no improvement after 30 days may require a new approach. Documentation of such cases may include a physician reassessment of underlying infection, metabolic, nutritional, or vascular problems inhibiting wound healing, or a new treatment approach. [39]
- Appropriate evaluation and management of contributory medical conditions or other factors affecting the course of wound healing (such as nutritional status or other predisposing conditions) should be addressed in the medical record at intervals consistent with the nature of the condition or factor.[39]
- In cases of excessive frequency or prolonged duration of treatment, documentation should include an evaluation for possible infection (e.g. culture and sensitivity), osteomyelitis (e.g. x-ray), and treatment of any infection by antibiotics. Any other conditions that may significantly affect wound healing should also be appropriately addressed in the medical record.[38]
- Documentation for low frequency, non-contact, non-thermal ultrasound (MIST Therapy) services should include documented improvements of pain reduction, reduction in wound size, improved and increased granulation tissue, or reduction in necrotic tissue. The services should be medically necessary based on the provider’s documentation of a medical evaluation of the patient's condition, diagnosis, and plan.[39]
CODING, COVERAGE AND REIMBURSEMENT
Medicare Administrative Contractors and Local Coverage Determinations
Medicare coverage of provider and facility fees related to debridement is managed by Medicare Administrative Contractors (MAC), under Medicare Part A or Part B. Each jurisdiction may have its own specific local coverage determination and policies, as follows
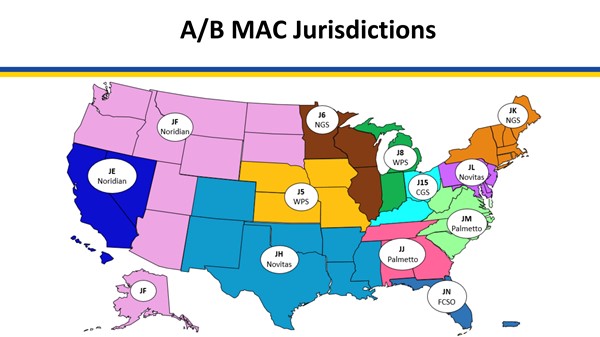
| Medicare Administrative Contractor | Coverage Determinations and Articles (click on reference, then on "View source site") |
Noridian
| - (Jurisdiction J-E) Wound Care & Debridement – Provided by a Therapist, Physician, NPP or as Incident-to Services (A53296) [16]
- (Jurisdiction J-F) Wound Care & Debridement – Provided by a Therapist, Physician, NPP or as Incident-to Services (A53046) [40]
- Local Coverage Article: Billing and Coding: Wound and Ulcer Care (A58565) [41]
- Local Coverage Article: Billing and Coding: Wound and Ulcer Care (A58567) [42]
- Local Coverage Determination (LCD): Wound and UIcer Care (L38902) [43]
- Local Coverage Determination (LCD): Wound and UIcer Care (L38904) [44]
- Response to Comments: Wound and Ulcer Care (A58903) [45]
|
| Novitas | - Local Coverage Article: Billing and Coding: Wound Care (A53001) [10]
- Local Coverage Determination (LCD): Wound Care (L35125) [4]
|
| WPS | - Local Coverage Determination (LCD): Wound Care (L37228) [46]
- Local Coverage Article: Billing and Coding: Wound Care (A55909) [17]
- Local Coverage Article: Response to Comments: Wound Care (DL37228) (A55910) [47]
- Local Coverage Article: Response to Comments: DL37228 Wound Care (A57846) [48]
|
| NGS | - Local Coverage Determination (LCD): Debridement Services (L33614) [49]
- Local Coverage Article: Billing and Coding: Debridement Services (A56617) [18]
|
| CGS | - Local Coverage Determination (LCD): Debridement Services (L34032) [38]
- Local Coverage Article: Billing and Coding for Debridement Services (A56459) [19]
|
| Palmetto | - Local Coverage Determination (LCD): Outpatient Occupational Therapy (L34427) [50]
- Local Coverage Determination (LCD): Outpatient Physical Therapy (L34428) [51]
|
| FCSO | - Local Coverage Article: Wound Care Coding Guidelines (A55818) [20]
- Local Coverage Determination (LCD): Wound Care (L37166) [39]
|
Each MAC may have its own variations, so it is recommended that clinicians check the LCDs and Articles above. A summary, which may or may not be applicable to your MAC is provided below for convenience:
Frequency limitations
- Wound care must be performed in accordance with accepted standards for medical and surgical treatment of wounds. The appropriate interval and frequency of debridement depends on the individual clinical characteristics of the patient and the extent of the wound. The extent and number of services provided should be medically necessary and reasonable based on the documented medical evaluation of the patient's condition, diagnosis, and plan.[10]
- With the above in mind, only a minority of beneficiaries who undergo debridements for wound care appear to require more than eight total surgical excisional debridement services involving subcutaneous tissue, muscle/fascia, or bone in a 360 day period, (five debridements of which involve removal of muscle/fascia, and/or bone) in order to accomplish the desired objective of the treatment plan of the wound. Only when medical necessity continues to be met and there is documented evidence of clear benefit from the debridements already provided, should debridement services be continued beyond this frequency or time frame.[10]
- When utilized, it is expected that the frequency of debridement will decrease over time. [10]
Non-coverage
- The following procedures are considered part of an E/M service and are not separately covered when an E/M service is performed:
- Removal of necrotic tissue by cleansing and dressing, including wet or dry-to-dry dressing changes,
- Cleansing and dressing small or superficial lesions, and
- Removal of coagulated serum from normal skin surrounding an ulcer.
The following services are considered to be not reasonable and necessary wound debridement services [10]:
- Removal of necrotic tissue by cleansing or dry-to-dry or wet-to-dry dressing.
- Washing bacterial or fungal debris from lesions.
- Removal of secretions and coagulation serum from normal skin surrounding an ulcer.
- Dressing of small or superficial lesions.
- Paring or cutting of corns or non-plantar calluses.
- Incision and drainage of abscess including paronychia, trimming or debridement of mycotic nails, avulsion of nail plates, acne surgery, or destruction of warts.
- Removal of non-tissue integrated fibrin exudates, crusts, or other materials from a wound without removal of tissue does not meet the definition of any debridement code and may not be reported as such.
Surgical debridement will be considered not reasonable and necessary when documentation indicates the wound is without devitalized, fibrotic, nonviable tissue, infection, necrosis, foreign matter, or if the wound has pink to red granulated tissue. When utilized, it is expected that the frequency of debridement will decrease over time. The routine application of a topical or local anesthetic does not elevate active wound care management to surgical debridement. [10]
CPT® Codes
- 11000 Debride infected skin
- 11001 Debride infected skin add-on
- 11004 Debride genitalia & perineum
- 11005 Debride abdom wall
- 11006 Debride genit/per/abdom wall
- 11008 Remove mesh from abd wall
- 11010 Debride skin at fx site
- 11011 Debride skin musc at fx site
- 11012 Deb skin bone at fx site
- 11042 Deb subq tissue 20 sq cm/<
- 11043 Deb musc/fascia 20 sq cm/<
- 11044 Deb bone 20 sq cm/<
- 11045 Deb subq tissue add-on
- 11046 Deb musc/fascia add-on
- 11047 Deb bone add-on
- 97610 Low frequency non-thermal us
- 97602 Removal of devitalized tissue from wound(s), non-selective debridement, without anesthesia
- 97597 Deb (e.g, high pressure waterjet with / without suction, sharp selective debridement with scissors, scalpel and forceps), open wound (e.g. fibrin, devitalized epidermis and/or dermis, exudate, debridement, biofilm), including topical application(s), wound assessment, use of a whirlpool, when performed and instruction(s) for ongoing care, per session, total wound(s) surface area, first 20 SQ CM or Less.
- 97598 Deb (e.g, high pressure waterjet with / without suction, sharp selective debridement with scissors, scalpel and forceps), open wound (e.g. fibrin, devitalized epidermis and/or dermis, exudate, debridement, biofilm), including topical application(s), wound assessment, use of a whirlpool, when performed and instruction(s) for ongoing care, per session, total wound(s) surface area, each additional 20 SQ CM, or part thereof (list separately in addition to code for primary procedure)